
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Unusual manifestation of pancreatic cancer in a young patient
Syed Ali Arsal1; Abdul Raheem2*; Chand kumar3; Mehwish Soomro1; Syed Muhammad Sinaan Ali3; Ashish kumar1
1Shaheed Mohtarma Benazir Bhutto Medical College, Lyari Hospital Rd, Rangiwara Karachi, Karachi, Pakistan.
2Baqai Medical University, P.O Box No 2407, Karachi - 75340, Pakistan.
3Liaquat National Hospital & Medical College, Stadium Road, Karachi, Pakistan.
*Corresponding Author : Abdul Raheem
Baqai Medical University, P.O Box No 2407, Karachi -
75340, Pakistan.
Tel: +923322062637;
Email: abdulraheem7712@gmail.com
Received : Jan 05, 2024
Accepted : Jan 25, 2024
Published : Feb 01, 2024
Archived : www.jcimcr.org
Copyright : © Raheem A (2024).
Abstract
Pancreatic cancer, often described as the most devastating among cancers, characterized by a malignant tumor with a grim prognosis and a limited response to systemic therapy. Its characterization is common in old age and very rare and unusual in the young age. We present an unusual case of a male patient, 35 years old. A case of diabetes and of pancreatic cancer in the head of the pancreas with stomach and bone metastases, highlighting its diagnostic challenges and management. The patient presented with changed bowel habits for a month, generalized body aches for a week, hip joint pain with decreased mobility for a week, decreased oral intake for three to four days, and hematuria for two days. The patient complained of irregular bowel habits, which included fatty and oily feces, minor abdominal discomfort, and intermittent constipation. According to the patient, he developed generalized bone pain in upper as well as lower back unlike usually present in pancreatic cancer. A contrast-enhanced CT scan of the abdomen and pelvis revealed indications of a heterogeneously enhancing lesion in the pancreatic head, with an interior necrotic component measuring 32x31 mm and generating a substantial dilatation of the pancreatic duct and CBD. A tentative diagnosis of pancreatic cancer in the head of the pancreas with stomach and bone metastases was made based on clinical history and testing. Given the poor prognosis associated with pancreatic cancer patients, the patient was admitted for conservative and palliative care. This case emphasizes the rarity of pancreatic cancer in young patients and that further research is needed to understand its epidemiology and etiology.
Keywords: Pancreatic cancer; PDAC (Pancreatic Ductal Adenocarcinoma); Global incidence; Multimodal therapies; Jaundice; Weight loss; Neoadjuvant therapy; Minimally Invasive Pancreaticoduodenectomy (MIPD); Microrna (Mirna); PALN (Para-Aortic Lymph Node) Metastasis; Prognosis; Spinal involvement; ERCP (Endoscopic Retrograde Cholangiopancreatography); Conservative and palliative care; Chemoradiation; Metastasis; Diagnostic imaging; Stent placement; Exocrine tumors; Pain management.
Citation: Arsal SA, Raheem A, Kumar C, Soomro M, Ali SMS, et al. Unusual manifestation of pancreatic cancer in a young patient. J Clin Images Med Case Rep. 2024; 5(2): 2829.
Introduction
Pancreatic cancer, often dubbed the “king of cancer,” exhibits rising global incidence and mortality rates annually, with poor prognosis and limited efficacy from current diagnostic and treatment modalities [1]. In primary care, the sole notable red flag for pancreatic cancer is jaundice, a symptom that undeniably calls for further investigation [2]. If weight loss is coupled with another symptom, it might necessitate investigation, likely involving abdominal computed tomography [2]. Despite advances in multimodal therapies, surgery remains the only potential for long-term cure in Pancreatic Ductal Adenocarcinoma (PDAC), with palliative surgery being crucial due to a substantial number of patients presenting in advanced disease stages [3]. Pancreatic adenocarcinoma is a very deadly cancer, and while neoadjuvant chemo (radio) therapy is suggested for borderline resectable and high-risk resectable cases, there is a lack of strong supporting evidence [4].
This disease is often identified in advanced stages, precluding curative surgery [5], and while chemotherapy is the prevalent approach for advanced pancreatic cancer, it demonstrates limited effectiveness, making targeted therapy and immunotherapy, which have shown promise in various cancers, potentially hopeful options for treating pancreatic cancer [5]. Minimally Invasive Pancreaticoduodenectomy (MIPD) is considered safe and viable for specific elderly patients when conducted by skilled surgeons in high-volume pancreatic surgery centers, with a rising trend in its utilization for pancreatic head or periampullary lesions [6]. MicroRNA (miRNA), a small non-coding RNA, exhibits diverse aberrant expressions in pancreatic cancer, playing a crucial role in the onset and progression of the disease, highlighting its potential as novel diagnostic, prognostic, and therapeutic targets for pancreatic cancer [7]. The presence of PALN (Para-Aortic Lymph Node) metastasis indicates an advanced stage of tumor growth and lymph node dissemination [8].
Pancreatic cancer’s impact is projected to increase due to both a growing population and the aging demographic [9]. Brain metastasis from pancreatic cancer is uncommon and often leads to a fatal outcome, the data presented in this review suggests that certain patient-specific and treatment-related factors may indicate a more favorable prognosis [10]. Pancreatic cancer rarely spreads to the spine, usually indicating a grim outlook, underscoring the importance of early detection and prompt intervention when spinal involvement is identified [11].
Case presentation
A male patient, 35 years old, known case of diabetes mellitus, made an emergency room visit complaining of changed bowel habits for a month, generalized body aches for a week, hip joint pain with decreased mobility for a week, decreased oral intake for three to four days, and hematuria for two days. The patient complained of irregular bowel habits, which included fatty and oily feces, minor abdominal discomfort, and intermittent constipation. According to the patient he developed generalized bone pain in upper as well as lower back unlike usually present in pancreatic cancer. The patient had previously smoked for 2.5 years, the past nine months of which he had abstained. In addition, he has a beer and Naswar addiction on and off.
The patient’s vitals showed that his temperature was afebrile, his pulse was 82 beats per minute, his blood pressure was 110/60 mmHg, and his oxygen saturation was 92%. The patient was oriented to time, place, and person. He had an emancipated and worn-out appearance, significant generalized weakness, and minor icterus. A minor distension was felt when the abdomen was palpated, but the systemic examination revealed nothing noteworthy.
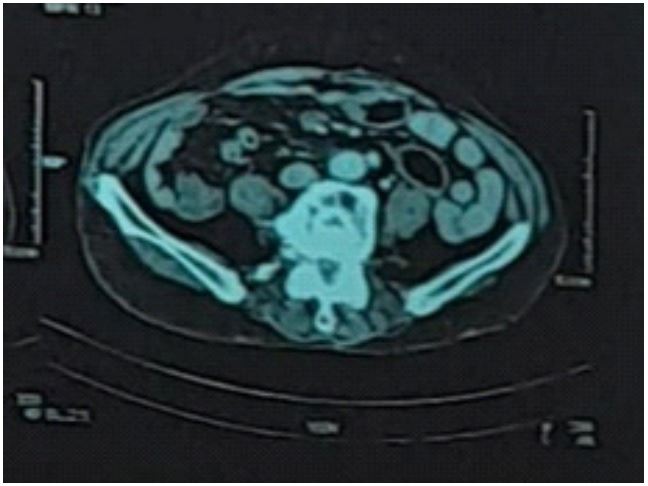
An ultrasound performed on the patient before this inquiry revealed a notable 2.1 cm dilatation of the common bile duct at the porta hepatis and a 1 cm dilatation of the pancreatic duct. As of right now, a contrast-enhanced CT scan of the abdomen and pelvis revealed indications of a heterogeneously enhancing lesion in the pancreatic head, with an interior necrotic component measuring 32x31 mm and generating a substantial dilatation of the pancreatic duct and CBD. There were a few swollen peri-pancreatic lymph nodes seen, the biggest of which measured 9 mm on the short axis in the stomach’s smaller sac. A similar lesion with encasement of splenic arteries and isolated parenchymal infiltration was also seen within the gastrosplenic ligament, infiltrating the splenic hilum and the posterior wall of the stomach body. It was discovered that there were no mass lesions in the liver, gall bladder, kidneys, adrenal glands, lungs, or peritoneum. A small number of lytic spots in the right iliac ischium and plain, however, suggested the possibility of bone metastases as shown in (Figure 1).
A tentative diagnosis of pancreatic cancer in the head of the pancreas with stomach and bone metastases was made based on clinical history and testing. Given the poor prognosis associated with pancreatic cancer patients, the patient was admitted for conservative and palliative care, which included the use of endoscopic retrograde cholangiopancreatography to place a stent, painkillers, antibiotics for any infections, small boluses of water to hydrate the patient, and a diet high in protein. To manage decreased appetite and NG placement, a gastrologic consultation was necessary. Following counseling of the illness, prognosis, and appropriate conservative and palliative care, the patient was discharged from the hospital.
Discussion
Pancreatic cancer, a highly invasive malignant tumor with a fatal risk, is primarily observed in males and older persons (60- 85 years old). It is one of the major causes of cancer-related death. Younger people are becoming more frequently diagnosed with pancreatic cancer. Because the illness can swiftly spread to other tissues and organs and has no early symptoms [12]. Individuals with this illness have a five-year survival rate of about 8% and a median overall survival of fewer than six months. Inadequate techniques for early identification of pancreatic cancer are partly to blame for the disease’s dismal prognosis [13]. Exocrine or endocrine cells may be the source of pancreatic tumors. Consequently, the histological appearance of endocrine and exocrine cancers may be differentiated [14]. Endocrine tumors frequently originate from islet cells of the pancreas and generate excessive amounts of pancreatic hormones constitutively. Depending on the hormones they emit and the type of cell they originated from, they can be further classified as insulinomas, glucagonomas, and gastrinomas [15]. The exocrine tumor which is the main subject of our study accounts most of the occurrence of pancreatic cancers. Pancreatic Ductal Adenocarcinoma (PDAC) is the most common exocrine origin, derived from the epithelial cells present around the ducts and glands [16]. Pancreatic cancer believed to have multifactorial etiology both environmental factors and genetic factors can be culprit for predisposition of the malignancy [17].
The diagnosis is very difficult because there are no cardinal symptoms, and an early screening test is available for pancreatic cancer. However, symptoms like abdominal discomfort, nausea vomiting, back pain, altered bowel habits and new onset diabetes reported by other articles [18] like the presentation of our case. Imaging plays an important role in the diagnosis, treatment and determining prognosis of the disease in which CT scan considered best modality for the non-invasive detection and staging of the cancer [19]. After staging, the clinical management of different cancer stages, the role of radiation therapy varies. For resectable tumors, the preferred approaches involve chemoradiation either before or after surgical resection, with additional consideration given to Stereotactic Body Radiation Therapy (SBRT). In cases of borderline resectable tumors, a similar sequence is followed, emphasizing chemoradiation before or after resection and the potential use of SBRT. Locally advanced cancers may benefit from chemoradiation post-chemotherapy, SBRT post-chemotherapy, or palliative measures. Metastatic disease primarily involves palliative radiation for symptom relief [20].
Like our case, patients with poor prognosis and high-grade disease shows effective results from palliative care and interventions [21], pain management with painkiller and strong analgesics shows improvement in quality and quantity of life [22]. In non-resectable tumors, use of chemo and radiotherapy is very controversial; study gives us data where stent placement in the pancreatic cancer of the head is proven effective in relieving the symptoms of the disease [23].
Strengths and limitations: The case provides an in-depth clinical overview, delineating the patient’s symptoms, medical background, and lifestyle details. The integration of ultrasound and contrast-enhanced CT scan findings offers crucial insights into the pancreatic lesion and potential metastases, facilitating accurate diagnosis and treatment planning. The management strategy showcases a praiseworthy multidisciplinary approach, encompassing interventions like Endoscopic Retrograde Cholangiopancreatography (ERCP), pain control, antibiotic administration, nutritional support, and gastrologic consultation. Notably, the acknowledgment of the grim prognosis associated with pancreatic cancer underscores a patient-centric approach, underscoring the significance of conservative and palliative care. However, the case’s limitations include the absence of specific diagnostic particulars, a comprehensive account of smoking and alcohol history, details about diabetes control, and information on genetic or family history. These shortcomings restrict a more nuanced comprehension of the patient’s overall condition.
Declarations
Statement of author contributions: A.R and M.S wrote the Introduction of the this manuscript. A.K and S.A.A wrote the discussion of the manuscript. S.M.S.A and C.K wrote the case presentation. A.R and S.A.A did the editing and finalization of manuscript.
Funding: The authors received no external funding for this study.
Conflict of interest statement: The authors declare that they have no competing interest and there is no conflict of interest.
References
- Zhonghua Zhong, Liu Za Zhi. Expert consensus on the wholecourse management of home medical care for patients with pancreatic cancer in China. 2022; 44(10): 1076-82.
- Schmidt-Hansen M, Berendse S, Hamilton W. Symptoms of Pancreatic Cancer in Primary Care: A Systematic Review. Pancreas. 2016; 45(6): 814-8.
- Belyaev O, Bösch F, Brunner M, Müller-Debus CF, RadulovaMauersberger O, et al. Indications for Surgery in Pancreatic Ductal Adenocarcinoma - Consensus Recommendations by the German Society for General and Visceral Surgery. Zentralbl Chir. 2020; 145(4): 354-64.
- Pan L, Fang J, Tong C, Chen M, Zhang B, et al. Survival benefits of neoadjuvant chemo(radio)therapy versus surgery first in patients with resectable or borderline resectable pancreatic cancer: A systematic review and meta-analysis. World J Surg Oncol. 2019; 18(1): 1.
- Leowattana W, Leowattana P, Leowattana T. Systemic treatment for advanced pancreatic cancer. World J Gastrointest Oncol. 2023; 15(10): 1691-705.
- Zhu J, Wang G, Du P, He J, Li Y. Minimally Invasive Pancreaticoduodenectomy in Elderly Patients: Systematic Review and MetaAnalysis. World J Surg. 2021; 45(4): 1186-201.
- Ren H, Wang CF. Diagnosis, treatment and prognosis evaluation of pancreatic cancer by microRNA. Zhonghua Zhong Liu Za Zhi. 2020; 42(11): 903-6.
- Hempel S, Oehme F, Müssle B, Aust DE, Distler M, et al. Prognostic impact of para-aortic lymph node metastases in non-pancreatic periampullary cancer. World J Surg Oncol. 2020; 18(1): 16.
- Chen DY, Yang XY, Fan WL, Wang HX, Wang P, et al. Analysis and forecast of burden of pancreatic cancer along with attributable risk factors in Asia countries between 1990 and 2019. Zhonghua Zhong Liu Za Zhi. 2022; 44(9): 955-61.
- De Stefano FA, Morell A, Marks K, Fernandez S, Smith G, et al. Brain Metastasis from Pancreatic Cancer: Our Experience and Systematic Review. World Neurosurg. 2022; 166: e590-e8.
- Rail B, Ogwumike E, Adeyemo E, Badejo O, Barrie U, et al. Pancreatic Cancer Metastasis to the Spine: A Systematic Review of Management Strategies and Outcomes with Case Illustration. World Neurosurg. 2022; 160: 94-101.e4.
- Zhao Z, Liu W. Pancreatic Cancer: A Review of Risk Factors, Diagnosis, and Treatment. Technol Cancer Res Treat. 2020; 19: 1533033820962117.
- Lennon AM, Wolfgang CL, Canto MI, Klein AP, Herman JM, et al. The early detection of pancreatic cancer: What will it take to diagnose and treat curable pancreatic neoplasia? Cancer Res. 2014; 74(13): 3381-9.
- Stefàno E, Cossa LG, De Castro F, De Luca E, Vergaro V, et al. Evaluation of the Antitumor Effects of Platinum-Based [Pt(η(1)-C(2)H(4)-OR)(DMSO)(phen)](+) (R = Me, Et) Cationic Organometallic Complexes on Chemoresistant Pancreatic Cancer Cell Lines. Bioinorg Chem Appl. 2023; 2023: 5564624.
- Fesinmeyer MD, Austin MA, Li CI, De Roos AJ, Bowen DJ. Differences in survival by histologic type of pancreatic cancer. Cancer Epidemiol Biomarkers Prev. 2005; 14(7): 1766-73.
- Halbrook CJ, Lyssiotis CA, Pasca di Magliano M, Maitra A. Pancreatic cancer: Advances and challenges. Cell. 2023; 186(8): 1729-54.
- Vincent A, Herman J, Schulick R, Hruban RH, Goggins M. Pancreatic cancer. Lancet. 2011; 378(9791): 607-20.
- Loveday BPT, Lipton L, Thomson BN. Pancreatic cancer: An update on diagnosis and management. Aust J Gen Pract. 2019; 48(12): 826-31.
- Chu LC, Goggins MG, Fishman EK. Diagnosis and Detection of Pancreatic Cancer. Cancer J. 2017; 23(6): 333-42.
- Koay EJ, Hall W, Park PC, Erickson B, Herman JM. The role of imaging in the clinical practice of radiation oncology for pancreatic cancer. Abdom Radiol (NY). 2018; 43(2): 393-403.
- Chung V, Sun V, Ruel N, Smith TJ, Ferrell BR. Improving Palliative Care and Quality of Life in Pancreatic Cancer Patients. J Palliat Med. 2022; 25(5): 720-7.
- Coveler AL, Mizrahi J, Eastman B, Apisarnthanarax SJ, Dalal S, et al. Pancreas Cancer-Associated Pain Management. Oncologist. 2021; 26(6): e971-e82.
- Kuwatani M, Kawakubo K, Sugimori K, Inoue H, Kamada H, et al. Trial protocol: A randomised controlled trial to verify the noninferiority of a partially covered self-expandable metal stent to an uncovered self-expandable metal stent for biliary drainage during neoadjuvant therapy in patients with pancreatic cancer with obstructive jaundice (PUN-NAC trial). BMJ Open. 2021; 11(7): e045698.