
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Unilateral hypoglossal nerve paralysis after microlaryngeal surgery
Márcia Mourão1*; Inês Dinis2; Gonçalo Quadros1; Clarinda Neves2; Sérgio Raposo1; Filipe Rodrigues1
1Department of Otorhinolaryngology, Tondela-Viseu Hospital Center, Portugal.
2Department of Anesthesiology, Tondela-Viseu Hospital Centeru, Portugal.
*Corresponding Author : Márcia Mourão
Department of Otorhinolaryngology, Tondela-Viseu Hospital Center, Portugal.
Email: marciaczmourao@gmail.com
Received : Jan 02, 2024
Accepted : Jan 22, 2024
Published : Jan 29, 2024
Archived : www.jcimcr.org
Copyright : © Mourão M (2024).
Keywords: Hypoglossal nerve paralysis; Microlaryngeal surgery; Orotracheal intubation; Suspension laryngoscopy.
Citation: Mourão M, Dinis I, Quadros G, Neves C, Raposo S et al. Unilateral hypoglossal nerve paralysis after microlaryngeal surgery. J Clin Images Med Case Rep. 2024; 5(1): 2826.
Introduction
The invasive airway approach, such as orotracheal intubation, laryngeal mask placement and suspension laryngoscopy for laryngeal microsurgery, may result in neurological complications in the postoperative period [1,2]. Although uncommon, unilateral or bilateral nerve injuries, namely of the recurrent laryngeal nerve, hypoglossal nerve and lingual nerve, may decrease the quality of life of patients [1]. Neurological deficit can be classified as: temporary in the form of neuropraxia, with complete recovery expected; or permanent with partial recovery or no recovery of function. The extent and duration of the injury will dictate the underlying deficit [3]. In this article, the authors describe a case of unilateral lesion of the hypoglossal nerve after suspension microlaryngoscopy for excision of a polypoid lesion in the left vocal cord.
Case report
Male patient, 47 years old, without associated pathologies, underwent suspension microlaryngoscopy for the excision of a polyp on the left vocal cord under Balanced General Anesthesia. The initially proposed procedure was excision with CO2 laser. After anesthesia induction, manual ventilation was performed without difficulties, followed by direct laryngoscopy with Macintosh blade number 4. A BURP maneuver was needed to improve the visualization of the glottic cleft. Successful intubation was achieved with a size 5.0 orotracheal tube for laser surgery. The patient underwent invasive mechanical ventilation with high respiratory frequency and low tidal volumes. Subsequently, the BoyceJackson position was assumed, and the rigid laryngoscope (Kleinsasser Laryngoscope) was introduced to optimize the surgical field. However, exposure was challenging, requiring multiple adjustments of the rigid laryngoscope and cervical extension. Additionally, from an anesthetic standpoint, mechanical ventilation was challenging due to upper airway resistance, resulting in a very high peak pressure (Peak 39-40 mmHg). Therefore, the anesthetic-surgical decision was to alter the initial surgical plan and perform conventional suspension microlaryngoscopy. The patient was extubated to replace the laser tube for a microlaryngeal orotracheal tube size 6.0. A new intubation was carried out, requiring the BURP maneuver, and was successful. After confirming tube placement, the endotracheal tube balloon was inflated without exceeding 20 cm H2O. Following intubation, there was a marked improvement in mechanical ventilation. The rigid laryngoscope was reintroduced and suspended, and the surgery was initiated, which involved the cold resection of the polypoid lesion on the left vocal cord. Surgery lasted a total of 50 minutes and underwent without complications. The anesthetic emergence was smooth, without incident.
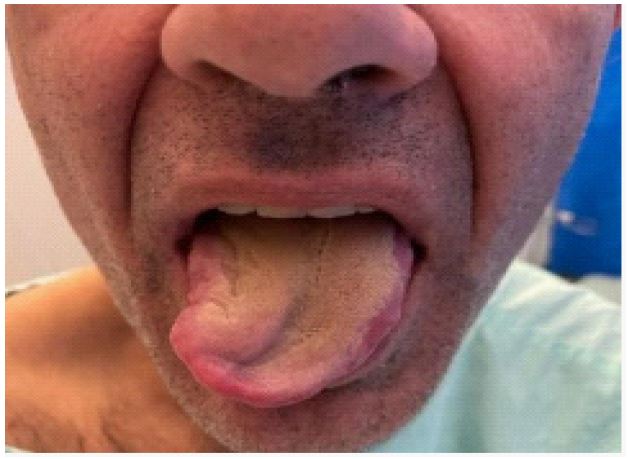
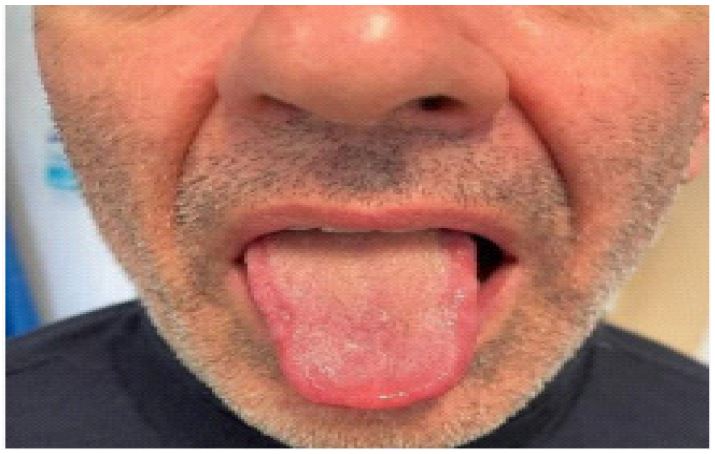
In the ward, the patient showed limited tongue mobility to the right and upon tongue protrusion, right deviation (Figure 1). Neurological and otorhinolaryngological examination, including the assessment of the remaining cranial nerves, revealed no other motor or sensory deficits. Flexible nasopharyngolaryngoscopy showed slight edema at the base of the tongue at the right side, with maintained and symmetric vocal cord mobility and pharyngeal sensitivity preserved. The remaining examination did not show other functional or structural alterations in the otorhinolaryngological territory. On the same day, the patient underwent a cranial-encephalic CT scan to rule out a central etiology. After excluding a central cause, the diagnosis of isolated hypoglossal nerve paralysis was finally assumed. The patient started oral corticosteroids (prednisolone 60 mg, once daily) for 10 days, followed by weaning, and Neurobion® (B1, B6, and B12 vitamin complex) until complete recovery of nerve function, which occurred 8 weeks after the surgical intervention (Figure 2).
Discussion
The hypoglossal nerve, XII cranial nerve, emerges from the medulla oblongata and leaves the cranial cavity through the hypoglossal canal. Then, on the lateral prominence of the anterior aspect of the transverse process of the first cervical vertebra (C1), it crosses the vagus nerve and begins its downward spiral path between the great vessels of the neck. At the angle of the mandible, the nerve runs under the posterior belly of the digastric muscle, in close proximity of the great cornu of the hyoid bone. Then, it enters the oral cavity to innervate all the intrinsic and extrinsic muscles of the tongue, except the palatoglossus [2,3]. Damage to the hypoglossal nerve compromises the motor function of the tongue with a deviation of the tongue towards the affected side, which can cause mild dysphagia and dysarthria [2]. Since unilateral hypoglossal nerve injury is generally well tolerated and compensated, this complication may go unnoticed in the postoperative period, especially when vocal rest is recommended [2].
Suspension laryngoscopy is a surgical procedure commonly performed for the diagnosis and treatment of laryngeal pathologies, which may be associated with minor complications such as dental, oral mucosal or lip lesions and temporary difficulty in swallowing or breathing, and major complications such as pneumothorax, need for emergent tracheotomy, and cardiovascular complications. Besides that, complications such as cranial nerve injuries, mostly lingual nerve injuries, have been described in the literature [4]. Isolated hypoglossal nerve injury associated with laryngoscopy and tracheal intubation is a rare complication with multifactorial cause, with anatomical and technical factors involved [1,2]. Occasionally, hypoglossal nerve and recurrent laryngeal nerve paresis may occur, and this is known as Tapia Syndrome [3].
Several mechanisms of hypoglossal nerve injury have been described. Dziewas et al. presented a series of 25 patients with hypoglossal lesions and six of these patients had undergone suspension laryngoscopy. They proposed as a mechanism of injury the direct compression of the nerve along its superficial course at the lateral root of the tongue [5]. Another mechanism described is anterior displacement of the tongue during laryngoscopy, which can cause tension on the hypoglossal nerve [6]. Baumgarten et al. suggest that nerve injury may occur due to nerve compression between the laryngoscope blade and the hyoid bone [7]. Evers et al. reported the pressure applied to the cricoid during airway approach as a possible risk factor [8]. In addition to injury mechanisms described, hyperextension of the neck during airway approach or manipulation of the head during surgeries may cause stretching of the hypoglossal nerve against the lateral prominence of the transverse process of C1 [9]. The duration of surgery, with the laryngoscope in suspension, also appears to be a causal factor [10].
The therapeutic approach on the acute phase consists of the administration of systemic corticosteroids for 10-14 days and, additionally, B1, B6, and B12 vitamin complex for a period for up to 3 months [3]. In our case, the treatment combination proved to be effective in the functional recovery of the nerve.
In this case, unilateral neuropraxia of the hypoglossal nerve (according to Seddon’s classification [11]. Occurred after suspension laryngoscopy for laryngeal microsurgery with orotracheal intubation. Several factors may have contributed to this injury, such as: positioning of the patient with hyperextension of the neck for surgical field exposure optimization; long surgical time; two attempts at intubation with orotracheal tube replacement; pressure exerted on the cricoid during intubation; compression of the nerve against the hyoid bone and the laryngoscope blade.
Conclusion
In conclusion, it is crucial for surgeons and anaesthesiologists to be aware of the risks of neurological injuries inherent to the manipulation of the airway and the positioning of the head and neck during surgeries. Preventive measures such as careful manipulation of the laryngoscope during intubation and exposure of the surgical field may be useful to reduce the incidence of these lesions [3]. Prompt recognition of the lesion, as well as early start of treatment can contribute to the functional recovery of the nerve [9].
References
- Ulusoy H. et al. Paresia transitória unilateral combinada do Nervo hipoglosso e do Nervo Lingual Após intubação Para Anestesia. Brazilian Journal of Anesthesiology. 2014; 64(2): 124-127.
- Cinar U, Akgul G, Seven H, Celik M, Cinar S, Dadas B. Determination of the changes in the hypoglossal nerve function after suspension laryngoscopy with needle electromyography of the tongue. J Laryngol Otol. 2004; 118(4): 289-93.
- Gevorgyan A, Nedzelski JM. A late recognition of tapia syndrome: a case report and literature review. Laryngoscope. 2013; 123(10): 2423-7.
- Ozdamar OI, Uzun L, Acar GO, Tekin M, Kokten N, Celik S. Risk Factors for Lingual Nerve Injury Associated With Suspension Laryngoscopy. Ann Otol Rhinol Laryngol. 2019; 128(7): 633-639.
- Dziewas R, Ludemann P. Hypoglossal nerve palsy as complication of oral intubation, bronchoscopy and use of the laryngeal mask airway. Eur Neurol. 2002; 47: 239-43.
- Michel O, Brusis T. Hypoglossal nerve paralysis following tonsillectomy. Laryngo-rhino-otologie. 1990; 69:.267-70.
- Baumgarten V, Jalinsky W, Bhom S, Galle E. Hypoglossal paralysis after septum correction with intubation anesthesia. Anesthetist. 1997; 46: 34-7.
- Evers K, Eindhoven GB, Wierda JM. Transient nerve damage following intubation for transsphenoidal hypophysectomy Can J Anaesth. 1999; 46: 1143-5.
- Coninckx M, Cardoen S, Hemelsoet D. Tapia’s syndrome in the intensive care unit: a rare cause of combined cranial nerve palsy following intubation. Acta Neurol Belg. 2015; 115(4): 533-7.
- Corvo MA, Inacio A, Mello MB, Eckley CA, Duprat Ade C. Extra-laryngeal complications of suspension laryngoscopy.Braz J Otorhinolaryngol. 2007; 73: 727-732.
- Graff-Radford SB, Evans RW. Lingual nerve injury. Headache. 2003; 43(9): 975-83.