
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Complex hysteroscopic diagnosis from a xanthogranulomatous endometritis to a uterine adenosarcoma after polyp resection: A case report
Natalia Hebrero1*; Mireia Rojas2; Ramon Cos2; Laura Costa2; Raquel Ruiz3; Laia Donoso3; Laia Ribot3; Bibiana Morillas3; Yolanda Canet1
1Department of Obstetrics and Gynaecology, Parc Taulí University Hospital, Institute of Research and Innovation Parc Taulí, I3PT, Autonomous University of Barcelona, Sabadell, Barcelona, Spain.
2Hysteroscopy Unit, Department of Obstetrics and Gynecology, Parc Taulí University Hospital, Institute of Research and Innovation Parc Taulí, I3PT, Autonomous University of Barcelona, Sabadell, Barcelona, Spain.
3Gynaecological Oncology Unit, Department of Obstetrics and Gynecology, Parc Taulí University Hospital, Institute of Research and Innovation Parc Taulí, I3PT, Autonomous University of Barcelona, Spain.
*Corresponding Author : Natalia Hebrero
Department of Obstetrics and Gynecology, Parc Taulí Hospital Universitari, Institut d’Investigació i Innovació Parc Taulí, I3PT, Universitat Autònoma de Barcelona, Sabadell, Barcelona, Spain.
Tel: + 34637747130;
Email: nhebrero@gmail.com
Received : Nov 19, 2023
Accepted : Jan 18, 2024
Published : Jan 25, 2024
Archived : www.jcimcr.org
Copyright : © Hebrero N (2024).
Abstract
Background: Uterine adenosarcoma is rare and can be associated with pelvic radiation and tamoxifen therapy in postmenopausal women. Symptoms are nonspecific but a recurrent polypoid formation is a characteristic clinical feature. Entities such as xanthogranulomatous inflammation is an uncommon type of chronic inflammation, normally associated with a benign condition, but there exist reported cases associated with malignancy.
The objective of this study is to describe a case of a recurrent polypoid formation with a final uterine adenosarcoma diagnosis.
Case report: A 63 year-old female presented with postmenopausal bleeding with no other symptomatology. A first examination with transvaginal ultrasonography showed a mild-vascularized round vacuolated mass occupying the uterine cavity and a blind endometrial biopsy was performed with results of xanthogranulomatous endometritis. A complementary office hysteroscopy showed presence of multiple endometrial polyps and definitive results confirmed xanthogranulomatous endometritis ruling out malignancy. A three month follow-up in office hysteroscopy showed reappearance of multiple polyps, and an operative hysteroscopy resection was performed with a complete resection achieved.
Anatomopathological definitive results confirmed uterine mesenchymal neoplasia (müllerian adenosarcoma with high-grade sarcomatoid overgrowth areas). The patient underwent primary surgery that confirmed diagnosis and a definitive early stage was established. She underwent follow-up evaluation and no further treatment was needed. To date, all follow-up evaluation has shown no evidence of tumor recurrence.
Conclusions: This case report revealed an uncommon uterine adenosarcoma. In cases of recurrent polyp formation in postmenopausal women it is necessary to rule out malignancy.
In the face of an entity such as xanthogranulomatous endometritis, a thorough cavity study is always necessary.
Keywords: Uterine adenosarcoma, müllerian adenosarcoma, xanthogranulomatous endometritis, postmenopausal bleeding, endometrial polyp, hysteroscopy.
Abbreviations: PET-CT: Positron Emission Tomography and Computed Tomography; FIGO: International Federation of Gynaecology and Obstetrics; AJCC: American Joint Committee on Cancer; UICC: Union for International Cancer Control.
Citation: Hebrero N, Rojas M, Cos R, Costa L, Ruiz R, et al. Complex hysteroscopic diagnosis from a xanthogranulomatous endometritis to a uterine adenosarcoma after polyp resection: A case report. J Clin Images Med Case Rep. 2024; 5(1): 2820.
Introduction
Uterine adenosarcoma is a rare neoplasm. According to the World Health Organization’s 2014 classification of uterine malignancies, uterine sarcomas comprise of leiomyosarcoma, endometrial stromal sarcoma, adenosarcoma, undifferentiated endometrial sarcoma and their histologic subtypes, adenosarcomas are the rarest of them all, making up roughly 0.2% of all uterine malignancies and only 8% of all uterine sarcomas [1].
This tumour is associated with pelvic radiation, tamoxifen therapy and hyperestrogenism status.
The age range of onset is very wide, ranging from 10 to 90 years, although it is more frequent in postmenopausal women (approximately from 55 to 65 years old).
Clinically, the symptoms are quite nonspecific, and there may be vaginal bleeding, enlarged uterus or pelvic pain, but a recurrent polypoid formation is one of the most characteristic clinical features, biopsied on several occasions, in which a definitive diagnosis could not be reached. It is common that some patients have often had previous biopsies for a cavity study after abnormal vaginal bleeding, but without an accurate diagnosis. We can also find reports of uterine sarcomas described as a polyp by hysteroscopy [2,3]. Uterine adenosarcoma consists of neoplastic glands with a benign appearance and a sarcomatous stroma.
Macroscopically, these are polypoid or multi-polypoid lesions that can occupy the entire uterine cavity and protrude through the endocervical orifice [4].
Given the relevance in the case, and later described, I will comment on another entity that can be confused in this case: the xanthogranulomatous endometritis.
A xanthogranulomatous inflammation is an uncommon type of chronic inflammation characterised by foamy lipid laden histiocytes admixed with other inflammatory cells.
Xanthogranulomatous endometritis is extremely rare and it typically occurs in postmenopausal women who may have endometrial hyperplasia, endometrial carcinoma and/or cervical stenosis. Normally associated with a benign condition, but in the literature exist some reported cases of this entity associated with malignancy (endometrial adenocarcinoma, mixed carcinoma, escamous cervical carcinoma) [5]. The nonspecific presentation and aggressive imaging characteristics make the differentiation between xanthogranulomatous inflammation and malignancy difficult, so in the face of an entity such as xanthogranulomatous endometritis, a thorough cavity study is necessary.
Case report
A 63 year-old female, with medical history of hypothyroidism in substitutive treatment, appendectomy during childhood and one vaginal delivery, presented in August 2022 to the Gynaecology Emergency Department with sudden-onset postmenopausal bleeding after a casual fall, with no other symptomatology. She referred to this episode as her first bleeding episode after her menopause was established ten years ago.
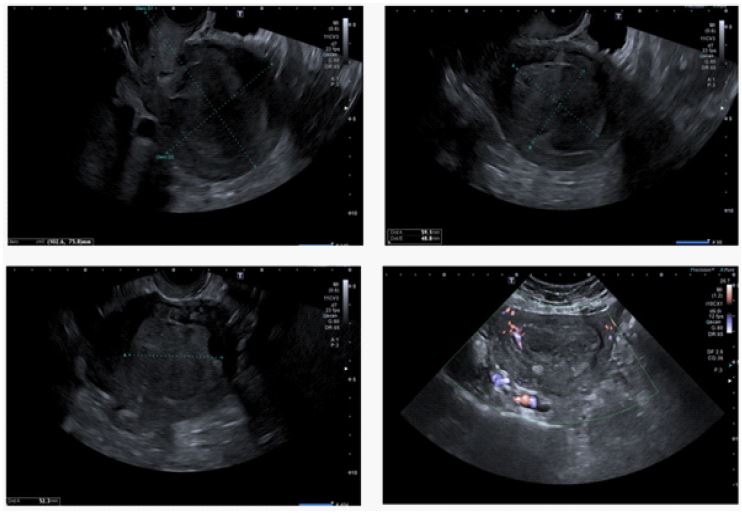
Gynecologic examination detected bloody vaginal discharge. A transvaginal ultrasonography showed a round soft fist-sized heterogeneous vacuolated mass measuring 27x50 mm (Figure 1), occupying the uterine cavity. An endometrial biopsy was performed with results of xanthogranulomatous endometritis (a benign cause) ruling out malignancy.
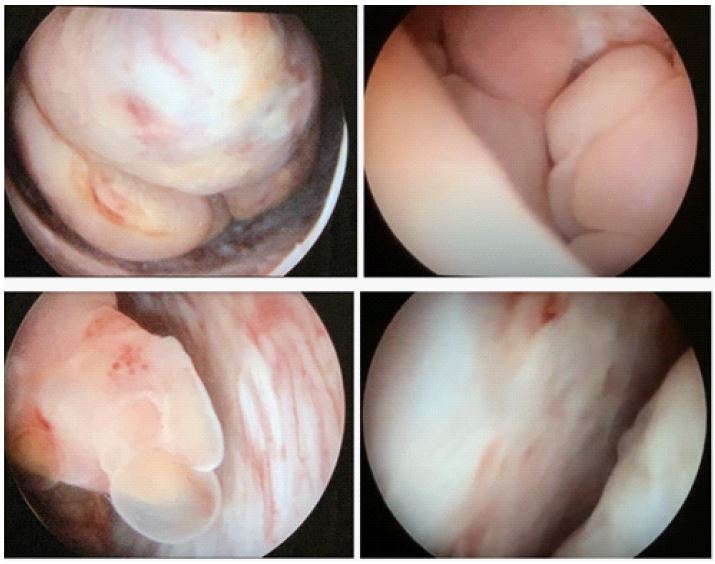
Due to the occupancy of the cavity and the first suspicion of malignant uterine mass versus big polyp formation a first hysteroscopy was performed. It showed presence of multiple endometrial polyps (more than ten), with yellow coloration, inserted in the posterior and fundal wall, the largest measuring four centimetres and hyperplastic appearance, compatible with xanthogranulomatous polyps and not descarting hyperplastic (Figure 2).
Incomplete polypectomy (cancelled by severe pain) and endometrial biopsy are performed with morcellator hysteroscopy equipment in the outpatient clinic, with definitive biopsy results of lymphohistiocytic infiltrate with abundant sparking histiocytes, compatible with xanthogranulomatous endometritis and absence of malignancy signs, and positive to CD68 immunohistochemical study.
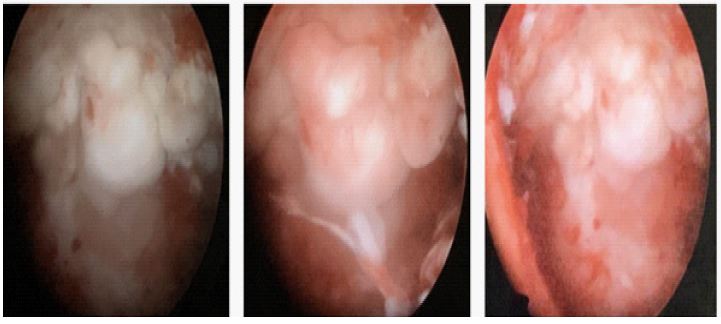
A three month follow up control with a transvaginal ultrasound (Figure 3) and hysteroscopy was performed. She explained persistence of vaginal bleeding, but in less frequency. The hysteroscopy showed the appearance of multiple polyp formation, similar to the first hysteroscopic study and new biopsies were taken with results of benign proliferation (Figure 4).
Due to the perduration of symptomatology and reappearance polypose formation a operative hysteroscopy resection was indicated.
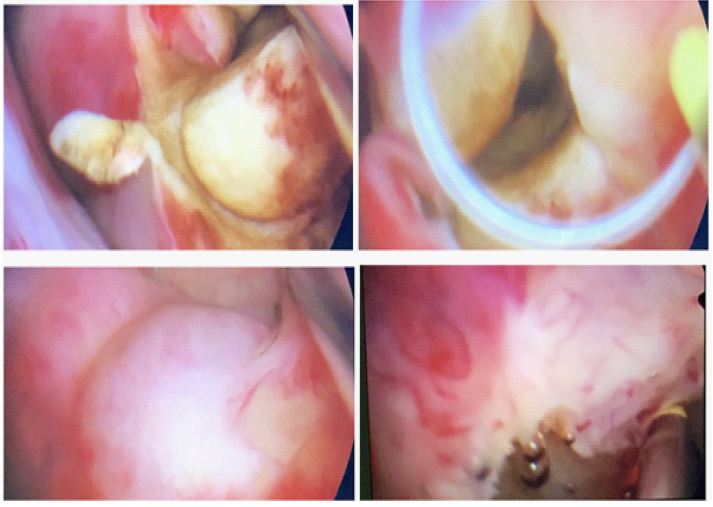
In October 2022 a operative hysteroscopy was performed under general anaesthesia, visualising multiple endometrial polyps (more than five) of 4-5 centimetre size (some fibrous appearance and others more hyperplastic), achieving a difficult complete resection with bipolar resectoscope loop (Figure 5).
The anatomopathological definitive results confirmed uterine mesenchymal neoplasia: morphological and immunohistochemical findings suggest as the first diagnostic option a mullerian uterine adenosarcoma with high-grade areas of sarcomatous overgrowth, with presence of fusocelular appearance cells, abundant necrosis areas and a high Ki67 proliferation index (up to 45%). A wide immunohistochemical panel was performed by the Pathology department, being positive to Vimentina (V9), WT1 (diffuse), estrogens receptors, p16, CD 10, CD34 and INI1 and negative to p53 (wild-type) and rearrangement pattern of the ALK gene.
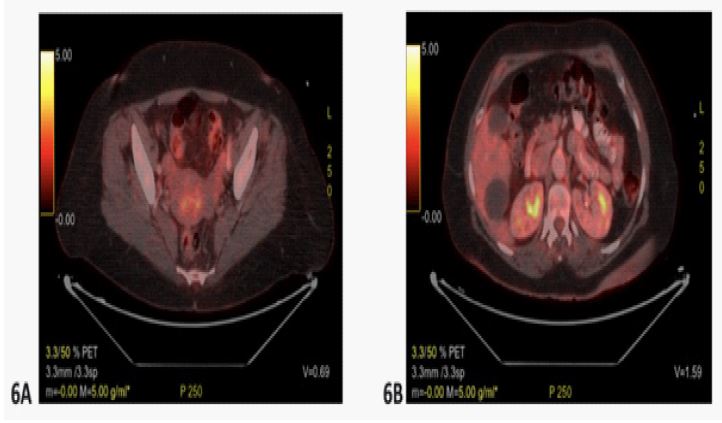
The patient was referred to our Gynecology-Oncology department and an extension study with a complete body positron emission tomography–computed tomography (total body PET-TC) was performed. It showed a discrete hypermetabolic lesion with not-defined margins in the uterus which corresponds to the known neoplasia (Figure 6A), a small right paracaval retroperitoneal hypermetabolic lymphadenopathy suggestive of tumour origin (Figure 6B) and small millimetre adenopathy with no metabolism in the bilateral external iliac region lecture as a nonspecific finding. No other hypermetabolic lesions suspected of metastasis.
With diagnosis of müllerian adenosarcoma with high-grade sarcomatoid overgrowth areas with no metastatic dissemination the patient underwent in January 2023 an abdominal hysterectomy, bilateral adnexectomy and paraaortic lymphadenectomy, with intra-surgery findings of: uterus enlarged in size, normal-looking ovaries, exploration of exposed pelvic ganglion territory during dissection is performed without objectifying any adenopathy, aortocaval lymphadenectomy is performed, visualising enlarge precave and aortocaval adenopathies. Rest of the abdominal cavity reviewed and normal.
Gross examination showed that the uterus measured 12x8x5 cm in size and weighed 226 g and no ovaries or adenopathies were affected.
Microscopic examination revealed a biphasic neoplastic lesion consisting of a benign endometrial epithelial component and a malignant stromal component. The glandular component adopts a “phyllodes-like” growth pattern, with the formation of cleft or dilated glands lined by a simple cubic epithelium of the endometrial type and surrounded by a sarcomatoid stroma, with condensation of the stromal cellularity around the glandular lumens. This mesenchymal component is made up of spindle-shaped cells, with an oval nucleus, granular chromatin and ample and clear cytoplasm.
Sarcomatous overgrowth areas are identified (representing at least 25% of the tumour area), with greater cellular pleomorphism, with larger nuclei with vesiculated and irregular chromatin and obvious nucleolus.
Immunohistochemical analysis showed the mesenchymal component positivity for oestrogen and progesterone receptors, WT-1 and smooth muscle actin while CKAE1-AE3, desmin and CD34 were negative. Preserved expression of CD10 was observed focally in the low-grade component, especially at the periglandular level. With p53, wild-type immunophenotypic expression is observed, compatible with NO mutated protein. The Ki67 proliferative index was approximately 40%. These microscopic findings suggested that the tumour was an adenosarcoma with areas of high grade and sarcomatoid overgrowth.
Taken together, these histologic findings indicated a high-grade Müllerian adenosarcoma, with pathological stage IA according to FIGO guidelines (AJCC-UICC 8th edition, FIGO Cancer Report 2018) [12] and pT1aN0.
The patient underwent follow-up evaluation three weeks after surgery, with good recovery.
Further clinical workup included a two month follow up body PET-CT with no evidence of tumour recurrence.
To date, one year after surgery, regular follow-up evaluation has shown no evidence of tumour recurrence, with negative radiologic findings, including transvaginal ultrasonography, and whole recent body PET-CT.
No further treatment has been necessary to the date.

Discussion
Adenosarcomas are the rarest of uterine sarcomas, making up roughly 0.2% of all uterine malignancies and only 8% of all uterine sarcomas [1].
They mostly originate from the endometrium in 87% of patients, followed by the ovary, cervix, myometrium and pelvis. Almost 60% of patients with this tumor are postmenopausalwomen (from 55 to 65 years old), like in the case described, although the age range of onset is very wide, ranging from 10 to 90 years. It can be associated with pelvic radiation, tamoxifen therapy and hyperestrogenism status.
The symptoms are quite nonspecific, and there may be vaginal bleeding, enlarged uterus or pelvic pain, but a recurrent polypoid formation is one of the most characteristic clinical features. The diagnosis can be challenging with multiple blind endometrial biopsies performed without an accurate diagnosis obtained or suspected benign polyp orientated by hysteroscopy [2,3].
In some occasions other diagnoses can be established by the Pathology department, such as xanthogranulomatous inflammation. Xanthogranulomatous endometritis is extremely rare and it typically occurs in postmenopausal women who may have endometrial hyperplasia, endometrial carcinoma and/or cervical stenosis. Normally associated with a benign condition, but the nonspecific presentation and aggressive imaging characteristics make the differentiation between xanthogranulomatous inflammation and malignancy. In front of an entity such as xanthogranulomatous endometritis, a thorough cavity study is necessary [5].
In uterine adenosarcoma, macroscopically can be seen like polypoid or multi-polypoid lesions that can occupy the entire uterine cavity and protrude through the endocervical orifice [4].
Microscopically, this neoplasm form can be established as a biphasic neoplastic lesion consisting of a benign endometrial epithelial component and a malignant stromal component. The glandular component adopts a “phyllodes-like” growth pattern, with the formation of cleft or dilated glands lined by a simple cubic epithelium of the endometrial type and surrounded by a sarcomatoid stroma, with condensation of the stromal cellularity around the glandular lumens. Sarcomatous overgrowth areas can be identified with greater cellular pleomorphism and with larger nuclei with vesiculated and irregular chromatin.
In the immunohistochemical analysis to confirm a adenosarcoma component was characterized by the mesenchymal component positive for estrogen and progesterone receptors, WT-1 and smooth muscle actin and negative to CKAE1-AE3, desmin and CD34 [3,8].
Mullerian adenosarcoma are usually low grade neoplasms and with good prognosis, but with a high recurrence risk. The prognosis depends basically on the presence of high grade zones with a high ki67 rate and the local advanced diagnosis.
The uterine adenosarcoma treatment is a total simple hysterectomy with double adnexectomy associated with or without radiotherapy treatment [7,8].
Although this neoplasm is associated with a good prognosis, it cannot be forgotten that in some cases might be a progression with metastasis appearance (most common abdominal inf form of peritoneal carcinomatosis) [8].
In our case, the patient presented a low grade mullerian adenosarcoma (with few high grade zones), went through surgery (hysterectomy and double adnexectomy) and orientated as a pathological FIGO IA stage and no further treatment was performed [12]. To the date (one year later), she maintains asymptomatic and no recurrence signs.
Conclusion
Uterine adenosarcoma is a rare neoplasm. A recurrent polypoid formation in a short period of time indicates further studies and rule out malignancy is necessary. The nonspecific presentation and aggressive imaging characteristics make the differentiation between xanthogranulomatous inflammation and malignancy, so in the face of an entity such as xanthogranulomatous endometritis, a thorough cavity study is always necessary.
Declarations
Author’s contributions: NH writing, editing of manuscript and figure preparation. MR editing of manuscript. All authors read and approved the final manuscript.
Funding: No sources of funding to declare.
Availability of data and materials: Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.
Ethics approval and consent to participate: Parc Taulí Commission noted that this report does not require consent to participate.
Consent for publication: Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Conflicts of interest: The authors declare that they have no competing interest.
This work has been presented at a prior international congress in 4th Global Congress on Hysteroscopy, in Sitges - Barcelona 25-28th April 2023.
References
- Nathenson MJ, Ravi V, Fleming N, Wang WL, Conley A. Uterine Adenosarcoma: a Review. Curr Oncol Rep. 2016; 18 (11):68.
- Shveiky D., Revel A., Rojansky N., Benshushan A., Shushan A. Diagnosis of malignant mesenchymal uterine tumors by hysteroscopic excisional biopsy. Min. Inv. Gynecol., 2005; 12: 29.
- Gonzalez-Bosquet E, Suñol M, Torralba A, Lozada C, Miñano J, Lailla JM. Hysteroscopic diagnosis of uterine sarcomas at the Department of Gynaecology, Sant Joan de Déu University Hospital. Eur J Gynaecol Oncol. 2011; 32(4):399-400.
- González Bosquet E, Sunol M, Callejo J, Lailla JM. Uterine adenosarcoma diagnosed following hysteroscopic resection of an intrauterine tumour. Eur J Gynaecol Oncol. 2005; 26(4):415-7.
- Du XZ, Lu M, Safneck J, Baker P, Dean E, Mottola J. Xanthogranulomatous endometritis mimicking endometrial carcinoma: A case report and review of literature. Radiol Case Rep. 2018; 14(1):121-125.
- Wang B, Yang HD, Shi XH, Li H. Advanced uterine adenosarcoma with sarcomatous overgrowth in a young woman: A case report. Medicine (Baltimore). 2019; 98(47): e18119.
- Lee SJ, Park JY. A Rare Case of Intramural Müllerian Adenosarcoma Arising from Adenomyosis of the Uterus. J Pathol Transl Med. 2017; 51(4):433-440
- Muñoz G., Ríos M. J., Valero M. I, Gimeno E. Adenosarcoma mülleriano de útero: un tumor infrecuente de difícil diagnóstico. Progresos de Obstetricia y Ginecología. 2013; 56(7): 382-386.
- Fakhar S, Zahid T, Ishtiaq Y. Uterine adenosarcoma arising from a subserosal adenomyoma: A case report. Gynecol Oncol Rep. 2022; 40:100957.
- Du XZ, Lu M, Safneck J, Baker P, Dean E, Mottola J. Xanthogranulomatous endometritis mimicking endometrial carcinoma: A case report and review of literature. Radiol Case Rep. 2018; 14(1):121-125.
- Merviel P, James P, Carlier M, Thomas-Kergastel I, Guilloique M, Conan-Charlet V et al. Xanthogranulomatous endometritis: A case report and literature review. Clin Case Rep. 2021; 9(6):e04299.
- Amin MB, Edge S, Greene F, Byrd DR, Brookland RK, Washington MK et al. AJCC Cancer Staging Manual, 8th edition.
- Ulker V, Yavuz E, Gedikbasi A, Numanoglu C, Sudolmus S, Gulkilik A. Uterine adenosarcoma with ovarian sex cord-like differentiation: a case report and review of the literature. Taiwan J Obstet Gynecol. 2011; 50(4):518-21.