Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 5
Portomesenteric gas in acute mesenteric ischemia - A defoliate tree appearance
Patrícia Varela Ramos1*; Ângela Simas2
1Intensive Care Unit, Hospital de Vila Franca de Xira, Lisbon, Portugal.
2Intensive Care Unit, Hospital Beatriz Ângelo, Portugal.
*Corresponding Author : Patrícia Varela Ramos
Intensive Care Unit, Hospital de Vila Franca de Xira, Lisbon, Portugal.
Tel: +351963250189.
Email: patriciavarelaramos@gmail.com
Received : Nov 20, 2023
Accepted : Jan 19, 2024
Published : Jan 26, 2024
Archived : www.jcimcr.org
Copyright : © Ramos PV (2024).
Citation: Ramos PV, Simas A. Portomesenteric gas in acute mesenteric ischemia: A defoliate tree appearance. J Clin Images Med Case Rep. 2024; 5(1): 2821.
Description
Acute mesenteric ischemia (AMI) is an uncommon life-threatening emergency in all acute surgical admissions with reported incidence rates of only 0.09-0.2% and a high mortality rate, ranging 30-90% [1,2]. In elderly people, its incidence is rising up to 10% [3-5]. CT angiography of the abdomen and pelvis should be the first-line imaging method in an AMI suspicious condition [2,4,5]. Thus CT angiography can show some common but unspecific imaging findings of acute bowel ischaemia such as bowel wall thickness or luminal dilation and air-fluid levels [4]. In contrast, less common but more specific findings of irreversible bowel ischaemia are pneumatosis and portomesenteric venous gas that are present in 6-28% and 3-14% of cases, respectively [1,4,5]. The most important predictor of patients´ outcome is the time to diagnose AMI [3].
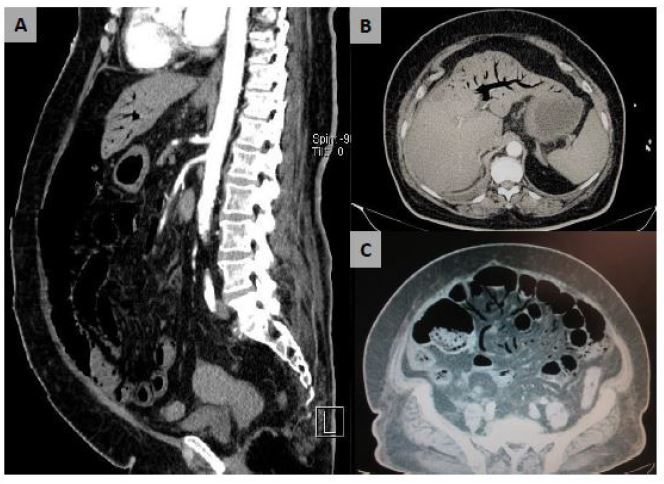
A 76-year-old woman with a known history of gastric lymphoma, arterial hypertension, dyslipidaemia, diabetes, and new onset atrial fibrillation was admitted to the Emergency Room due to a distended and painful abdomen. Arterial blood gas analysis showed a metabolic and lactic acidosis. Laboratory tests showed an acute kidney injury, LDH 199 UI/L. Given the suspicion of bowel ischaemia, she underwent an urgent CT-scan that showed clear signs of diffuse bowel necrosis with evident pneumatosis intestinalis, extensive portomesenteric gas and a filiform superior mesenteric artery.
A high index of clinical and radiologic suspicion is required for accurate and timely diagnosis [2,5]. Early recognition and prompt diagnosis and intervention are crucial and eventually lifesaving, reducing mortality. All clinicians should keep in mind patient symptoms and dependent risk factors [3]. AMI diagnosis can be a challenge as patients´ symptoms, laboratory test results and imaging findings are often nonspecific [2].