
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Paraplegia and brachial diparesis from Mycobacterium Ulcerans infection: A case report
Horlali Yao Gudjinu*; Abigail Gudjinu
Hohoe Municipal Hospital, P.O. Box 27, Hohoe, Volta Region, Ghana.
*Corresponding Author : Horlali Yao Gudjinu
Hohoe Municipal Hospital, P.O. Box 27, Hohoe Volta
Region, Ghana.
Email: sirhorlali@yahoo.co.uk
ORCID ID: 0000-0001-6244-0720
Received : Jan 05, 2024
Accepted : Jan 26, 2024
Published : Feb 02, 2024
Archived : www.jcimcr.org
Copyright : © Gudjinu HY (2024).
Abstract
Background: We report a case of atypical presentation and misdiagnosed nodular Mycobacterium Ulcerans infection, which was administered the wrong treatment options leading significant delay in treatment. This led to the development of complications of Buruli ulcer disease and probable CNS manifestations of the polyketide toxin of Mycobacterium Ulcerans. The diagnosis was finally corrected at another health facility. However, the patient’s condition had deteriorated considerably and the patient had to endure severe complications that were life threatening.
Case presentation: The patient a 31 years old male, developed lower back pains which was later followed by the occurrence of a nodule over the site of the pain to the at the level of L4 just to the left of the midline. The lesion was unfortunately confused for a furuncle (boil). Incision and drainage was done and antibiotics given. This resulted in an ulcer that would not heal in spite of treatment. He moved to another health facility where he was admitted and with time developed progressive paraparesis, then paraplegia and further brachial diaparesis. Over time he started manifesting clonic-tonic seizures which started from the lower limbs and progressed proximally to the upper limbs. The patient’s consciousness remained intact throughout the period. PCR on wound swab sample confirmed Buruli ulcer disease in the patient. The recommended antibiotics regiment was instituted and the was a gradually resolution of all the signs and symptoms as well as wound healing. Physiotherapy was also added to the management. After a few months the patient was able to return to normal life and even ride bicycles.
Conclusion: An atypical presentation of Buruli ulcer could lead to mis-diagnosis, wrong treatments and life-threatening complications. Progressive paraparesis, paraplegia, brachial diparesis with tonic-clonic seizures is documented here for the first time as possible manifestations/complications arising from a probable mycolactone effects in the CNS. There is the need for further studies into the effect of mycolactone on all body tissues especially the CNS.
Keywords: Buruli ulcer; Paraplegia; Brachial diparesis; Mycolactone; CNS.
Citation: Gudjinu HY, Gudjinu A. Paraplegia and brachial diparesis from Mycobacterium Ulcerans infection: A case Report. J Clin Images Med Case Rep. 2024; 5(2): 2833.
Background
This case report uniquely presents the challenges of a patient (health worker) suffering from a neglected tropical disease which occurred with atypical signs and symptoms (including pains at the site). He sorted for treatmentatreputable health facilities in a highly urban area where he was misdiagnosed and given the wrong treatments. He developed a lot of complications with CNS manifestations of probably the mycolactone toxin. The right diagnosis was made at a health facility in a less developed part of the country where he was also given the appropriate treatment. He recovered fully and has return to normal live after months of management.
Case presentation
The patient is a 31 years-old male (a clinical health worker by profession) presented to the Hohoe Municipal Hospital in February 2018 with general bodily pains of two weeks duration and a chronic ulcer on the lower back. The ulcer developed secondary to an incision and drainage procedure performed on a furuncle five months earlier.
He developed lower back pains in April 2017. This pain persisted in spite of management on analgesics until he developed a furuncle at the lower back. He reported to a clinic in the capital city of Accra (where he was employed as a clinical staff) and was managed with flucloxacillin but there was no improvement. The furuncle was therefore incised and drained in September, 2017 after which he continued with antibiotics therapy and wound dressing. Some minimal debridement was done for the wound to improve healing during one of the wound dressing sessions in Accra. The wound continued to persist with no improvement. The patient earlier on in his life was diagnosed and treated for lymphatic filariasis in his left lower limb. This was treated and has resolved but the limb has a lightly darker skin pigmentation. It is also a bit larger in size.
He was a young man walking with a lot of difficulty, looks chronically ill, not pale but wasted, not icteric, blood pressure was pulse were all within normal ranges. There was an open ulcer at his back around the level of L4 vertebra just to the left of the midline. The ulcer is roughly oval in shape, measuring about 3.5 cm x 5 cm, it is deeply undermined (approximately 3 to 7.5 cm from the edge). The ulcer had a light creamy discharge sometimes mixed with blood. The floor had sloth, base is firm and non-tender.
After days of wound dressing and antibiotics treatment, there was no improvement in his condition. He rather deteriorated. He developed an insidious onset of spastic paraparesis which gradually progressed and transformed into a paraplegia (also spastic). At this point, he could only sit-up in bed with the help of staff and family. Interestingly, sensation for pain, deep and light touch were intact in the affected limbs Figure 1 below shows progression of the disease from the nodular stage to the early stages of healing.

Healed ulcer
This paralysis worsened and advanced further proximally. The patient complained of weakness in the hands and fingers with loss of ability to properly grip objects. Then followed a gradual manifestation of weakness in his upper limbs that worsened with time to the point where he loss the ability to control hands, forearms and lastly the arms. He had then clearly developed a complete brachial diparesis. The brachial diparesis was also spastic. Surprisingly, sensation for pain, deep and light touch were intact in all four limbs. At this point the patient could not sit-up even with support. The respiration system examinations revealed normal findings with no reports of dyspnoea, apnoea nor respiratory arrests.
After a while, we received complains and observed jerky clonic-tonic spasmic contractions of the lower limbs. At the initial stages it was brief and barely observable lasting for less than 20 seconds. Things progressed quickly and it later increased in intensity, duration and gross manifestation. Again, this was initially limited to only the lower limbs but it soon progressed proximally to involve the trunk and the upper limbs. The neck also seemed involved but to a lesser extent. There was however, no photophobia (in fact the patient was nursed on a bed by the window side with plenty of sun light throughout his time of admission). There was no involvement of any facial muscle. Respiration findings continue to remain normal.
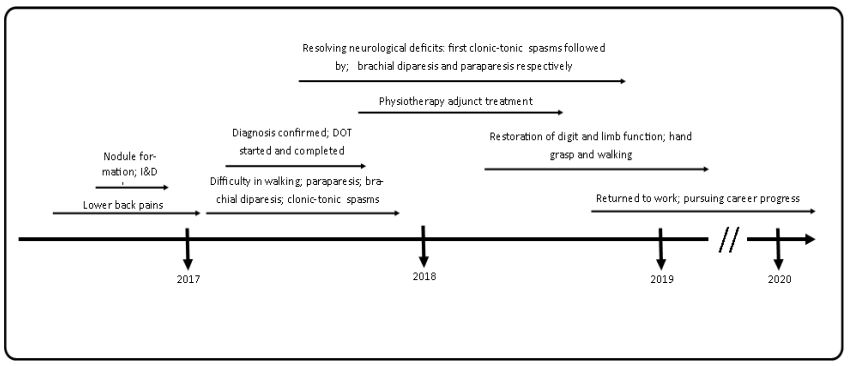
The timeline of key developments in the progression and management of the case is summarized in the figure 2.
From the history, there was not much to help with the diagnosis other that the fact that although he lives in Accra, he sometimes visits his hometown where there is a river. The history of pains and a furuncle at the lower back which was incised and drained but subsequently resulted in an ulcer is a bit misleading/confusing. However, the presence of a chronic highly undermined, tender-less ulcer is highly suggestive of Buruli ulcer regardless of the afore mention history. Although it must be said that the siting of the ulcer is not typical.
Chest and lumbosacral spine x-ray showed no lung changes consistent with pulmonary tuberculosis and no bone involvement as seen in Pot’s disease. Furthermore, to rule out pulmonary tuberculosis Gene X-pert was done for Mycobacterium tuberculosis on saliva specimen and it returned a negative result. Wound swab was taken and sent for PCR testing at the Nugochi Memorial Institute for Medical Research which returned a positive result for Mycobacterium Ulcerans.
Various analgesics were prescribed pains and routine empirical antibiotics given to cover for wound sepsis. The ulcer was dressed under aseptic conditions. It was done initially daily but reduced to alternate day dressing. This was to allow for more rapid wound healing. Minimal wound debridement was done on 10th of April, 2018. Also, there was administration of varies doses of phenobarbitone for the recurrent spasms observed in the lower limbs. At the point when he was having intermittent clonic-tonic contractions, tetanus immunoglobulins were prescribed but the patient could not afford all and this was discontinued.
Once the diagnoses was confirmed as Buruli ulcer, the patient was put on streptomycin capsules 750 mg daily and clarithromycin 600 mg daily for a period of 56 days. The wound healing process was monitored closely and on the 31st May, 2018 the wound edges were directly apposed together with nylon 1 sutures. The patient was then referred to the physiotherapy unit of the hospital where he was put on various interventions while on admonition and subsequently discharged to continue with the physiotherapy sessions on out-patient basis.
Medication was done as Directly Observed Therapy (DOT). The patient was on admission throughout the time of medication. The ulcer, the paraplegia and spasm were monitored during the period of treatment whiles on admission. All these stopped gradually in the reverse order of their individual manifestation starting with the clonic-tonic contractions. This was followed by the resolution of the upper limb weakness then down to the lower limbs. These resolutions where however not fully completed (say <50%) while on admission. The patient was discharged home on the 31st May, 2018 and referred to the Physiotherapy unit of the hospital for adjunct management on out-patient basis. Review was scheduled for two periods following discharge.
The ulcer gradually healed and closed-up the defect with full skin cover. There has been gradual and progressive return to full function in all limbs of the patient. He was able to sit-up and walk once again. This was attendant with improvement in the quality of life of the patient. He was able to pick-up old activities like riding a bicycle and going to the farm. He was able to pursue a return to his clinical career as well. By the time the first halve of the year 2020 it is as if nothing ever happened to him. He is back in Accra working in a clinic. He has also expressed interest in pursuing further education in public health related field.
Discussion and Conclusion
Buruli ulcer disease is endemic or prevalent in warm humid riverine areas as is the case in parts of Sub-Saharan Africa (including Ghana) and Australia [1,2]. This is certainly the case in the part of Hohoe Municipality where the patient visits his parents periodically. Again parts of the Greater Accra Region were in the not too distant past having very high prevalence of Buruli ulcer [3]. It is caused by infection from Mycobacterium Ulcerans. This organism was shown to have evolved from a the aquatic dwelling progenitor Mycobacterium Marinum and developed the ability to produce a toxic immunosuppressing polyketide, mycolatone [4]. The mycolactones produced by M. Ulcerans are also known to be cytotoxic. Most researchers agree that the exact mode/s of transmission of M. Ulcerans is still not very clear [5,6].
The age of the patient is very interestingly close to the mean age of affected people in a nation-wide case search study conducted in 1999 to characterize the problem of Buruli ulcer in Ghana [7]. The initial clinical manifestation of the disease in this patient was a lower back pain with sub-sequent nodule formation. Pain is not recognized as in general symptom for Buruli ulcer but rather the lack thereof (analgesia) [8-10]. Could the rather unusual siting (around the level of L4 vertebra just to the left of the midline over the vertebra). This positioning of Buruli ulcer lesion is hardly documented in literature. It is generally known that the lesions of Buruli ulcer are usually found on the limbs or extremities but now one does wonder why he should manifest pain. Given the siting of the lesion, the tissues of this region are very tightly packed together with limited movement or restriction in movement of tissue. It is our impression that formation of the nodule in this site cause considerable pressure to build-up in the surrounding soft tissue extending into compression of nerve fibres in the region against the prominent bony surfaces of the vertebra bone in the region.
The lesion was clearly misdiagnosed and managed as a regular furuncle with routine antibiotics, incision and drainage which obviously failed to resolve the problem and rather led to the formation of the unintended ulcer that would not heal. It is therefore clear in that this is more of a case of late diagnosis rather than late reporting as is noted in some studies [11,12]. This patient presented very earlier even when apparently no lesion had even developed and yet he suffered almost a worse outcome than those who would report late. He was apparently attended to at many reputable hospitals which failed to identify the problem. But why was this so? Could it have been because of the atypical site of the presentation of the lesion? If the patient had delayed a bit and presented at the ulceration stage rather than the pre-ulcerative stage would the health care system have been able to arrive at the right diagnosis faster? If the afore mentioned should be true then there is cause for serious concern on the surveillance and clinical management for Buruli ulcer in Ghana.
To add to the concert of unusual clinical presentation of this Buruli ulcer is the progressive and ascending paralytic manifestation. The mycolactone of M. Ulcerans has been shown to be able to limit the initiation of primary immune responses as well as the recruitment of inflammatory cells [13]. This facilitates the process of infection by the pathogen with minimal response from the host. Additional to these properties, mycolactones are also diffusible in nature [14]; again, they are able to cause impaired nociception, neurite degeneration and apoptosis which is associated with neural pathology that is observed in clinically induced analgesia [15] and anaesthesia [16]. Considering these peculiar properties of this polyketide toxin (the mycolactone), we are better position to thus explain the observed presentation in this patient.
The ulcer was painless (cutaneous hypoalgesia) in itself superficially, which is standard, common and consistent with most other cases of Buruli ulcer explained by the anti-nociception action of the mycolactone. As the condition progressed and more mycolactone is excreted by the Mycobacterium Ulcerans, the concentration of the mycolactone increases affecting the anatomic structures in the region of the ulcer. This of course in the L4 region includes neuronal fibres exiting out from the vertebra column. These were obviously adversely affected and that in a gradual manner corresponding to dose-response manifestation clinically, starting from weakness in the limbs through paraparesis to complete paraplegia. Beyond this point, as the disease progressed the neuronal declined continued and extended into the upper limbs starting with the weakness in the hands and subsequently symmetrically involving the whole of both upper limbs then progressing into the neck region.
What could account for this phenomenon? The polyketide toxin (mycolactone) has been shown to be diffusible [17] and able to distribute beyond the local site of infection [14,17]. We therefore propose that given the proximity of the affected anatomic structure to the spinal cord which houses spinal column containing spinal fluid; the mycolactone produced at the site of infected diffused from this point of production and higher concentration into the spinal column and the spinal fluid and then build up concentration in the spinal fluid ascending up gradually and manifesting clinically in a dose-response dependent manner gradually with increasing and worsening upper limp weakness progressing to full brachial diparesis. Given more time with no appropriate intervention, it is quite obvious that respiratory muscle function would be impaired through damage to the nerve cells in the spinal cord and possibly cortical brain function interference with the ultimate undesirable outcome of death.
Intermittent tonic-clonic jerky movement of the lower limbs not induced by any obvious stimulus was also documented in this patient. We do not pretend to have an answer to this observation, nevertheless one can not hold-back from realizing the striking resemblance of this clinical manifestation to a tonicclonic focal or regional seizure observed in patients with epilepsy or some other brain injury/condition. There is a remarkable difference however that the patient was fully conscious all the time without exception. Making one to consider; could the mycolactone of M. Ulceran act as or mimic the behaviour of neurotransmitters or rather neurotransmitter-antagonists under certain circumstances say in the CNS or in a ganglion? This is because some studies of this polyketide have already revealed that mycolactones are able to induce hypoesthesia [18] long before causing neuronal degeneration or cell death. We were limited in this regard that we did not have the capacity to test for the mycolactone and its concentrations in the ulcer nor the cerebrovascular fluid. We also had a number of obvious clinical contra-indications to sampling of cerebrovascular fluid in this particular case.
Another point of interest is the nomenclature of the disease. The name “Buruli ulcer” often tend to connote the presence of an ulcer in the disease, while the disease actually has a preulcerative and ulcerative stages. The name could therefore be misleading in many ways. The general populace in the communities as well as less experienced or exposed health staff could be fixated on the ulcer and unconsciously, gradually and surely become more and oblivious of the pre-ulcerative stage of the disease. Again, as access to health service and socio-economic conditions improve one is naturally expecting to have less and less of the late presentations while more and more of the early stages are expected to report for management. Will they suffer the same faith? When that day comes that our surveillance is working well enough such that we hardly see any ulcers at all will it be proper to continue to call it Buruli ulcer or will we at a point consider a change in name such as Buruli or Mycobacterium ulceran disease (rather than the ulcer)?.
We conclude that the patient developed paraplegia with brachial diparesis [19] secondary to a Buruli ulcer infection. This paralytic effect we strongly suspect comes from the M. Ulcerans’ toxin (mycolactone) acting locally on the nervous tissue and distally through diffusion into the CNS transported by the medium of spinal fluid. This case maybe the first ever reported case of possible CNS involvement in-vivo in human by mycolactone. There is a tremendous need for further studies into the mechanism of action of mycolatones in all body tissue especially in the CNS. Again, we can infer that the current treatment modalities are adequate even with possible CNS involvement. Finally, the current WHO classification [20] for Buruli ulcer may not easily accommodated this presentation of Buruli ulcer disease with CNS involvement. The WHO can possibly consider a category IV to make room for cases with CNS involvement. This may draw attention to the severity of the case, priority and urgency of attention it requires in treatment.
Some key lessons from this case include
An atypical presentation of a disease condition as in this case could lead to a complicated diagnostic challenge for the clinicians and a mystical as well as frustrating disease condition for the patient who sort for early treatment and yet fails to achieve cure. The effect of the toxins from Mycobacterium Ulcerans can possibly cause complete blockage, degeneration and or death of motor nerves as well as paralysis. The presence of Buruli ulcer over the spines/back is a potential cause of paralysis that should be treated urgently and aggressively to avoid this CNS involvement and complications. We may have just reported the first case of Buruli ulcer disease with CNS involvement and presentation. Ascending paralysis as in this case with possible respiratory paralysis is a real danger that faces a patient with Buruli ulcer over the spine or close to the CNS.
Declarations
Informed consent: Informed consent for publication was given by the patient on 31st May, 2018.
Ethical considerations: There is no conflict of interest.
Availability of data and materials: The data used in this study is available from the corresponding author on reasonable request.
Funding information: There was no funding received from any organization.
Authors contributions: Author was responsible of coming up with the idea and managing the case as well as the write-up. Co-author: Was responsible for monitoring the process of the reporting, reading, editing and corrections.
Acknowledgement: I greatly acknowledge the only ones who says “For my thoughts are not your thoughts, neither are your ways my ways my ways, saith the LORD. For as the heavens are higher than the earth, so are my ways higher than your thoughts” Isaiah 55: 8-9. Thank you.
Patients perspective: “I knew that I was surely dying! In fact, I had given up and I just wanted to die in peace. I thank God for bringing you to this institution at this time. I know that God certainly has a hand in this. I am so glad. I still hope that I should one day regain full use of my legs. Thank you”.
References
- van der Werf, T S, et al. Mycobacterium Ulcerans disease. Bull. World Health Organ. 2005; 83: 785-791.
- Johnson P D, Veitch M G, Leslie D E, Flood P E, Hayman J A. The emergence of Mycobacterium Ulcerans infection near Melbourne. Med. J. Aust. 1996; 164: 76-78.
- Amofah G, et al. Buruli Ulcer in Ghana: Results of a National Case Search. Emerg. Infect. Dis. 2002; 8: 167-170.
- Doig, K. D. et al. On the origin of Mycobacterium Ulcerans, the causative agent of Buruli ulcer. BMC Genomics. 2012; 13: 258.
- Akoachere J F K T, Nsai F S, Ndip R N A. Community Based Study on the Mode of Transmission, Prevention and Treatment of Buruli Ulcers in Southwest Cameroon: Knowledge, Attitude and Practices. PLOS ONE. 2016; 11: e0156463.
- Marion, E. et al. Seasonal and Regional Dynamics of M. Ulcerans Transmission in Environmental Context: Deciphering the Role of Water Bugs as Hosts and Vectors. PLoS Negl. Trop. Dis. 2010; 4: e731.
- Amofah G, et al. Buruli Ulcer in Ghana: Results of a National Case Search. Emerg. Infect. Dis. 2002; 8: 167-170.
- Yotsu R R, et al. Revisiting Buruli ulcer. J. Dermatol. 2015; 42: 1033-1041.
- Signs and Symptoms. Buruli Ulcer. NCEZID. 2018. https://www.cdc.gov/buruli-ulcer/signs-symptoms.html.
- Buruli ulcer. Mycobacterium-ulcerans-infection. https://www.who.int/news-room/fact-sheets/detail/buruli-ulcer-.
- Abass K M, et al. Buruli Ulcer Control in a Highly Endemic District in Ghana: Role of Community-Based Surveillance Volunteers. Am. J. Trop. Med. Hyg. 2015; 92: 115-117.
- Enhancing Buruli ulcer control in Ghana through social interventions: A case study from the Obom sub-district BMC Public Health. Full Text. https://bmcpublichealth.biomedcentral.com/articles/10.1186/1471-2458-13-59.
- Coutanceau E, et al. Selective suppression of dendritic cell functions by Mycobacterium Ulcerans toxin mycolactone. J. Exp. Med. 2007; 204: 1395-1403.
- Guenin-Macé L, Ruf M T, Pluschke G, Demangel C. Mycolactone: More than Just a Cytotoxin. In Buruli Ulcer: Mycobacterium Ulcerans Disease (eds. Pluschke, G. & Röltgen, K.) 117-134 (Springer International Publishing. 2019. doi:10.1007/978-3-030-11114-4_7.
- Anand U, et al. Mycolactone-mediated neurite degeneration and functional effects in cultured human and rat DRG neurons: Mechanisms underlying hypoalgesia in Buruli ulcer. Mol. Pain. 2016; 12: 1744806916654144.
- Zavattaro E, et al. Apoptosis in Buruli ulcer: A clinicopathological study of 45 cases. Histopathology. 2012; 61: 224-236.
- Hong H, et al. Mycolactone Diffuses from Mycobacterium Ulcerans-Infected Tissues and Targets Mononuclear Cells in Peripheral Blood and Lymphoid Organs. PLoS Negl. Trop. Dis. 2008; 2: e325.
- Marion, E. et al. Mycobacterial Toxin Induces Analgesia in Buruli Ulcer by Targeting the Angiotensin Pathways. Cell. 2014; 157: 1565-1576.
- Figueiredo N, Figueiredo I, Resnick D. Tetraplegia or paraplegia with brachial diparesis? What is the most appropriate designation for the motor deficit in patients with lower cervical spinal cord injury? Neurol. Sci. Off. J. Ital. Neurol. Soc. Ital. Soc. Clin. Neurophysiology. 2012; 34.
- WHO. Buruli ulcer. Mycobacterium-ulcerans-infection. https://www.who.int/news-room/fact-sheets/detail/buruli-ulcer.