
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Series - Open Access, Volume 5
Sweet syndrome associated with ulcerative colitis treated with ustekinumab: Case report
Laura Melotti1*; Nikolas Konstantine Dussias1; Federico Bardazzi3; Fernando Rizzello1,2; Paolo Gionchetti1,2
1Department of Medical and Surgical Sciences, University of Bologna, Italy.
2IBD Unit, IRCCS University Hospital Policlinico Sant’Orsola-Malpighi, Bologna, Italy.
3Hospital of Bologna Sant Orsola Polyclinic Dermatology, IRCCS University, Italy.
*Corresponding Author : Laura Melot
Department of Medical and Surgical Sciences, University of Bologna, Modena, Italy.
Tel: +39 3291336071.
Email: Laura.melotti2@studio.unibo.it
Received : Jan 03, 2024
Accepted : Jan 25, 2024
Published : Feb 01, 2024
Archived : www.jcimcr.org
Copyright : © Melotti L (2024).
Abstract
Introduction: Acute febrile neutrophilic dermatosis, also known as Sweet Syndrome (SS), is a rare inflammatory disorder that can be associated with IBD and it is considered as an extraintestinal manifestation. A systematic review in 2021 described 95 known cases.
Case report: We report the cases of two patients with Ulcerative Colitis-related SS. The patients are two females, 49 and 55 years of age, with ulcerative colitis. Due to the an acute disease flare, they were started on infliximab therapy, but after the induction phase, they developed skin lesions suspected of SS. Biopsies were performed and they were diagnostic for neutrophilic dermatosis in one case, and an histiocytoid variant in the other.
Skin lesions disappeared after a course of systemic steroids but reappeared during steroid tapering. Because of this, the decision was made to initiate treatment with ustekinumab, an anti-IL12/23 monoclonal antibody approved for the treatment of both the cutaneous and intestinal disease. Both patients achieved steroid-free clinical remission.
Conclusion: In conclusion, ustekinumab can be a valid treatment in cases of SS associated with IBD and should be considered in steroidrefractory or dependent diseases.
Citation: Melotti L, Dussias NK, Bardazzi F, Rizzello F, Gionchetti P. Sweet syndrome associated with ulcerative colitis treated with ustekinumab: Case report. J Clin Images Med Case Rep. 2024; 5(2): 2828.
Background
Inflammatory Bowel Diseases (IBD) frequently develop Extra-Intestinal Manifestations (EIMs) that affects predominantly joints, skin and eyes. The most frequent cutaneous manifestations are pyoderma gangrenosum and erythema nodosum [1]. Acute febrile neutrophilic dermatosis, also known as Sweet Syndrome (SS), is a rare cutaneous manifestation that occurs between 0.07% and 0.21% of IBD patients [2,3]. A recent systematic review by Sleiman et al. collected a total of 95 cases of IBD-associated SS [4]. We report the cases of two patients with Ulcerative Colitis (UC) - associated SS that were treated with ustekinumab. To our knowledge, these are the first cases described where ustekinumab was able to effectively deal both conditions.
Narrative
Case 1
The patient is a 55-year-old caucasian female affected by distal Ulcerative Colitis (UC), diagnosed in 2016. Past medical history is otherwise unremarkable, she has not EIMs and she takes no chronic medications except for mesalamine for maintenance of UC remission. Family history was negative for IBD and autoimmune disorders.
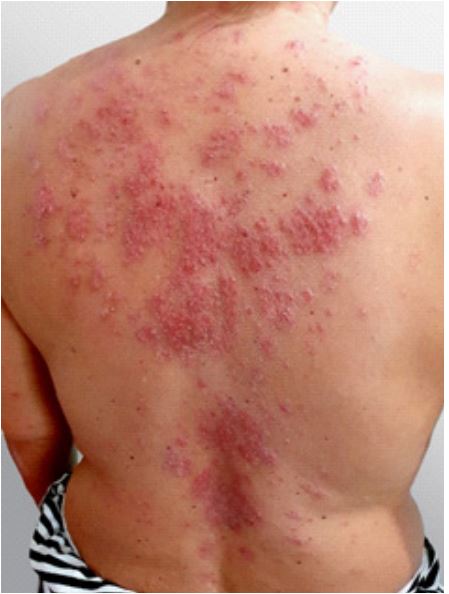
After a stressful life event, the patient experienced a severe disease flare, characterized by abdominal pain and bloody diarrhea. It was confirmed endoscopically and histologically and required hospitalization with intravenous steroid treatment. Due to the subsequent development of steroid-resistance, biological treatment with anti-TNFalfa (infliximab) was initiated. After the second administration of infliximab, the patient presented two self-limiting febrile episodes (39°C). Concurrently, intensely itchy, erythematous plaques appeared on the extensor surfaces of the upper limbs (Figure 1) and papules on the thighs. In the following days, these lesions merged into infiltrating plaques with vesiculobullous elements. The lesions appeared also on the patient’s back, were hard to the touch and non-painful. Laboratory exams revealed anemia (Hemoglobin 10.6 g/dL), relative neutropenia (31,8%), lymphocytosis (56,4%) and monocytosis (12,5 %), piastrinosis (402000/mmc) and elevated inflammatory markers (C-reactive Protein 1,8 mg/dL, ESR 48 mm/h); findings compatible in part with active ulcerative colitis. As the clinical picture was suspect for Inflammatory Bowel Disease (IBD)-related Sweet Syndrome (SS), with onset after the initiation of infliximab, treatment was suspended and the patient was started on intravenous steroids.
Cutaneous biopsy of a lesion of the arm was performed, confirming histiocytoid-variant Sweet syndrome (dermal edema with subdermal dense inflammatory infiltrate with a prevalence of histiocytes and sparse lymphocytes, neutrophils and eosinophils; histiocyte intracytoplasmic cellular debris, absence of vasculitis).
The patient’s UC-related symptoms were poorly controlled with corticosteroids, moreover cutaneous lesions reappeared on the upper limbs during steroid tapering, even after anti-TNFalfa suspension. Therefore, we decided to start ustekinumab (390 mg intravenous at induction followed by 90 mg subcutaneous as scheduled for UC).
After one year, the patient is in clinical remission for UC (Partial Mayo score <2) [5] without steroids and the skin lesions are disappeared.
Case 2
The patient is a 49-year-old caucasian female, diagnosed with ulcerative pancolitis in 2010. Past medical history was unsignificant and she has no EIMs. Family history was negative for IBD and autoimmune disorders. UC was previously treated with infliximab and azathioprine, suspended after achieving sustained clinical and endoscopic remission. After the patient experienced a disease flare with concomitant Clostridium difficile colitis, the patients was started on a second course of infliximab, following treatment for c. difficile infection. The treatment was successful leading to UC remission.
Approximately one month after the fifth infusion of infliximab, the patient presented with erythematous-desquamative cutaneous lesions and diffuse pustules on the scalp, thorax and limbs (Figure 2). Laboratory exams revealed mild anemia (Hemoglobin 11.2 g/dL), relative neutrophilia (85%) and elevate inflammatory biomarker (C-reactive Protein 2.1 mg/dL). Biopsy of a lesion of the left leg revealed hyperkeratosis, intracorneal neutrophils, epidermal spongiosis, dermal edema and a dense interstitial infiltrate in the papillary and reticular dermis rich in lymphocytes, neutrophils, rare eosinophils and numerous macrophages containing intracytoplasmic cell debris; findings compatible with neutrophilic dermatosis.
The patient received systemic steroids with initial resolution of the lesions, which reappeared during steroid tapering. Suspecting a correlation between infliximab treatment and the development of Sweet syndrome, the patient was switched initially to vedolizumab; however, the skin lesions persisted, so vedolizumab was suspended and the patient was treated with a second course of oral steroids. In the following months, she developed a steroid-dependent ulcerative colitis, thus a treatment with ustekinumab (390 mg intravenous at induction followed by 90 mg subcutaneous as scheduled for UC) was started. After one year, the patient is in clinical remission for UC (Partial Mayo score <2) without steroids and the skin lesions are disappeared.

Discussion
These cases show how two rare associated diseases can be treated with an unique therapy. Patients are middle-aged female as it is more frequently described [4]. Both UC and SS was active at the time of ustekinumab initiation, and both improved rapidly. Probably, there are no previous cases regarding the use of ustekinumab for UC-related SS due to the recent approval of ustekinumab for UC. There is only one case described in which ustekinumab was used for treatment of Crohn’s Disease-related SS [6], but it was not effective in terms of resolution of skin lesions and achievement of clinical remission for Crohn’s Disease according to Harvey Bradshaw Index [7]. The initial suspicion of infliximab-inducted SS in both cases was excluded because of the non-resolution of skin lesions after drug withdrawal and the worsening during steroid tapering. The purpose of this case report is dual: firstly, to reinforce available literature on rare and neglected association between two rare diseases, secondly to describe the effectiveness of a new therapy as ustekinumab for these conditions.
The main limitation is, due to the chronicity of the diseases, the short time of follow-up.
Conclusion
IBD-related SS is a rare disease that can be a heavy burden for patients and challenging for physician mostly in cases in which they do not respond to steroids and/or anti-TNFalfa monoclonal antibody. In these cases, we showed how ustekinumab can be a valid alternative option and should be considered in case of steroid-dependent or refractory diseases.
References
- Rogler G, Singh A, Kavanaugh A, Rubin DT. Extraintestinal Manifestations of Inflammatory Bowel Disease: Current Concepts, Treatment, and Implications for Disease Management. Gastroenterology. 2021; 161(4): 1118-1132. doi:10.1053/J.GASTRO.2021.07.042
- Ko JS, Uberti G, Napekoski K, Patil DT, Billings SD. Cutaneous manifestations in inflammatory bowel disease: a single institutional study of non-neoplastic biopsies over 13 years. J Cutan Pathol. 2016; 43(11): 946-955. doi: 10.1111/CUP.12777.
- Cleynen I, Van Moerkercke W, Billiet T, et al. Characteristics of skin lesions associated with anti-tumor necrosis factor therapy in patients with inflammatory bowel disease: A cohort study. Ann Intern Med. 2016; 164(1): 10-22. doi:10.7326/M15-0729.
- Sleiman J, Hitawala AA, Cohen B, et al. Systematic Review: Sweet Syndrome Associated with Inflammatory BowelDisease. J Crohns Colitis. 2021; 15(11): 1864. doi:10.1093/ECCO-JCC/JJAB079.
- Lewis JD, Chuai S, Nessel L, Lichtenstein GR, Aberra FN, Ellenberg JH. Use of the Non-invasive Components of the Mayo Score to Assess Clinical Response in Ulcerative Colitis. Inflamm Bowel Dis. 2008; 14(12): 1660. doi:10.1002/IBD.20520
- de Risi-Pugliese T, Seksik P, Bouaziz JD, et al. Ustekinumab treatment for neutrophilic dermatoses associated with Crohn’s disease: A multicenter retrospective study. J Am Acad Dermatol. 2019; 80(3): 781-784. doi:10.1016/J.JAAD.2018.06.065
- Harvey RF, Bradshaw JM. A simple index of Crohn’s-disease activity. Lancet (London, England). 1980; 1(8167): 514. doi: 10.1016/S0140-6736(80)92767-1.