
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Report - Open Access, Volume 5
Pulmonary actinomycosis masquerading as lung cancer
Mengning Zheng1; Yonggang Wei2; Niyati A Borkar3; Xinyan Yang4; Xinni Wang4*
1Department of Respiratory and Critical Care Medicine, Guizhou Provincial People’s Hospital, Guiyang, Guizhou, China.
2Department of Neurology, Gaozhou People’s Hospital, Gaozhou, Guangdong, China.
3Department of Anesthesiology and Perioperative Medicine, Rochester, MN, USA.
4Department of Respiratory Disease, Guangzhou Institute of Respiratory Health, the First Affiliated Hospital of Guangzhou Medical University, Guangzhou, Guangdong, China.
*Corresponding Author : Xinni Wang
Department of Respiratory Disease, Guangzhou Institute of Respiratory Health, the First Affiliated Hospital of Guangzhou Medical University, Guangzhou, Guangdong, China.
Email: 3929544042@139.com
Received : Nov 17, 2023
Accepted : Jan 18, 2024
Published : Jan 25, 2024
Archived : www.jcimcr.org
Copyright : © Wang X (2024).
Abstract
Pulmonary actinomycosis is a rare chronic purulent granulomatous disease, which can be easily misdiagnosed as lung cancer, tuberculosis, and other diseases. However, diagnosis relies on histopathological evidence, and early diagnosis is conducive to the patient’s recovery. In this study, a case of a 70-year-old man with a soft tissue density mass at the right lower lung was studied, with initial chest CT suggesting lung cancer, pulmonary actinomycosis was confirmed by subsequent pathological biopsy of lung tissues eventually. The patient responded well to antibiotics treatment. This paper is to explore the clinical characteristics of the disease, providing insight into the disease, and its diagnosis and treatment.
Keywords: Actinomycosis; Lung neoplasms.
Citation: Zheng M, Wei Y, Borkar NA, Yang X, Wang X. Pulmonary actinomycosis masquerading as lung cancer. J Clin Images Med Case Rep. 2024; 5(1): 2818.
Case report
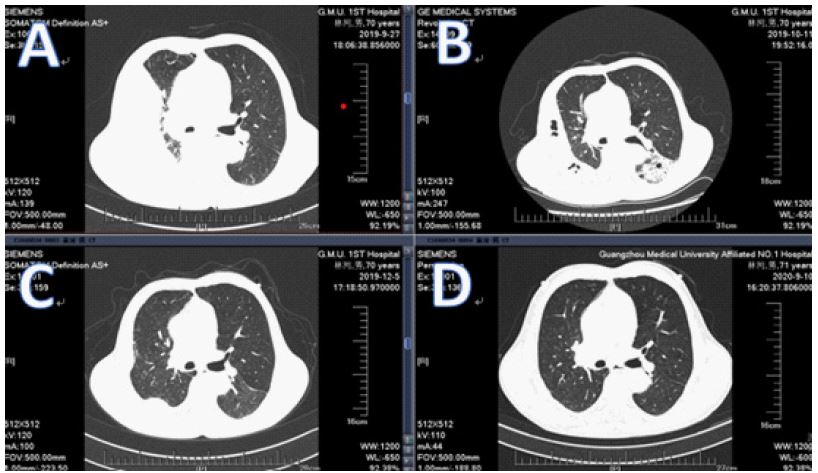
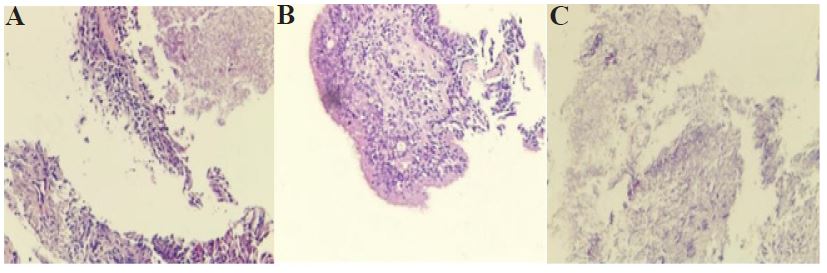
A 70-year-old male, currently a smoker, who was considered for lung cancer in another hospital, was admitted to the Department of Guangzhou Institute of Respiratory Diseases and Health, 1st Affiliated Hospital of Guangzhou Medical University, for 4 months due to recurrent cough and sputum, with an aggravation of 1 week. In chest CT, an area of lung consolidation about 35x24 mm was found in the lower part of the right hilus. In contrast-enhanced scan, there was significant enhancement with a slightly less enhanced mass shadow inside, with right pleural effusion (Figure 1A). Additionally, several enlarged lymph nodes were also observed in the mediastinum and right lung hilus. During hospital stay, both lung lesions progressed on review chest CT after broad-spectrum antibiotic treatment (Figure 1B). Because of clinical and radiological picture arousing oncology vigilance, an ultrasound-guided lung biopsy was performed. Afterward, the bronchoaspirate was taken for microbiological examination, with no neoplastic tissue in a pathology test. However, colonies of microorganisms morphologically corresponding to actinomyces were found within purulent masses, with sulfur particles (Figures 2A, 2B and 2C), with positive gram stain, GMS, and PAS. Treatment was initiated with penicillin G at a dose of 720 units/day for 2 months. During the initial intravenous antibiotic treatment, cough and sputum subsided, and the well-being of the patient has been significantly improved. According to chest CT reexamined in outpatient, there was a reduction in the partial consolidation of right lung, as well as a significant reduction in the enveloped pleural effusion on right. Then, the patient was switched to penicillin G on an outpatient basis for 6 months. And about 2 months of treatment later, CT scan showed that the lesion in the right lung was significantly reduced, and the lesion was largely absorbed after 1 year (Figures 1C and 1D).
Discussion
Pulmonary actinomycosis is a rare chronic purulent granulomatous disease triggered by actinomycetes, which is more prevalent in middle-aged and young people, with common symptoms, such as cough, sputum, fever, and hemoptysis, but no typical clinical symptoms. The disease can induce the local formation of a purulent fistula, which may discharge pus containing “sulfur particles” as a typical manifestation of the disease. However, it is not a specific manifestation [1]. Masquerading as lung cancer, tuberculosis, and other diseases [2]. Actinomycetes are anaerobic or micro-aerobic gram-positive bacteria that are branched, acid-resistant, with fungal properties. Known as actinomycetes because of their radial arrangement of hyphae, they are generally colonized in healthy people, such as oral, digestive tract, reproductive tract, and other parts [3]. Diabetes, alcoholism, oral problems, and respiratory diseases are risk factors for this disease [4]. In this case, the patient studied had poor oral hygiene as he was a smoker with alcohol drinking. Thus, the cause of the disease could be attributed to the obstruction of lung mass, resulting in the formation of a local hypoxic environment. In patients with bacterial infections, bacterial inflammation may trigger hypoxic environments that favor the growth of actinomyces.
At present, the main long-term treatment of actinomycosis was high dose intravenous injection of penicillin. And, although treatment varies from person to person, in general, 18-24 million units of penicillin are administered daily for 2-6 weeks, with oral penicillin (or amoxicillin) for 6-12 months [5]. For people allergic to penicillin, tetracycline and erythromycin can be used as an alternative treatment.
Conclusion
To sum up, pulmonary actinomycosis is relatively rare in clinical practice. For patients with history of smoking, poor oral hygiene, diabetes, and other chronic basic diseases, imaging examination suggests the presence of pulmonary consolidation or space-occupying lesions, and attention should be paid to the differential diagnosis of pulmonary actinomycosis. At the same time, the diagnosis of pulmonary actinomycosis requires pathological examination, and bronchoscopic biopsy and percutaneous lung puncture biopsy are the preferred treatment options [6]. Currently, new-generation metagenomic sequencing (MNGS) is a new molecular technology, which is highly sensitive and independent of culture, to assist the accurate diagnosis of this disease [7]. Early diagnosis, as well as early and correct treatment, can reduce mortality rate and teratogenic rate of the disease [8].
Declarations
Funding: This study was supported by the Science and Technology Program of Guizhou ZK [2021]-351 (M.Z.) and Traditional Chinese Medicine Management in Guizhou qzyyxg-2020-9 (M.Z.)
Author contributions: Conceived and designed the article: M.Z., Y.W, and P.R. Collect case information: X.Y,X.W. Contributed to writing manuscript: M.Z., Y.W,N.B. All the authors approved the submission of the manuscript for publication.
Competing financial interests: The authors declare no competing financial interests.
Acknowledgment: The authors thank Nuofu Zhang for providing valuable suggestions.
Our study was approved by the medical ethics committee of the First Affiliated Hospital of Guangzhou Medical University.
References
- Zhang M, Zhang X Y, Chen Y B. Primary pulmonary actinomycosis: a retrospective analysis of 145 cases in mainland China[J]. Int J Tuberc Lung Dis, 2017, 21(7): 825-831.
- Mabeza G F, Macfarlane J. Pulmonary actinomycosis[J]. Eur Respir J, 2003, 21(3): 545-51.
- Sullivan D C, Chapman S W. Bacteria that masquerade as fungi: actinomycosis/nocardia[J]. Proc Am Thorac Soc, 2010, 7(3): 216-21.
- Takiguchi Y, Terano T, Hirai A. Lung abscess caused by Actinomyces odontolyticus[J]. Intern Med, 2003, 42(8): 723-5.
- Cheon J E, Im J G, Kim M Y, et al. Thoracic actinomycosis: CT findings[J]. Radiology, 1998, 209(1): 229-33.
- Ge M J, Fu Y Q, Zhou H, et al. [Clinical feature analysis of 30 cases with pulmonary actinomycosis][J]. Zhonghua Yi Xue Za Zhi, 2019, 99(46): 3617-3621.
- Wang W, Ren D, Xu C, et al. Pulmonary actinomycosis diagnosed by radial endobronchial ultrasound coupled with metagenomic next-generation sequencing: A case report and brief literature review[J]. Int J Infect Dis, 2020, 100: 379-381.
- Newsom B D, Hardy J D. Pulmonary fungal infection. Survey of 159 cases with surgical implications[J]. J Thorac Cardiovasc Surg, 1982, 83(2): 218-26.