
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 5
Giant cutaneous squamous cell carcinoma
Camila Félix1*; Franklin Cabrera2
1Resident in Dermatology at UTE University, Quito, Ecuador.
2Dermatologist, Carlos Andrade Marín Specialties Hospital, Quito, Ecuador.
*Corresponding Author : Camila Félix
Resident in Dermatology at UTE University, Quito,
Ecuador.
Email: cami_felix95@hotmail.com
Received : Jan 13, 2024
Accepted : Jan 29, 2024
Published : Feb 05, 2024
Archived : www.jcimcr.org
Copyright : © Félix C (2024).
Abstract
Cutaneous squamous cell carcinoma is the second most common type of skin cancer after basal cell carcinoma [1]. Of all non melanoma skin cancers, it accounts for 20% to 25% and its mortality is up 1.5 to 3.4% [2]. SCC is considered very high risk if it is a tumor ≥4 cm, in any location. In these cases, surgery remains the first-line and most effective treatment. However, radiation therapy or systemic therapy can be used in situations where surgery is not feasible or is contraindicated. We present the case of an 89 year of female with 6 month evolution of a 10x8 cm rapidly growing mass on the biparietal region of the scalp, with a skin biopsy that reported a well-differentiated invasive cutaneous squamous cell carcinoma, without perineural or lymphovascular invasion. CT study reported invasion of the external and internal table of the skull. Radiation therapy was chosen as the first line treatment.
Keywords: Giant; Cutaneous squamous cell carcinoma; Invasion.
Citation: Félix C, Cabrera F. Giant cutaneous squamous cell carcinoma. J Clin Images Med Case Rep. 2024; 5(2): 2837.
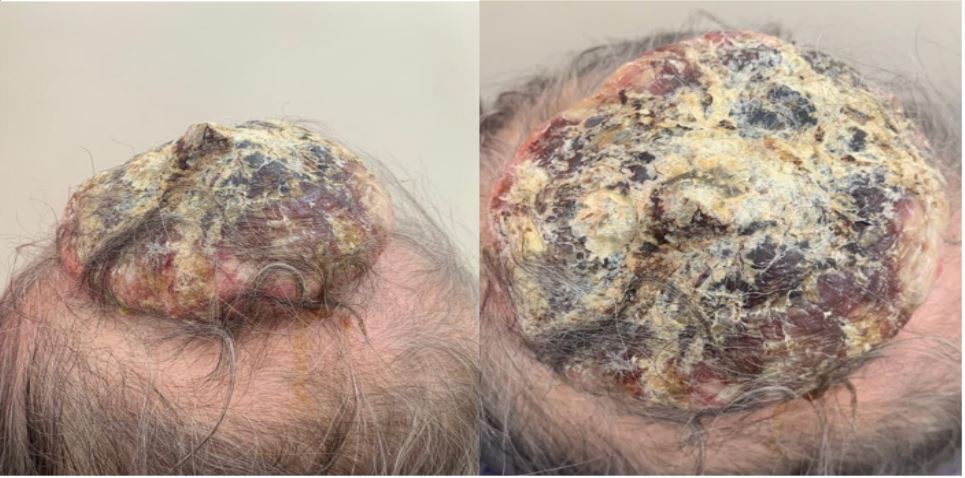
Description
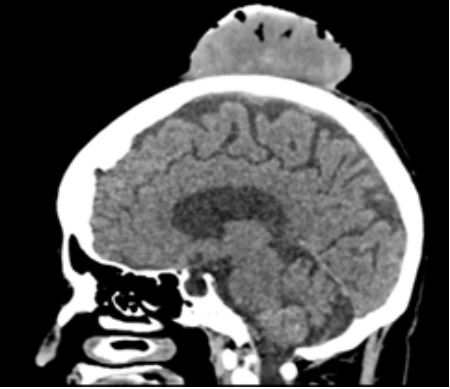
An 89-year-old female, with past medical history of diabetes mellitus, congestive heart failure, hyperparathyroidism and glaucoma, presented to the Dermatology department with 6 month evolution of a rapidly growing mass on the biparietal region of the scalp. The mass was a 10x8 cm, painful and friable tumor, with central necrosis and hyperkeratosis, over an erythematous area (Figures 1 and 2). There were no palpable lymph nodes. She had history of ultraviolet exposure due to previous jobs without family history of cancer. The patient reported that 3 years ago presented on the same region an erythematous and scaly, 1.5 cm plaque, with irregular, poorly defined edges; for which, an incisional biopsy was performed, reporting actinic keratosis and then treated with 5-Fluoracil for a month, after which the lesion disappeared. A new biopsy of the tumor was obtained and reported a well-differentiated invasive cutaneous squamous cell carcinoma, without perineural or lymphovascular invasion. Computed tomography reported a heterogeneous mass with air bubbles inside (Figure 3) that provokes lithic destruction of the skull compromising the internal and external table. The TNM stage was T4N0M0, stage IV, using the American Joint Committee on Cancer (AJCC). Due to other comorbidities and tumor extension, radiation therapy was chosen as the first line therapy.
Cutaneous squamous cell carcinoma is the second most common type of skin cancer after basal cell carcinoma [1]. Of all non melanoma skin cancers, it accounts for 20% to 25% and its mortality is up 1.5 to 3.4% [2]. SCC is considered very high risk if it is a tumor ≥4 cm, in any location. In these cases, surgery remains the first-line and most effective treatment. However, radiation therapy or systemic therapy can be used in situations where surgery is not feasible or is contraindicated [3]. Treatments such as topical therapies, photodynamic therapy, cryosurgery, curettage, and electrosurgery are not recommended in high-risk cases [4]. Lymph node metastases can develop in 1.9 to 5.2% of cases and patients with local or distant metastases tend to have much poorer outcomes [1]. In case of recurrence, it occurs most commonly within 2 years after the diagnosis, which is why its necessary a close clinical surveillance on the basis of the risks for local recurrence and metastasis [1].
References
- Wysong A. Squamous-cell carcinoma of the skin. N Engl J Med. 2023; 388(24): 2262-2273.
- Martorell-Calatayud A, Sanmartín Jimenez O, Cruz Mojarrieta J, & Guillén Barona C. Cutaneous squamous cell carcinoma: Defining the high-risk variant. Actas Dermosifiliogr. 2013; 104(5): 367-379.
- National Comprehensive Cancer Network. Squamous cell skin cancer, NCCN guidelines version. 2024. 2023 https://www.nccn. org/professionals/physician_gls/pdf/squamous.pdf.
- Uribe-Bojanini E, María Á, García L, Calfat GJ, Álvaro Sanabria Quiroga E, Mejía Montoya ME, & Cutánea, M Med Cutan Iber Lat Am. 2017; 45(1): 8-13.