
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 5
A tale of noisy airways: Asthma or not?
Kutty Sharada Vinod1*; Vasudha Goel2
1Consultant Internal medicine and Pulmonology, Karuna Hospital, Dilshad Colony, Delhi-110095, India.
2Consultant Gastroenterology, Kailash Deepak Hospital, Delhi-110092, India.
*Corresponding Author : Kutty Sharada Vinod
Consultant Internal medicine and Pulmonology, Karuna Hospital, Dilshad Colony, Delhi-110095, India;
Kailash Deepak Hospital, Delhi-110092, India.
Tel: +918826370686;
Email: Sharada.vinod@gmail.com
Received : Jan 05, 2024
Accepted : Jan 26, 2024
Published : Feb 02, 2024
Archived : www.jcimcr.org
Copyright : © Vinod KS (2024).
Abstract
Citation: Vinod KS, Goel V. A tale of noisy airways: Asthma or not?. J Clin Images Med Case Rep. 2024; 5(2): 2835.
Background
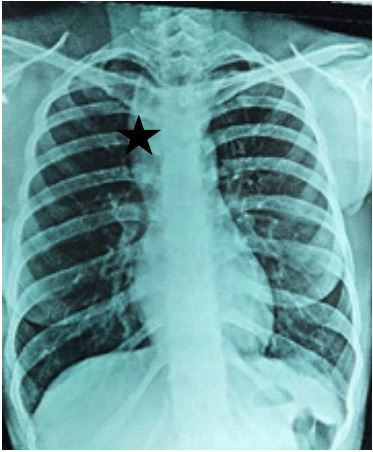
A young female in her early twenties presented with complaints of sneezing, nocturnal dry cough, chest tightness and occasional nocturnal wheeze. She reported occasional reflux symptoms. She denied loss of weight, loss of appetite or fever. She gave a history of biomass fuel exposure. The duration of symptoms was for a period of one and half years. She denied history of any new exposures or change in residence prior to onset of symptoms. She reported partial relief with inhaled bronchodilators. On examination, she had a BMI of 18.76 Kg/m2 . She was hemodynamically stable. A general examination and that of individual systems was normal. The patient’s baseline blood investigations were normal. There was no evidence of peripheral eosinophilia. A chest X-ray was performed which showed a convex opacity overlapping the mediastinum on the right side (Figure 1).
In view of the respiratory symptoms and the imaging findings, a posterior mediastinal pathology was suspected. The patient was advised a pulmonary function test and a CT chest.
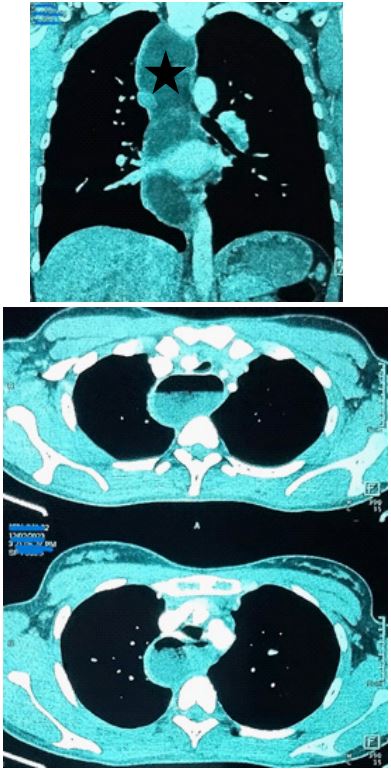
A CT chest done revealed a dilated thoracic esophagus along its entire extent with smooth tapering of the GE junction (Figures 2a and 2b). Note was also made of few centrilobular nodules in bilateral upper lobes.
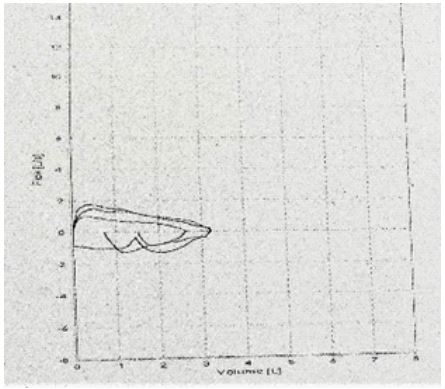
Since the patient had presented with respiratory symptoms, a pulmonary function test was performed. The test revealed, an FEV1 of 1.62 L (59.34%), FVC of 3.02 L (96.49%), and an FEV1/ FVC ratio of 53.64. There was no bronchodilator reversibility. There was plateauing of the inspiratory and expiratory limbs (Figure 3).
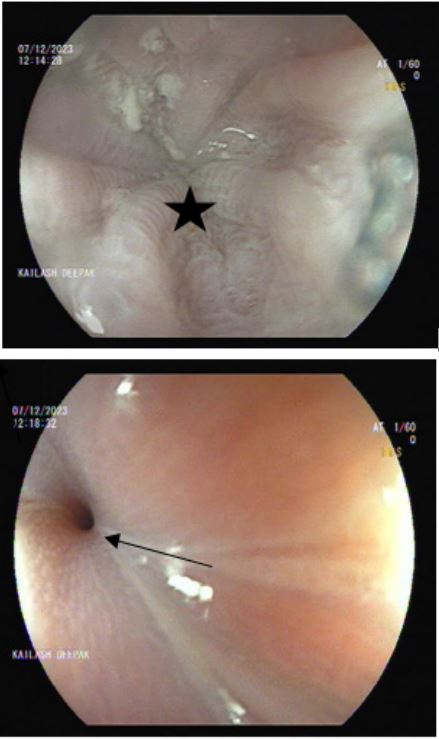
In view of the imaging findings, an upper GI endoscopy was performed that revealed, a dilated esophagus with hyperemic mucosa and residual food contents. Resistance was noted at the Lower esophageal sphincter (Figure 4a and 4b).
On the basis of clinicoradiological and endoscopic findings, the patient was diagnosed with achalasia cardia.
Declarations
Achalasia is an idiopathic esophageal motility disorder, characterized by incomplete Lower Esophageal Sphincter (LES) relaxation, loss of enteric neurons and lack of peristalsis of the oesophagus. It can be seen in all ages with an incidence of 0.5- 1 per 100.000 [1]. Patients with achalasia usually suffer from progressive dysphagia and regurgitation and rarely chest pain, weight loss and dyspnea [2]. A systematic investigation of the prevalence of respiratory symptoms and diseases in patients with achalasia [3] was performed and reported a relatively high prevalence of patients with cough, hoarseness, wheezing, dyspnea, sore throat, and episodes of pneumonia. Impaired esophageal emptying from achalasia may lead to episodes of micro and macro-aspiration, thereby causing symptoms or airway and pulmonary disease [4,5], in up to 40% of cases of achalasia, pulmonary disorders can occur, with diffuse aspiration bronchiolitis occurring rarely [6].
Our patient has been planned for a Per-Oral Endoscopic Myotomy (POEM) procedure and she is on oral nitrates as she awaits the procedure.
Teaching point: All that wheezes is not asthma. Our patient had inadequate response to inhaled bronchodilators. In patients with suspected asthma and poor response to treatment, be sure to look for asthma mimics. A chest X-ray and a pulmonary function test are important for baseline evaluation. It is also important to remember that achalasia may present without any significant symptoms, except for reflux. A holistic approach to patient symptoms is important to clinical medicine.
References
- Fisichella PM, Carter SR, Robles LY. Presentation, diagnosis and treatment of oesophegeal motility disorders. Dig Liver Dis. 2012; 44: 1-7.
- Patti MG, Herbella FA. Achalasia and other esophageal motility disorders. J Gastrointest Surg. 2011; 15: 703-7.
- Sinan H, Tatum RP, Soares RV, Martin AV, Pellegrini CA, et al. Dis Esophagus. 2010. doi:10.1111/ j.1442-2050.2010.01126.x.
- Franquet T, Gimenez A, Roson N, et al. Aspiration diseases: Findings, pitfalls, and differential diagnosis. Radiographics. 2000; 20(3): 673-85.
- McArthur MS. Pulmonary complications of benign esophageal disease. Am J Surg. 1986; 151(2): 296-9.
- Sinan H, Tatum RP, Soares RV, Martin AV, Pellegrini CV, et al. Prevalence of respiratory symptoms in patients with achalasia. Dis Esophagus. 2011; 24(2): 224-8.