
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Primary catastrophic antiphospholipid syndrome in children with midbrain infarction: A case report
*Corresponding Author : Qinghua Dong
National Laboratory of Macromolecules, Institute
of Biophysics, Chinese Academy of Sciences, Beijing,
China.
Email: 1668020893@qq.com
Received : Jan 13, 2024
Accepted : Jan 29, 2024
Published : Feb 05, 2024
Archived : www.jcimcr.org
Copyright : © Dong Q (2024).
Abstract
Background: Catastrophic Antiphospholipid Syndrome (CAPS) is a multi-system autoimmune disease characterized by extensive thrombosis. Pediatric CAPS is extremely rare and associated with a high mortality rate, especially when midbrain infarction is involved. Hence, early diagnosis and prompt initiation of appropriate treatment for CAPS complicated by midbrain infarction are of utmost importance in achieving favorable outcomes.
Case presentation: In this report, we present the case of a 14-yearold girl with primary CAPS who was admitted to our hospital with abdominal pain, altered consciousness, and chorea-like movements as primary symptoms. In subsequent examinations, we observed evidence of midbrain infarction and choreiform movements combined with hemolytic anemia, pulmonary embolism, microthrombus formation in the palms and soles, acute gastritis, and acute pancreatitis—all of which were consistent with the diagnosis of CAPS. The patient was treated in the intensive care unit with anticoagulation therapy, steroid shock, and multiple plasma infusions for 27 days before discharge, followed by regular follow-up.
Conclusion: This case report provides a description of the clinical features observed in a pediatric patient with CAPS and concurrent midbrain infarction, highlighting the crucial role of early diagnosis and timely treatment in influencing patient prognosis.
Keywords: Catastrophic antiphospholipid syndrome; Brain stem infarction; Pediatric; Thrombosis.
Abbreviations: APS: Antiphospholipid Syndrome; CAPS: Catastrophic Antiphospholipid Syndrome; CT: Computed Tomography; MRI: Magnetic Resonance Imaging; PICU: Pediatric Intensive Care Unit; SLE: Systemic Lupus Erythematosus.
Citation: Dong Q. Primary catastrophic antiphospholipid syndrome in children with midbrain infarction: A case report. J Clin Images Med Case Rep. 2024; 5(2): 2838.
Background
Catastrophic Antiphospholipid Syndrome (CAPS) is a severe form of Antiphospholipid Syndrome (APS) characterized by the occurrence of multiple thrombotic events within a short period of time, accompanied by elevated titers of antiphospholipid antibodies (aPL)—including persistently positive lupus anticoagulant, anti-β2-glycoprotein, and anti-cardiolipin antibodies often leading to multi-organ failure and life-threatening conditions. While CAPS is well documented in adults, it is extremely rare in children; however, it is known to be associated with a high mortality rate (33%-50%) [1]. Previous studies have shown minimal differences in clinical and laboratory characteristics, treatment, and outcomes between pediatric and adult patients with CAPS. The primary difference between the two is that pediatric populations have a higher proportion of infections as triggering factors than adults [2]. It is worth noting that, although the proportion of primary diseases in pediatric APS is low, the opposite is often observed in CAPS (38%-50% vs. 70%), with nearly 90% of pediatric APS cases presenting as CAPS at the time of disease onset [2,3].
The general diagnostic criteria for CAPS require the presence of persistent antiphospholipid antibodies (aPL), suchas anti-cardiolipin antibodies, anti-β2-glycoprotein I antibodies (β2GPIA), and/or Lupus Anticoagulant (LA), detected for at least 12 weeks. Evidence of the involvement of at least three organs, organ systems, and/or tissues, with these injuries occurring within 1 week is also needed. In the pediatric population, apart from being vigilant for thrombus formation in various organs or tissues, it is important to consider the differential diagnosis of non-criteria manifestations, as many pediatric cases of CAPS present with non-thrombotic manifestations. With central nervous system involvement frequently manifesting as chorea, epilepsy, migraine, pseudotumor cerebri, mood disorder, cognitive disorder, and transverse myelitis. Skin involvement frequently manifests as livedo reticularis, Raynaud phenomenon, skin ulcers, and purpura fulminans. Finally, blood system involvement frequently manifests as thrombocytopenia, autoimmune hemolytic anemia, Evans syndrome, leukopenia, or bleeding disorders [1,4,5]. The treatment for pediatric CAPS currently follows the guidelines published in the literature for adults with CAPS and generally involves a multimodal therapy regimen comprising anticoagulants, intravenous corticosteroids, plasma exchange, and/or intravenous immunoglobulins. However, some researchers have suggested that only Anticoagulation (AC) has a significant impact on the disease prognosis in these patients. Additionally, rituximab and eculizumab may be administered in refractory cases [6]. Despite standardized treatment, the mortality rate associated with this disease remains high (up to 30%) [5]. In the Pediatric Intensive Care Unit (PICU) setting, the rarity and high mortality rate, combined with non-thrombotic manifestations in pediatric patients, can lead to misdiagnosis of the disease and missed detection of thrombosis in critical areas, which can be fatal for the patients. Through this case report, we aim to raise awareness among clinicians about the possibility of brainstem infarction in CAPS children, especially when atypical symptoms resembling chorea are present.
Case presentation
A 14-year-old girl presented to the pediatric emergency department with abdominal pain and altered mental status. According to her mother, the patient had experienced abdominal pain for 2 weeks prior to admission. After 5 days of antibiotic treatment, her symptoms did not improve and altered consciousness developed. Upon admission, the patient had a Glasgow Coma Scale score of 8, with response to stimuli but without verbal response and withdrawal response to painful stimuli. Physical examination revealed dysarthria, gait and limb ataxia, as well as choreiform movements in the face and limbs. The patient had been hospitalized 5 years prior for thrombocytopenia but had no history of autoimmune diseases, cerebrovascular events, or seizures.
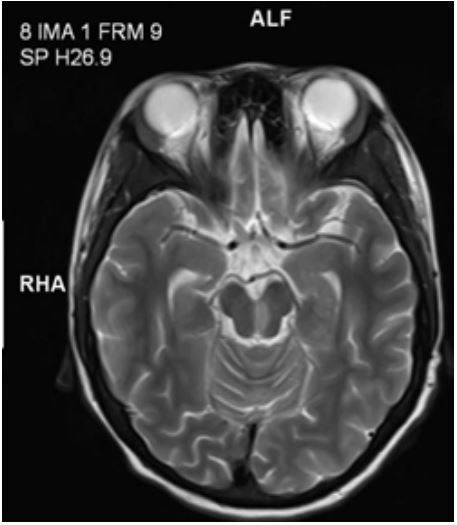
Further imaging and laboratory evaluations were performed after the patient was admitted to the PICU. Laboratory analysis indicated anemia, characterized by a hemoglobin level of 6.7 g/dL. Head magnetic resonance imaging (MRI) (Figure 1) revealed evidence of a left-sided infarct in the midbrain, while chest Computed Tomography (CT) revealed a bilateral pulmonary embolism in the basal regions of the lungs. Microthrombus formation was also observed in the patient’s palms and feet (Figure 2). Furthermore, the formation of reticular erythema was observed on the limbs. Vascular ultrasound of the extremities failed to reveal any obvious thrombus formation. Rheumatological laboratory tests showed elevated levels of antiphospholipid antibodies, including anticardiolipin antibodies, anti-β2-glycoprotein antibodies, and lupus anticoagulant (Table 1). Gastroscopy revealed erosive gastritis with gastroesophageal reflux and erosive esophagitis. Biochemical blood tests revealed increased serum amylase and lipase levels, suggesting possible acute pancreatitis. All these findings were consistent with the diagnosis of CAPS. The patient received 27 days of treatment in the PICU, with interdisciplinary discussions. Despite the presence of thrombocytopenia, systemic anticoagulation with heparin and corticosteroid therapy was administered owing to the association between CAPS, persistent thrombosis, and high mortality rates. Following a detailed evaluation of the patient’s condition and a multidisciplinary discussion, we considered multiple plasma transfusions as an alternative to plasma exchange, and achieved favorable treatment outcomes via this approach. Ultimately, the patient’s condition improved, and she was discharged after the recovery of consciousness.

Discussion
CAPS is an exceptionally rare yet profoundly deleterious disease among the pediatric population. This condition is characterized by the combined impairment of multiple organ functions, distinguishing it from APS. However, owing to its rarity, there is a paucity of literature on CAPS in pediatric patients. Only one recent case report described ischemic stroke as a coincidental clinical presentation of pediatric CAPS, but specifically presented CAPS as a secondary manifestation in the setting of systemic lupus erythematosus (SLE) [7]. Compared to the case in that report, our patient had a smaller infarction area and a better prognosis.
In our patient’s case, although CAPS was diagnosed promptly during the emergency department visit, the possibility of midbrain infarction was not initially considered. This could be attributed to the low incidence rate of this condition, and the patient’s chorea-like movements shortly after admission led us to initially attribute the neurological symptoms to atypical APS manifestations. Fortunately, the midbrain infarction in the patient was relatively localized, and upon reviewing the literature, we found that nearly 90% of pediatric APS cases present as CAPS. Although confirmation of the patient’s CAPS was only made after obtaining results of head MRI and chest CT, treatment for CAPS was initiated early on, which may have contributed to a better prognosis for our patient.
An analysis of 45 children with catastrophic APS from the CAPS Registry revealed that cerebral involvement was present in 22 cases (47.8%) [2]. This involvement included manifestations such as encephalopathy, cerebrovascular accidents, and seizures. In our patient, the manifestations of cerebral involvement were choreiform movement and cerebrovascular lesions of midbrain infarction. Although choreiform movement can be seen in cases without significant thrombotic events, midbrain infarction often leads to a series of manifestations such as extrapyramidal dysfunction, loss of consciousness, and incontinence. Therefore, we tend to attribute the patient’s choreiform symptoms to extrapyramidal dysfunction caused by midbrain infarction. Overall, we believe that central nervous system pathology cannot be separated from CAPS—and that, when corresponding neuropsychiatric symptoms and cerebral involvement are found, it is necessary to closely monitor patients due to the possibility of corresponding functional brain thrombotic events.
This case patient has provided a valuable insight into the potential close relationship between non-classical manifestations and thrombus formation in pediatric CAPS, which is of utmost importance in guiding clinical diagnosis and treatment. Typically, in pediatric cases of APS, non-thrombotic clinical manifestations (such as thrombocytopenia) and neurological disorders (such as migraine, epilepsy, and chorea) may precede thrombotic manifestations [8]. Even without clear evidence of brain thrombotic formation, choreiform movement has been identified as a characteristic manifestation of pediatric APS [9]. However, our reported case presents opposite findings, as the presence of chronic midbrain infarction on MRI suggests thrombus formation prior to the occurrence of neurological manifestations and may likely be the underlying cause of these neurological conditions. Therefore, it is crucial to emphasize considering the possibility of midbrain infarction in CAPS children who present with altered consciousness and chorea-like movements, rather than merely classifying them as atypical CAPS manifestations.
Triple therapy with anticoagulation, corticosteroids, and plasma exchange or intravenous immunoglobulin administration has been proposed as an optimal treatment strategy for CAPS [10]. Although plasma exchange is an established treatment option and a standard procedure in CAPS, we were unable to evaluate whether the pre-bypass process of priming the circuit would cause further harm to children owing to their low blood volume, hypotension, and the presence of anemia. Additionally, clinical evidence supporting the application of plasma exchange therapy in pediatric patients with CAPS is lacking. Therefore, after a detailed assessment of the patient’s condition, we empirically administered multiple plasma infusions as an alternative to plasma exchange, considering that multiple plasma infusions reduce the amount of plasma used and clinical risks associated with plasma exchange. This approach may serve as a reference for the treatment of children with a low blood volume.
Conclusion
While CAPS is exceedingly rare in the pediatric population, this case suggests that PICU physicians must be aware of its existence during the diagnostic and treatment processes, as misdiagnosis or delayed diagnosis poses significant risks to the patient’s life. Furthermore, we advocate for more standardized diagnostic and treatment protocols for pediatric CAPS to facilitate earlier recognition and uniform management in clinical practice. Finally, we emphasize considering the possibility of midbrain infarction in CAPS children who present with altered consciousness and chorea-like movements, rather than merely classifying them as atypical CAPS manifestations.
Educational objective: The study describes an extremely rare case of midbrain infarction in pediatric CAPS, along with its clinical manifestations. Clinicians should consider the possibility of midbrain infarction when encountering CAPS patients with altered consciousness and choreiform movements, rather than dismissing them as atypical presentations of CAPS. Multiple plasma transfusions and plasma exchange can be considered as alternative treatment options for certain pediatric CAPS cases.
References
- Go E, O’Neil K M. The catastrophic antiphospholipid syndrome in children [J]. Curr Opin Rheumatol. 2017; 29(5): 516-522.
- Berman H, Rodriguez-Pinto I, Cervera R, et al. Pediatric catastrophic antiphospholipid syndrome: descriptive analysis of 45 patients from the “CAPS Registry” [J]. Autoimmun Rev. 2014; 13(2): 157-162.
- Wincup C, Ioannou Y. The Differences Between Childhood and adult onset antiphospholipid syndrome [J]. Front Pediatr. 2018; 6: 362.
- Cervera R, Rodriguez-Pinto I, Espinosa G. The diagnosis and clinical management of the catastrophic antiphospholipid syndrome: A comprehensive review[J]. J Autoimmun. 2018; 92: 1-11.
- Islabao A G, Trindade V C, Da M L, et al. Managing Antiphospholipid Syndrome in Children and Adolescents: Current and Future Prospects [J]. Paediatr Drugs. 2022; 24(1): 13-27.
- Kazzaz NM, McCune WJ, Knight JS. Treatment of catastrophic antiphospholipid syndrome [J]. Curr Opin Rheumatol. 2016; 28(3): 218-227.
- Senken B, Whitehead A. Catastrophic Antiphospholipid Syndrome Presenting as a Stroke in an 11-Year-Old with Lupus [J]. Case Rep Pediatr. 2022; 2022: 7890566.
- Soybilgic A, Avcin T. Pediatric APS: State of the Art [J]. Curr Rheumatol Rep. 2020; 22(3): 9.
- Avcin T, Cimaz R, Silverman E D, et al. Pediatric antiphospholipid syndrome: clinical and immunologic features of 121 patients in an international registry [J]. Pediatrics. 2008; 122(5): 1100-e1107.
- Rodríguez-Pintó I, Lozano M, Cid J, Espinosa G, Cervera R. Plasma exchange in catastrophic antiphospholipid syndrome. Presse Med. 2019; 48(11-2): 347-353.