
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Ulcerative colitis in a young Nigerian male: A case report
Lukman O Abdulkareem1,4*; Oluwasesan A Abdul2; Rukayat A Abdulkareem3; Kosisochukwu G Analikwu4
1Department of Internal Medicine, University of Abuja Teaching Hospital, Abuja, Nigeria.
2Department of Histopathology, University of Abuja Teaching Hospital, Abuja, Nigeria.
3Department of Family Medicine, University of Abuja Teaching Hospital, Abuja, Nigeria.
4Arewa Specialist Hospital and Diagnostic Centre, Abuja, Nigeria.
*Corresponding Author : Abdulkareem LO
Department of Internal Medicine, University of Abuja Teaching Hospital, Abuja, Nigeria.
Email: lukkareem@yahoo.com
Received : Dec 18, 2023
Accepted : Jan 19, 2024
Published : Jan 26, 2024
Archived : www.jcimcr.org
Copyright : © Abdulkareem LO (2024).
Abstract
Ulcerative Colitis (UC) is a chronic inflammatory bowel disease which is rare in the Nigerian populace. It is often misdiagnosed as most patients may not have ready access to endoscopy services which is key to diagnosis. We present a 22 year old Nigerian male who was referred to our clinic on account of passage of frequent blood-stained and mucoid stools of about two months duration. He had associated abdominal discomfort, weight loss, easy fatiguability and low-grade fever. He had been previously evaluated and managed by his general practitioner without resolution of symptoms. Physical examination was remarkable for pallor and mild abdominal tenderness. Rectal examination was unremarkable except for blood-stained stools on the examining finger. An assessment of suspected inflammatory bowel disease to rule out colonic malignancy was made. Colonoscopy showed widespread erosions/ulcerations, granularity and loss of normal mucosa lustre involving the rectum and the entire colon. Multiple biopsy specimen taken for histology confirmed features consistent with UC. He was commenced on mesalazine, prednisolone, antibiotics and haematinics. When he was reviewed after six weeks, he had made remarkable improvement with resolution of symptoms and improvement in laboratory parameters. The significance of this case lies in the rarity of UC among Nigerians. However, to make a diagnosis, a high index of suspicion and prompt colonoscopy assessment among individuals with chronic blood-stained diarrhea are essential.
Keywords: Ulcerative colitis; Colonoscopy; Nigeria.
Abbreviations: UC: Ulcerative Colitis; IBD: Inflammatory Bowel Disease; CD: Crohn’s Disease; GI: Gastrointestinal.
Citation: Abdulkareem LO, Abdul OA, Abdulkareem RA, Analikwu KG. Ulcerative colitis in a young Nigerian male: A case report. J Clin Images Med Case Rep. 2024; 5(1): 2823.
Introduction
Inflammatory Bowel Disease (IBD) is a chronic inflammatory disorder of the gastrointestinal tract caused by a dysregulated immune response to host intestinal lining [1]. There are two major types of IBD namely; Ulcerative Colitis (UC) and Crohn’s Disease (CD). Colonoscopy is needed for diagnosis with histological confirmation from tissue biopsy obtained at colonoscopy. UC is a rare disease among Blacks with an estimated prevalence rate of about 9.9-11.2 per 100,000 population [2]. It is however, about 40-fold more prevalent among Caucasians [2]. There are a few case reports and case series on UC in Nigeria but there is no national study on the prevalence of UC in Nigeria [3-5]. Reported colonoscopy studies in Nigeria have also shown the rarity of the disease among patients studied [6,7]. Moreover, some suspected UC at colonoscopy may not be confirmed histologically [8]. This publication aims to add to the literature on UC in Nigeria. We thus present a 22 year old Nigerian male who had a histologic diagnosis of UC following characteristic symptoms and colonoscopy features of the disease.
Case presentation
Mr. R. W, a 22 year old male undergraduate, presented with complaints of frequent passage of stools of two months durations and recurrent abdominal pain of one month duration. Stools were about five episodes per day, could be formed, but loose most times, usually small volume, mucoid and blood stained with associated tenesmus. He had occasional vomiting usually containing recent meals or fluids, but not bilious or blood stained. Recurrent abdominal pain was located in the lower abdomen, insidious in onset and described to be sharp but did not radiate to any other region. There was no aggravating factor but pain was sometimes relieved after stooling. He had associated anorexia, occasional low-grade fever and progressive weight loss (about 7 kg in over the previous two months). He had no cardio-respiratory, neurological or urinary symptoms. He had no visual, skin or musculoskeletal symptoms. He had no similar symptoms in the past. He lived with his parents and his meals were cooked at home while source of drinking water was pipe-borne and sachet water. He had no significant past medical history. He was not on any medication, such as laxatives or antibiotics, prior to onset of illness. There was no family history of similar illness, IBD or colorectal malignancy. He neither smoked cigarette nor drank alcohol. He had been treated by general practitioners in other health centres without resolution of his symptoms. This necessitated his being referred to our facility. At presentation, he was acutely ill-looking, asthenic, weight was 54.5 kg, afebrile (axillary temperature was 37.0oC), pale, anicteric, acyanosed, mildly dehydrated and had no pedal oedema. His pulse was 92 beats per minute, regular and full volume. Blood pressure was 128/84 mmHg and heart sounds were first and second only. Abdominal examination revealed mild tenderness at the suprapubic and left iliac fossa regions, no palpable organomegaly and no demonstrable ascites. Bowel sounds were present and normoactive. Rectal examination was normal but gloved finger was blood-stained. Respiratory and neurologic system examinations were normal. A preliminary diagnosis of suspected IBD to rule out colorectal malignancy was made. Samples were taken for investigations-results are as shown on Table 1. Abdominal ultrasound scan was normal. He had both upper Gastrointestinal (GI) endoscopy and colonoscopy done. Upper GI endoscopy showed grossly normal findings. Colonoscopy showed widespread erythema with erosions and ulcerations involving the rectum and the entire colonic mucosa (Figure 1). The colonic mucosa lacked the normal lustre and also appeared granular in some parts. There were however, no polyps or pseudopolyps. The terminal ileum was normal. Multiple biopsy specimen were taken from the different parts of the colon, stored in formalin, labelled and sent for histology. An assessment of “Moderately severe Ulcerative Pan-colitis” was made. He was commenced on mesalazine granules and suppositories. He was also placed on Prednisolone 40 mg which was reduced by 10 mg every week over a four-week period. He had a five-day course of antibiotics. Haematinics and probiotics were also added to his treatment. Histology report showed: Macroscopy: Received specimens labelled A-caecal mucosa, B-ascending colon mucosa, C-transverse colon mucosa, D-descending colon mucosa, E-sigmoid colon mucosa, F-rectal mucosa-all containing four (4) fragments each. Microscopy: Histological sections from specimen labelled “A”-“F” showed similar lesions. It was composed of focal ulcerations and erosions, crypt distortion with basal lymphoplasmacytosis, intense polymorphonuclear cellular infiltrates limited to the superficial mucosa and cryptitis. There was no formation of granulomas or dysplasia. Diagnosis: A-F: Ulcerative Colitis. Figure 2 shows the histology microphotographs. He had follow-up clinic visits after two and six weeks. On his follow up visit at 6 weeks, his clinical condition had improved remarkably. His bowel movement had reduced to two times a day and was no longer mucoid or blood-stained. His weight had improved to 62 kg. Laboratory parameters improved as compared to his pre-treatment laboratory results (Table 1). He was to continue mesalazine and scheduled for 3 monthly follow-up appointments.
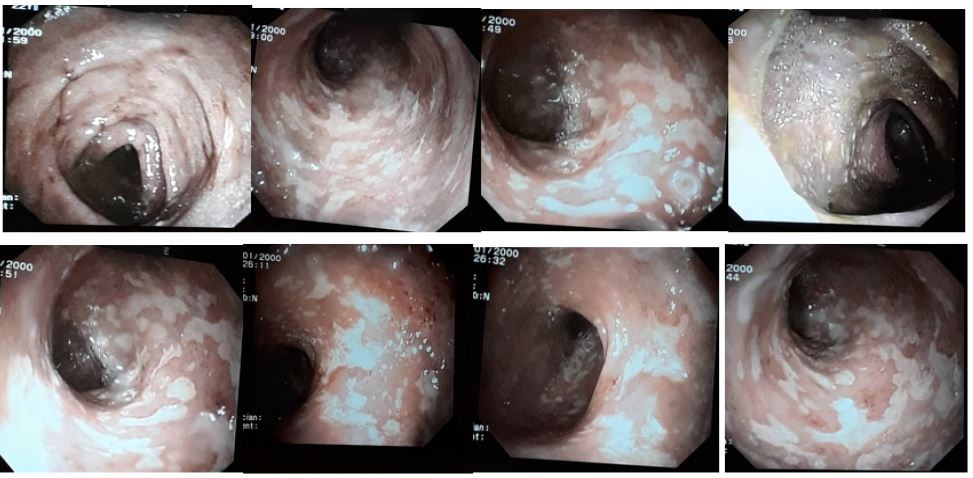
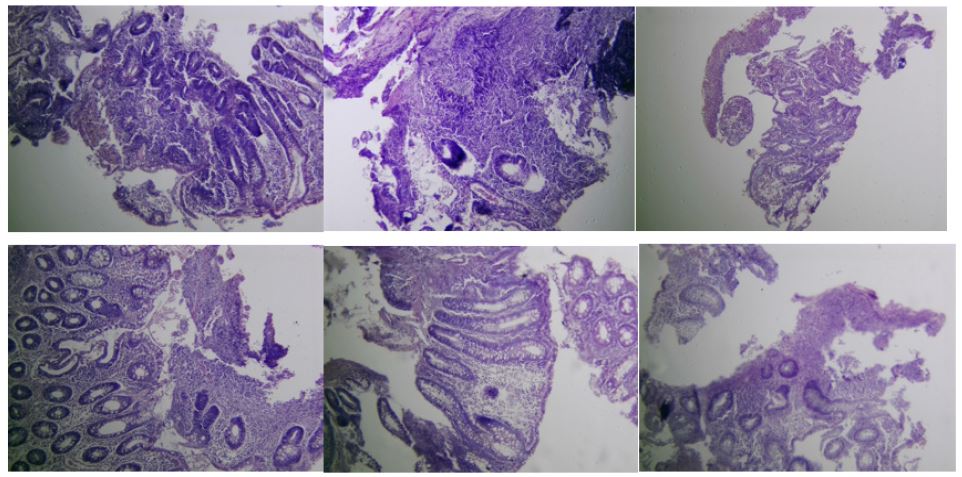
Table 1: Laboratory parameters of R.W.
| Laboratory Parameter | At Presentation | Follow up at 2 weeks | Follow up at 6 weeks |
|---|---|---|---|
| Erythrocyte sedimentation rate (mm/hr) | 61 | 12 | 5 |
| Random Blood Sugar (mmol/L) | 5.3 | 5.1 | |
| Full Blood Count (FBC)> | |||
| Hb (g/dl) | 7.9 | 9.6 | 13 |
| PCV (%) | 25.4 | 31.5 | 42.8 |
| MCV (fl) | 62.7 | 71.6 | 76.2 |
| MCH (pg) | 19.5 | 21.8 | 23.3 |
| MCHC | 31.1 | 30.5 | 30.6 |
| WBC (x109/L) | 9.89 | 13.61 | 6.21 |
| Neutrophils (%) | 65.1 | 87.4 | 66.0 |
| Lymphocytes (%) | 19.0 | 8.7 | 22.7 |
| Monocytes (%) | 14.9 | 3.2 | 10.3 |
| Basophils (%) | 0.5 | 0.3 | 0.2 |
| Eosinophils (%) | 0.5 | 0.4 | 0.8 |
| Platelets (x109/L) | 133 | 371 | 260 |
| Electrolyte, Urea,Creatinine | |||
| Sodium (mmol/L) | 140 | 142 | |
| Potassium (mmol/L) | 3.3 | 3.0 | |
| Bicarbonate (mmol/L) | 22 | 20 | |
| Chloride (mmol/L) | 100 | 103 | |
| Urea (mmol/L) | 5.5 | 3.5 | |
| Creatinine (µmol/L) | 70.0 | 60.4 | |
| Liver function test | |||
| AST (U/L) | 15 | 20 | 18 |
| ALT (U/L) | 6 | 53 | 16 |
| ALP (U/L) | 41 | 30 | 45 |
| Total Bilirubin (µmol/L) | 4.3 | 3.0 | 5.7 |
| Direct Bilirubin (µmol/L) | 2.3 | 1.8 | 1.8 |
| Total Protein (g/L) | 70 | 68 | 72 |
| Albumin (g/L) | 34 | 43 | 45 |
| Globulin (g/L) | 36 | 25 | 27 |
| GGT (U/L) | 17 | 40 | 24 |
Discussion
UC is a chronic relapsing inflammatory disease of the large bowel that typically affects the rectum and extends in a retropattern to involve a variable part of the large intestine [1]. It is commoner among Caucasians, especially among people of Ashkenazi Jewish descent, compared to Asians or Blacks. Reported prevalence rates of UC are 249/100,000 in North America and 505/100,000 in Europe [2]. Much lower prevalence rates of 9.9-11/100,000 has been reported in sub-Saharan Africa [2]. U.C is a rare disease in Nigeria, though there is paucity of data on the national prevalence rate amongst Nigerians. There are only a few case reports and case series of UC amongst Nigerians found in the literature [3-5]. Colonoscopy reports in Nigeria shows a prevalence rate of 1.3% among those who underwent colonoscopy in Ibadan, southwest Nigeria [6]. UC is slightly commoner in females than males. The age of onset has a bimodal pattern, with a peak at 15-25 years age group which our patient belonged to [9]. There is a second, though smaller peak at 55-65 years however, the disease can occur at any age [9]. The disease is typically characterized by diffuse colonic mucosa inflammation and ulcerations. Predominant symptoms of UC are frequent loose, blood-stained and mucoid stools. These are usually associated with tenesmus, abdominal pains, low-grade fever and weight loss. These symptoms were present in our patient. It usually runs a chronic relapsing course and diagnosis is most times elusive until a colonoscopy is done. Previous case reports and case series of UC in Nigeria reported a range of about 2-7 years from onset of symptoms to colonoscopic/ histologic diagnosis [3,4]. Perhaps, delay in diagnosis is usually due to low index of suspicion, poor referral system to specialist care as well as paucity of colonoscopy services in the country [10]. Delay in diagnosis of UC is usually associated with a greater risk of complications and other morbidities from the disease [11]. A study showed that delayed diagnosis of UC was the only factor associated increased intestinal surgery risks (OR=6.81) [11]. Our patient had prompt referral to specialist care with diagnosis of UC made two months after onset of symptoms which is much earlier than previously reported cases from our environment. The mainstay of treatment of UC is medical therapy and includes the use of corticosteroids, amino-salicylates and other anti-inflammatory agents/ biologics. Rehydration, anti-diarrhea agents, antibiotics (short-term use) and probiotics also have roles to play in treating UC. Our patient had a combination of some of these medical therapy with marked improvement of symptoms. Surgery is reserved for those presenting with complications, surgical emergency (such as toxic megacolon) or when medical therapy fails.
Conclusion
Despite the rarity of UC in our environment, a high index of suspicion among physicians is important particularly in patients with typical symptoms of UC, after ruling out infective causes and other common causes of haematochezia. The importance is to avoid delays in diagnosis and treatment in order to prevent complications from the disease. More extensive studies are needed in Nigeria to determine the prevalence of UC in the general population. Perhaps a national data base may be created for this purpose. Colonoscopy services should be made more readily available and affordable in Nigeria to aid prompt diagnosis of UC among other important colonic diseases.
Declarations
Conflict of interest statement: The authors have no conflicts of interest to declare.
Ethical consideration: The patient gave oral consent to publish his case.
Funding sources: None.
References
- Kaistha A, Levine J. Inflammatory bowel disease: The classic gastrointestinal autoimmune disease. Curr Probl Pediatr Adolesc Health Care. 2014; 44: 328-34.
- Watermeyer G, Katsidzira L, Setshedi M, Devani S, Mudombi W, et al. Gastroenterology and Hepatology Association of sub-Saharan Africa (GHASSA). Inflammatory bowel disease in sub-Saharan Africa: Epidemiology, risk factors, and challenges in diagnosis. Lancet Gastroenterol Hepatol. 2022; 7: 952-961.
- Ekwunife CN, Nweke IG, Achusi IB, Ekwunife CU. Ulcerative Colitis Prone to Delayed Diagnosis in a Nigerian Population: Case Series. Ann Med Health Sci Res. 2015; 5: 311-313.
- Alatise OI, Otegbayo JA, Nwosu MN, Lawal OO, Ola SO, et al. Characteristics of inflammatory bowel disease in three tertiary health centers in southern Nigeria. West Afr J Med. 2012; 31: 28-33.
- Senbanjo IO, Oshikoya KA, Onyekwere CA, Abdulkareem FB, Njokanma OF. Ulcerative colitis in a Nigerian girl: A case report. BMC Res Notes. 2012; 5: 564.
- Akere A, Oke TO, Otegbayo JA. Colonoscopy at a tertiary healthcare facility in Southwest Nigeria: Spectrum of indications and colonic abnormalities. Ann Afr Med. 2016; 15: 109-113.
- Bojuwoye MO, Bamidele OF, Okonkwo K, Adeyeye A, Aliyu AM, et al. The Indications and Findings at Colonoscopy in a Tertiary Hospital in North-Central Nigeria: A Seven-Year Review. West African Journal of Medicine. 2021; 38: 885-891.
- Musa Y, Abdulkadir YM, Manko M, Umar YS, Mohammed AN, et al. A 10-year review of colonoscopy at Aminu Kano Teaching Hospital, Kano Nigeria. Niger J Clin Pract. 2021; 24: 1072-1076.
- Jang ES, Lee DH, Kim J, Yang HJ, Lee SH, et al. Age as a clinical predictor of relapse after induction therapy in ulcerative colitis. Hepatogastroenterology. 2009; 56: 1304-1309.
- Watermeyer G, Katsidzira L, Nsokolo B, Alatise O, Duduyemi BM, et al. Challenges in the diagnosis and management of IBD: A sub-Saharan African perspective. Therap Adv Gastroenterol. 2023; 16: 17562848231184986.
- Lee DW, Koo JS, Choe JW, Suh SJ, Kim SY, et al. Diagnostic delay in inflammatory bowel disease increases the risk of intestinal surgery. World J Gastroenterol. 2017; 23: 6474-6481.