
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Sinusoidal obstruction syndrome of the liver successfully managed by defibrotide during chemotherapy in a child with Hodgkin lymphoma with liver involvement: A case report and review of the literature
Dima Abla1*; Emad Saad1; Nasser Al-Rahbi2
1Department of Pediatric Hematology and oncology, The National Oncology Centre, Royal Hospital, Muscat, Oman.
2Department of Pathology, Royal Hospital, Ministry of Health, Muscat, Oman.
*Corresponding Author : Dima Abla
Department of Pediatric Hematology and oncology, The National Oncology Centre, Royal Hospital, Muscat, Oman.
Tel: +968-79977195;
Email: abladeema@gmail.com
Received : Jan 01, 2024
Accepted : Jan 22, 2024
Published : Jan 29, 2024
Archived : www.jcimcr.org
Copyright : © Abla D (2024).
Abstract
Background: Sinusoidal Obstruction Syndrome (SOS) of the liver is a life-threatening disorder generally occurring as a complication of Hematopoietic Stem Cell Transplantation (HSCT). Here, we describe a case of a child with Hodgkin’s lymphoma and liver involvement who developed SOS during induction chemotherapy outside the transplant context, which is a very unusual presentation in pediatric patients.
Case description: This case describes a 12-year-old male patient with Hodgkin’s Lymphoma and liver involvement. During induction chemotherapy, which contained Vincristine and Cyclophosphamide, he developed SOS symptoms, including weight gain, refractory thrombocytopenia, and hyperbilirubinemia. He was managed successfully with Defibrotide.
Conclusion: This case is one of the rare reported cases for SOS during induction chemotherapy in a child with Hodgkin’s Lymphoma and liver involvement, highlighting the importance of early recognition and treatment of this fatal complication.
Key findings: The successful management of a patient with Hodgkin’s Lymphoma and liver involvement who developed SOS during induction chemotherapy.
What is known and what is new?
-SOS is a known complication in HSCT patients. Sometimes, it can be missed in non-HSCT patients.
-Liver involvement could be a risk factor for developing SOS in patients with Hodgkin’s Lymphoma.
What is the implication, and what should change now?
-SOS should be recognized early during chemotherapy in non-HSCT pediatric patients, and aggressive treatment should be provided.
-A multidisciplinary approach provided by pediatric oncologists, intensivists and radiologists is essential.
Keywords: Sinusoidal obstruction syndrome; Hodgkin’s lymphoma; Chemotherapy; Defibrotide; Case report.
Citation: Abla D, Saad E, Rahbi NA. Sinusoidal obstruction syndrome of the liver successfully managed by defibrotide during chemotherapy in a child with Hodgkin lymphoma with liver involvement: A case report and review of the literature. J Clin Images Med Case Rep. 2024; 5(1): 2825.
Background
Sinusoidal Obstruction Syndrome (SOS) of the liver, is a well-known fatal complication that can occur after Hematopoietic Stem Cell Transplantation (HSCT) [1]. It also has been described in non-transplant settings after chemotherapy or radiotherapy for different types of malignances [2]. Defibrotide remains the corner stone of management of SOS in both HSCT and non-HSCT patients [2]. Here, we present a case of a 12-year-old pediatric patient who developed SOS during induction chemotherapy for stage IV Hodgkin’s Lymphoma with liver metastasis and successfully managed by Defibrotide. A comprehensive literature review was performed regarding diagnosis, treatment and prophylaxis of SOS in children.
Case description
A 12-year-old previously healthy male was referred to our department in January 2022 from a peripheral hospital with a 1-week history of fever, fatigue, anemia and loss of weight. Family history was unremarkable. Physical examination revealed right cervical and supraclavicular lymph adenopathy as well as hepatosplenomegaly. Blood work performed on admission showed moderate anemia (hemoglobin of 7 g/dL), mild thrombocytopenia (Platelets count of 139x109/L), a mild transaminitis with elevated Bilirubin (total bilirubin of 41 umol/L and conjugated bilirubin of 28 umol/L). Erythrocyte Sedimentation Rate (ESR) was markedly elevated at 99 mm/hr, lactate dehydrogenase was slightly elevated as well at 511 U/L and Albumin level was 17 g/L.
Initial diagnostic imaging was done including Computed Tomography (CT) of the chest and abdomen which showed a mediastinal mass, enlarged hilar lymph nodes, hepatomegaly with multiple hypo-enhancing focal lesions, and splenomegaly with innumerable focal lesions. Bilateral bone marrow aspirates and biopsies were negative for atypical infiltrates. An ultrasound-guided liver biopsy demonstrated infiltration by large bi-nucleate and mononuclear cells with prominent eosinophilic nucleoli. On immunohistochemistry, the neoplastic cells were CD30, CD15 positive, Pax5 weakly positive, EBV, CD20, and CD3 negative, confirming the diagnosis of Classic Hodgkin lymphoma (Figure 1). A Positron Emission Tomography (PET) scan was performed for disease staging and showed multiple FDG avid enlarged right cervical, supraclavicular, mediastinal, hilar, peripancreatic, porta hepatis, and para-aortic lymph nodes, hepatosplenomegaly with multiple infiltrative splenic and intraparenchymal lesions, and focal increased FDG activity at the right acetabulum (Figure 2).
Based on the initial workup, the patient was risk stratified as stage IV B, high risk. CHIPS score: 3. Chemotherapy was initiated as per Hodgkin lymphoma, high-risk protocol (based on COG AHOD0831, and AHOD1331 HR Protocols) with cycle I ABVE-PC (doxorubicin, bleomycin, vincristine, etoposide, prednisone, and cyclophosphamide). On day 4 of Cycle I, the patient complained of abdominal pain and vomiting. On physical examination, he was icteric with signs of respiratory distress and abdominal tenderness. On the next day, his clinical status progressively deteriorated with a rapid increase in bilirubin levels (total bilirubin of 116 umol/L and conjugated bilirubin of 83 umol/L),an increase in body weight by 5 kg, which makes 9% of his original weight, and refractory thrombocytopenia (Platelets count of 19x109/L which did not respond to platelets transfusion). A chest x-ray was showing bilateral pleural effusion with features of pulmonary edema, and an ultrasound abdomen revealed hepatosplenomegaly with a moderate amount of ascites.
According to the above clinical and biochemical findings, the patient was fulfilling all the 5 European Society for Blood and marrow Transplantation (EBMT) diagnostic criteria for hepatic Sinusoidal Obstruction Syndrome (SOS) in children, he was transferred to the pediatric intensive care unit for supportive care, including diuretics, strict fluid balance, and respiratory support. Vincristine and Bleomycin of day 8 were omitted. He started to improve clinically, but due to persistent fluid overload, hepatic dysfunction, and refractory thrombocytopenia, N-Acetyl cysteine was started on day 14 as Defibrotide was not available. After 2 days Defibrotide was administered at a dose of 6.25 mg/Kg/dose every 6 hours as a 2-hour intravenous infusion for a total of 17 days. On day 23, the patient underwent pericardiocentesis when 300 mL of serosanguinous fluid was removed. Eventually on day 31, all the symptoms resolved with normalization of liver function tests and platelets count, and the patient’s weight returned to his baseline, (Figure 3). Therefore, the decision was to proceed to cycle II with Defibrotide prophylaxis, he received it for 3 days and then stopped.
The patient was subsequently able to complete his remaining 3 cycles of chemotherapy. Clinical course was complicated by polyneuropathy, which required elimination of Vincristine in cycles III, IV, and V. He received Involved-Field Radiation Therapy (IFRT) at a dose of 21Gy to the spleen and mediastinum. No other adverse events were encountered. The patient remained in clinical and radiologic remission for 1 year following the completion of therapy. Ultimately, both the patient and his parents were satisfied with the outcome.
Timeline: In summary, diagnosis of Hodgkin lymphoma was confirmed and patient was started on chemotherapy in February 2022. SOS symptoms started on day 4 of cycle I. Defibrotide was started on day 16 for a total of 17 days. Pericardiocentesis was done on day 23. Symptoms resolved on day 31.
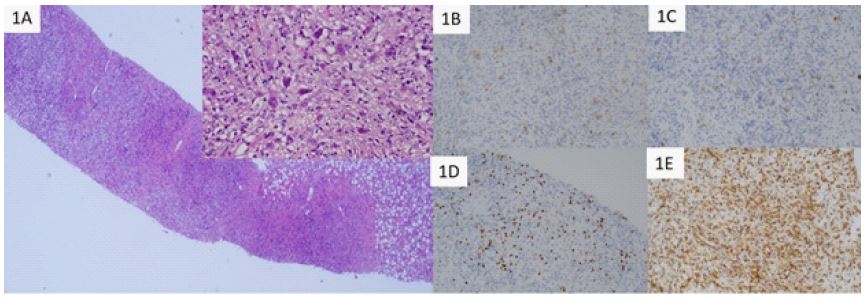
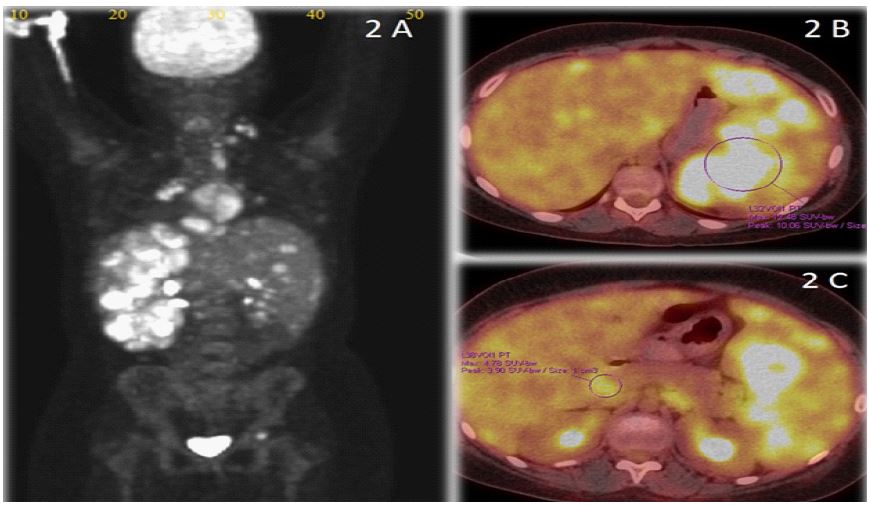
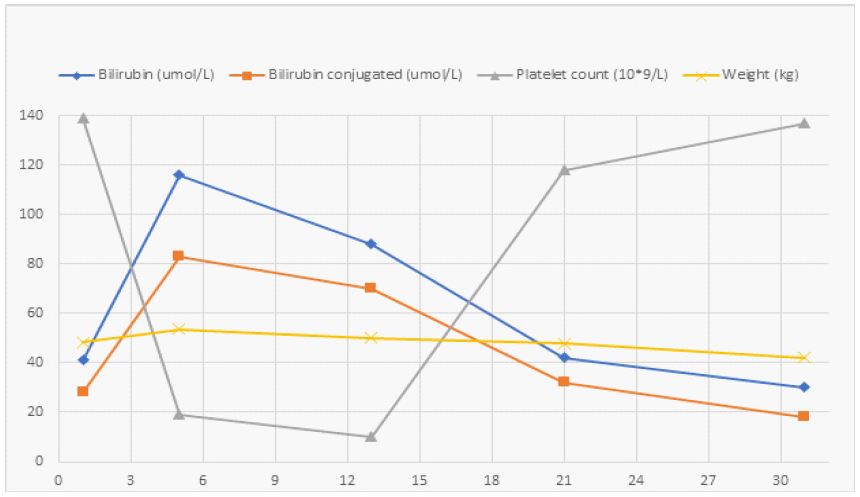
Table 1: EBMT diagnostic criteria for hepatic SOS/VOD in children [4].
| • No limitation for time of onset of SOS/VOD |
| The presence of two or more of the following: |
| • Unexplained consumptive and transfusion-refractory thrombocytopenia |
| • Otherwise unexplained weight gain on three consecutive days despite the use of diuretics or a weight gain >5% above baseline value |
| • Hepatomegaly (best if confirmed by imaging) above baseline value |
| • Ascites (best if confirmed by imaging) above baseline value |
| • Rising bilirubin from a baseline value on 3 consecutive days or bilirubin ⩾2 mg/dL within 72 h |
Discussion
SOS, previously known as a Veno-Occlusive Disease (VOD), is a serious complication caused by damage in the sinusoidal endothelial cells of the liver leading to obstruction of the sinusoidal flow [1]. It was established as a disease entity during the 1950s [3]. Although it is mainly observed after HSCT, it can also occur as a complication of conventional chemotherapy, immunotherapy, or radiation therapy outside of the setting of HSCT [2]. In the recent European Society for Blood and Marrow Transplantation (EBMT) criteria for SOS/VOD in pediatric patients, there is neither limitation for the time of onset of VOD, nor restriction to only HSCT patients [4] (Table 1).
Risk factors for hepatic SOS after HSCT are divided into pretransplant patient characteristics like age, underlying disease, and pre-existent liver disease, as well as transplantation-related factors such as conditioning regimen and graft source [5]. In non-transplant patients, SOS has been described to be associated with many chemotherapeutic agents including actinomycin-D, vincristine, cyclophosphamide, and thioguanine [2]. Early in 1985, Björk O et al. [3] observed VOD in 8 patients with Wilms Tumor treated with Actinomycin D. Elli, Murat et al. [6] and Ishaqi, M Kashif et al. [7] reported 2 cases of liver SOS after one course of chemotherapy for Medulloblastoma. McAtee, Casey L et al. [8] described 10 patients who developed SOS within 60 days of receiving a short-course of the anti-metabolite 6-thioguanine (6-TG) for the treatment of Acute Lymphoblastic Leukemia (ALL). In a multicenter, single-arm, US clinical trial (NCT00628498), 66 patients were aged ≤16 years and had nontransplant-associated SOS [2]. Recently in 2021, AlSaad, Tayseer et al. [9] reported a case series of 6 patients in Qatar who developed SOS after standard treatment for different types of malignancies outside the HSCT context. Our patient developed SOS shortly after starting cycle I chemotherapy for Hodgkin Lymphoma which contained vincristine and cyclophosphamide.
Many studies had linked the pre-existent liver disease to the increased risk for hepatic SOS [10-12]. The involvement of the liver by Hodgkin lymphoma in our patient could be a predisposing factor for developing SOS.
As hepatic SOS is a fatal disease, treatment should be initiated as soon as the first evidence of SOS occurs, rather than waiting for development of severe disease [2]. Currently, the treatment of choice is Defibrotide, which is approved by both the United States Food and Drug Administration (FDA) as well as the European Medicines Agency (EMA) for the treatment of SOS [2]. It has been observed that patients who had nontransplant-associated SOS demonstrated superior survival if the treatment was started before development of Multi-Organ Dysfunction (MOD) [2]. N-acetylcysteine (NAC) was used for the treatment of SOS in children and showed good results [13]. In our case, treatment with N-acetylcysteine was started awaiting the availability of Defibrotide.
Neither FDA nor EMA has approved any medication for the prevention of hepatic SOS. 2 ongoing studies are conducted to prove the role of SOS prophylaxis in high-risk patients undergoing HSCT. The first study is a Phase 3, randomized trial (NCT02851407) comparing the Efficacy and safety of Defibrotide vs best supportive care in the prevention of hepatic VOD. The other one is a phase 2, randomized, placebo-controlled study (NCT04712435) to evaluate the efficacy and safety of N-acetylcysteine as prophylaxis of SOS. The role of SOS prophylaxis in non-transplant patients has not been studied yet. We opted to give our patient Defibrotide as prophylaxis during the second cycle of chemotherapy, but unfortunately, it was stopped due to lack of supply of the drug.
Conclusion
This case report emphasizes the importance of early recognition and aggressive management of SOS in non HSCT pediatric patients during chemotherapy. It also highlights the role of multidisciplinary care to those patients provided by pediatric oncologist, intensivists and radiologists. Further studies are certainly needed to identify patients at risk who are candidate for prophylaxis to prevent this serious fatal complication.
Declarations
Patient’s/Guardian’s consent: Informed consent was obtained from the patient guardian.
Ethical clearance: Not required
Funding: This research did not receive any specific grant from funding agencies in the public, commercial or not-for-profit sectors.
Declaration of competing interest: None.
Acknowledgments: None.
References
- Mohty M, Malard F, Abecassis M. et al. Sinusoidal obstruction syndrome/veno-occlusive disease: current situation and perspectives—a position statement from the European Society for Blood and Marrow Transplantation (EBMT). Bone Marrow Transplant. 2015; 50: 781-789. https://doi.org/10.1038/bmt.2015.52.
- Kernan NA, Richardson PG, Smith AR, et al. Defibrotide for the treatment of hepatic veno-occlusive disease/sinusoidal obstruction syndrome following nontransplant-associated chemotherapy: Final results from a post hoc analysis of data from an expanded-access program. Pediatr Blood Cancer. 2018; 65: 27269. https://doi.org/10.1002/pbc.27269.
- Björk O, Eklöf O, Willi U, Åhström L. Veno-Occlusive Disease and Peliosis of the Liver Complicating the Course of Wilms’ Tumour. Acta Radiologica Diagnosis. 1985; 26(5): 589-597. doi:10.1177/028418518502600515
- Corbacioglu S, Carreras E, Ansari M, Balduzzi A, Cesaro S, Dalle JH, et al. Diagnosis and severity criteria for sinusoidal obstruction syndrome/veno-occlusive disease in pediatric patients: a new classification from the European society for blood and marrow transplantation. Bone Marrow Transplant. 2018; 53(2): 138145. doi: 10.1038/bmt.2017.161. Epub 2017 Jul 31. PMID: 28759025; PMCID: PMC5803572.
- Cesaro S, Pillon M, Talenti E, et al. A prospective survey on incidence, risk factors and therapy of hepatic veno-occlusive disease in children after hematopoietic stem cell transplantation. Haematologica. 2005; 90(10): 1396-1404.
- Elli M, Pinarli FG, Dagdemir A, Acar S. Veno-occlusive disease of the liver in a child after chemotherapy for brain tumor. Pediatr Blood Cancer. 2006; 46(4): 521-523. doi:10.1002/pbc.20338.
- Ishaqi MK, Jamil A, Khanani M, et al. Hepatic Sinusoidal Obstruction Syndrome in a child after chemotherapy for medulloblastoma. J Neurooncol. 2010; 97(1): 137-141. doi:10.1007/s11060-009-9996-z.
- McAtee CL, Schneller N, Brackett J, Bernhardt MB, Schafer ES. Treatment-related sinusoidal obstruction syndrome in children with de novo acute lymphoblastic leukemiaduring intensification. Cancer Chemother Pharmacol. 2017; 80(6): 1261-1264. doi:10.1007/s00280-017-3453-z.
- AlSaad T, Yousif T, Saleh A, Ahmed H, Cole C, Cugno C. Hepatic sinusoidal obstruction syndrome post-chemotherapy in pediatric and adolescent age: case series of six patients in Qatar. Ann Hematol. 2022; 101(3): 693-695. doi:10.1007/s00277-021-04526-8.
- Dalle JH, Giralt SA. Hepatic Veno-Occlusive Disease after Hematopoietic Stem Cell Transplantation: Risk Factors and Stratification, Prophylaxis, and Treatment. Biol Blood Marrow Transplant. 2016; 22: 400.
- El-Sayed MH, El-Haddad A, Fahmy OA, et al. Liver disease is a major cause of mortality following allogeneic bone-marrow transplantation. Eur J Gastroenterol Hepatol. 2004; 16: 1347.
- Corbacioglu S, Cesaro S, Faraci M, et al. Defibrotide for prophylaxis of hepatic veno-occlusive disease in paediatric haemopoietic stem-cell transplantation:an open-label, phase 3, randomised controlled trial. Lancet. 2012; 379: 1301-1309.
- Lee AC, Aung L. Treatment of hepatic veno-occlusive disease in children with N-acetylcysteine. Pediatr Blood Cancer. 2019; 66(2): 27518. doi:10.1002/pbc.27518.