
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 5
Improvement of graphene induced abdominal distension with melena, nephropathy by graphene exfoliator NaCl + KCl solution
*Corresponding Author : Chur Chin
Department of Emergency Medicine, New life Hospital Bokhyun-dong, Bukgu, Daegu, Korea.
Email: gemcitabinecisplatin@nate.com
Received : Dec 05, 2023
Accepted : Jan 17, 2024
Published : Jan 24, 2024
Archived : www.jcimcr.org
Copyright : © Chin C (2024).
Citation: Chin C. Improvement of graphene induced abdominal distension with melena, nephropathy by graphene exfoliator NaCl + KCl solution. J Clin Images Med Case Rep. 2024; 5(1): 2816.
Description
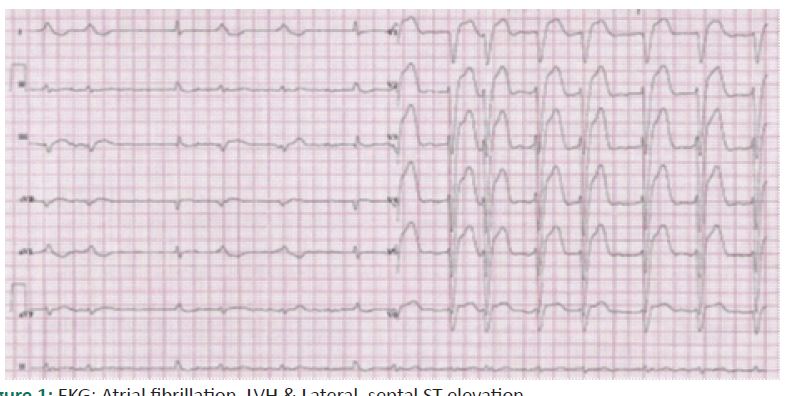
A 63-year-old man with right corona radiata infarct presented to our hospital with a history of abdominal distension, 500 cc melena, vital signs: Blood pressure 90 (systolic)/60 (diastolic), heart rate 90, total leukocyte count of 11500/cmm, hemoglobin 11.3 g/dl, platelet 414000/ μl, stool occult blood: Positive, a prothrombin time 15.5 sec (normal range: 10-15), Blood Urea Nitrogen (BUN) 41.7 mg/dL, Creatinine (Cr) 2.28 mg/dL, serum sodium/potassium/chloride 137/4.9/108 nmol/L, aspartate transaminase and alanine transaminase 45 IU/L and Erythrocyte Sedimentation Rate (ESR) 40 mm in the first hour using Westergren method. The intravenous infusion of a solution consisting of 250 mL normal saline over 6h for 3 days with supportive care resulted in recovery of the symptoms with BUN/Cr 22.8/1.69 mg/dL, platelet 264000/ μl with negative stool blood [1-7]. Ischemic bowel disease is due to inadequate oxygenated blood supply to the bowel walls. Ischemic bowel disease includes acute and chronic mesenteric ischemia affecting the small bowel and colon ischemia with embolism, arterial or venous thrombosis. Embolism to the visceral vessels is the most common cause of mesenteric ischemia. Atrial Fibrillation (AF) is a risk factor for ischemic bowel disease in patients with atrial fibrillation. AF-related irregular heart rhythm may predispose to hypoperfusion and ischemia of the bowel walls. CT findings of the ischemic bowel disaese emcompass the presence of pericolic fluid was found in the acute phase and bowel wall thickening in the subacute phase [8].

References
- Chin C. Comparison of 50 Cases of the Anti-Cancer Effects of NaCl with KCl as a Potent Graphene Exfoliator, Prehydrated Patients to NaCl-Only Prehydrated Patients on the Terminal Stage Cancer Patients. Case Reports in Clinical Medicine. 2023; 12: 425-431.
- Chin C. Changes in electrocardiogram after intramuscular injection of graphene using salt- intercalation exfoliation, J Clin Exp Cardiol. 2023; 14: 1-15.
- Chin C. Cell entry inhibitor with sulfonated colloid gold as new potent broad spectrum virucides. J Infect Dis Ther. 2021; 9: 1-4.
- Chin C. The Anti-Inflammatory Effects of NaCl with KCl as a Potent Graphene Exfoliator in a Patient with Guillaine-Barré Syndrome and Facial Nerve Palsy, Case Reports in Clinical Medicine. 2023; 12: 447-451.
- Chin C. Improvement of renal functions, graphene-induced rapid progression of prediabetes in an elderly woman with arthritis by graphene-exfoliator NaCl with KCl solution, 3 cases, Journal of Clinical Images and Medical Case Reports. 2023; 4: 1-3.
- Chin C. Improvement of graphene induced pulmonary edema by graphene exfoliator NaCl with KCl solution, Journal of Clinical Images and Medical Case Reports. 2023; 4: 4-5.
- Chin C. The anti-inflammatory effects of NaCl with KCl as a potent graphene exfoliator in a patients with interstitial pneumonia by epithelial-mesenchymal transition, Journal of Clinical Images and Medical Case Reports. 2023; 4: 36-37.
- Francesca Iacobellis, Daniela Berritto, Dominik Fleischmann, Giuliano Gagliardi, Antonio Brillantino, et al. CT Findings in Acute, Subacute, and Chronic Ischemic Colitis: Suggestions for Diagnosis, Biomedical Research International. 2014; 895248: 1-7.