
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Report - Open Access, Volume 5
Unidigital severe lichen planus vulgaris: “Tincture of timing”
Revathi K, MD, DVL*; Rajesh Rajagopalan, MD, DNB, MNAMS
Department of Skin, STDs and Leprosy, Government Erode Medical College Hospital, Perundurai, Erode, Tamilnadu, South India.
*Corresponding Author : Revathi K, MD, DVL
Assistant Professor, Department of Skin, STDs and Leprosy, Government Erode Medical College Hospital, Perundurai, Erode, Tamilnadu, South India.
Email: gemchskin@gmail.com
Received : Nov 18, 2023
Accepted : Jan 18, 2024
Published : Jan 25, 2024
Archived : www.jcimcr.org
Copyright : © Revathi K (2024).
Abstract
Background: Lichen Planus is a multifaceted muco-cutaneous auto immune inflammatory disease of multiplex etiopathogenesis. Nail involvement is seen in up to 10-15% of patients. Most cases are mild, and serious consequences may occur due to swift progression of the disease, the high risk of scarring, and resulting in permanent damage to the nail architecture (4-12%).
Case presentation: We report a 32 year old male patient with nail lichen planus affecting only the right thumb nail which has gradually improved with topical steroid and calcineurin inhibitors.
Conclusion: We report this case to draw the attention to the necessity of tincture of timing (watchful waiting) in majority of the cases which may subside or improve with first line of drugs and to avoid the systemic side effects of immunosuppressives in the long run. Onchyscopy often confirm the diagnosis as a non-invasive tool. We suggest observing for 4-8 weeks in most cases for clinical improvement before switching over to other therapies.
Keywords: Lichen planus; Dorsal pterygium; Topical therapy.
Citation: Revathi K, Rajagopalan R. Unidigital severe lichen planus vulgaris: “Tincture of timing”. J Clin Images Med Case Rep. 2024; 5(1): 2819.
Introduction
Nail involvement in lichen planus is generally seen along with mucocutaneous LP involving other sites. It is seen in up to 10% (3-15%) of patients with LP, 4% of nail LP patients may eventually develop dorsal pterygium, an irreversible destruction of the nail matrix with a ‘V’ shaped extension of the proximal nail fold [1,2]. Here in, we report a case of classical nail lichen planus (LP vulgaris) in right thumb only with no other lesions in skin, oral and genital mucosa.
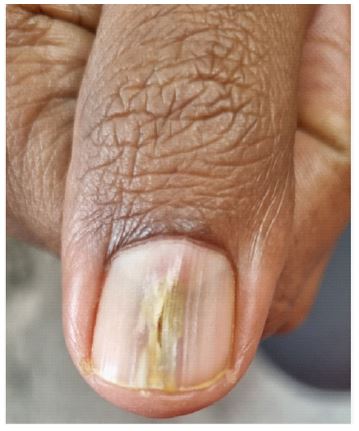
An otherwise healthy 32 year old male, a software professional presented to the skin OPD with complaints of discoloration/slow growth of right thumb nail (cosmetic concerns). There was no previous history of itchy skin eruptions, oral or genital involvement, scalp hair loss or any preceding trauma. Examination of his nails revealed longitudinal groove, pterygium on the right thumb finger (Figure 1). Pup tent sign was positive.KOH/ Lactophenol cotton blue mount for fungus in nail clippings was negative. Onchyoscopy was confirmatory Dermoscopy (DermLite DL4, 10×, polarized mode) which showed thin nail plate, longitudinal ridges, dorsal pterygium with elongated capillaries, and the pup tent sign (nail plate separated from the nail bed with sloping lateral edges). The patient refused nail biopsy. Routine investigations were within the normal limits. Based on the history, physical examination findings and relevant lab findings, a diagnosis of isolated nail lichen planus was made. Patient was initiated on topical steroid lotion (clobetasol propionate 0.05%) 1 drop twice daily and was advised to report after 4 weeks. Patient showed a gradual improvement with the reduction in nail bed erythema and partial closure of nail fissure (Figure 2). At present, he is on topical steroid at night and calcineurin inhibitor (tacrolimus 0.1% solution at morning). Patient is being followed up for development of LP over other nails and skin at regular intervals [3].

Discussion
The degree of nail disease severity is categorized as mild, moderate, or severe. The features of mild nail lichen planus were nail thinning, longitudinal ridging, distal splitting < 3 mm in length, onycholysis area < 25%, and no subungual hyperkeratosis. The features of moderate nail lichen planus were partial fissuring, longitudinal grooves, distal splitting 3 to 5 mm in length, onycholysis area between 25% and 50%, mottled erythema of the lunula, and subungual hyperkeratosis. The features of severe nail lichen planus were complete fissuring, deep grooves, splitting >5 mm in length, onycholysis area >50%, diffuse erythema of the lunula, pterygium, and anonychia. Pterygium unguis is the hallmark of severe nail disease, though not specific. It results from a focal destruction of the nail matrix with subsequent scar formation [4]. As the nail plate is not formed at the affected site, the epithelium of the proximal nail fold attaches itself directly to the nail bed epithelium and both grow distally together to produce a wing-like deformity. Pterygium unguis usually affects the fingers and rarely the toes. Discrete red or violaceous papules in the nail bed may lift and split the overlying nail plate longitudinally, and split lateral edges angle forward to give rise to so called pup tent sign. Pterygium is the most non-responsive form for treatment [5,6]. Topical treatment has poor short-term efficacy and may cause long-term side effects. But to be tried, the first instance to notice any improvement with therapy. Most cases may not respond with an exception as in our case, hence intramatriceal and intramuscular triamcinolone acetonide should also be considered first. Oral retinoids are second-line choices. Immunosuppressive agents like methotrexate, cyclosporine and apremilast may also be considered in the cases who didn’t respond [7]. The percentage of success of a treatment was categorized as follows [8]: no improvement or worsening of nail finding; minimal improvement (≤25% reduction of nail plate abnormality); mild improvement (26% to 50% reduction); moderate improvement (51% to 75% reduction); and great improvement (76% to 99% reduction). Clinical cure was defined as 100% reduction of nail plate and nail bed abnormalities or a normal nail appearance after treatment. When the nails are affected, it may lead to permanent destruction with severe functional impairment and psychosocial consequences. It is most resistant form to treat and is challenging to cure [7].
Conclusion
Although nail lichen planus is a common manifestation of disseminated lichen planus, isolated nail involvement is extremely rare and may pose a diagnostic challenge. Being a true nail emergency, prompt diagnosis and early treatment of this aggressive and deforming disease is essential, even for mild forms.
Declarations
Patient consent: The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship: Nil
Conflicts of interest: There are no conflicts of interest
References
- Goettmann S., Zaraa I., Moulonguet I. Nail lichen planus: epidemiological, clinical, pathological, therapeutic and prognosis study of 67 cases. J Eur Acad Dermatol Venereol. 2012; 26(10): 1304–1309.
- Tosti A., Peluso A.M., Fanti P.A., Piraccini B.M. Nail lichen planus: clinical and pathologic study of twenty-four patients. J Am Acad Dermatol. 1993; 28(5 Pt 1): 724–730.
- Ujiie H, Shibaki A, Akiyama M, Shimizu H. Successful treatment of nail lichen planus with topical tacrolimus. Acta Derm Venereol. 2010; 90(2): 218–9.
- Iorizzo M., Tosti A., Starace M. Isolated nail lichen planus: an expert consensus on treatment of the classical form. J Am Acad Dermatol. 2020; 83(6): 1717–1723.
- Rajababu KK. Nail and its disorders. In: Valia RG, Valia AR, editors. IADVL Textbook of Dermatology. Mumbai: Bhalani Publishing House; 2010. pp. 962–3.
- Naveen KN. Pup tent sign. Indian Dermatol Online J. 2014; 5(4): 552-3.
- Gupta MK, Lipner SR. Review of Nail Lichen Planus: Epidemiology, Pathogenesis, Diagnosis, and Treatment. Dermatol Clin. 2021; 39(2): 221-230.
- McClanahan DR, English JC 3rd. Therapeutics for Adult Nail Psoriasis and Nail Lichen Planus: A Guide for Clinicians. Am J Clin Dermatol. 2018; 19(4): 559-584.