
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Submucosal retropharyngeal dissection during nasotracheal intubation: A case report
Leekyeong Kang; Kyungsoo Ha; Seungcheol Yu; Tae Yeon Kim; Mi Ae Jeong*
Department of Anesthesiology and Pain Medicine, Hanyang University Hospital, Seoul, Korea.
*Corresponding Author : Mi Ae Jeong
Department of Anesthesiology and Pain Medicine,
Hanyang University Hospital, Seoul, Korea.
Tel: 82-2-2290-8680, Fax: 82-2-2299-0742;
Email: macheong@hanyang.ac.kr
Received : Jan 11, 2024
Accepted : Jan 30, 2024
Published : Feb 06, 2024
Archived : www.jcimcr.org
Copyright : © Jeong MA (2024).
Abstract
Introduction: Nasotracheal intubation is a common procedure in the operating room, but it carries the risk of various complications, ranging from benign conditions to more serious complications such as retropharyngeal dissection. Here, we present a case of retropharyngeal dissection together with a brief review of the related literature.
Case report: A 52-year-old man with oral cavity cancer was admitted for maxillectomy and free-flap reconstruction. Nasotracheal intubation was attempted twice, but the nasotracheal tube tip created a bulging contour that was detected in the right submandibular region, indicating retropharyngeal dissection. After successful fiberoptic intubation, the surgeon detected retropharyngeal dissection and repaired it. The patient was transferred to the intensive care unit after surgery and there were no delayed complications.
Conclusion: When retropharyngeal dissection occurs, prompt diagnosis and management are crucial. As indicated in the literature, it is also important to make every effort to perform nasotracheal intubation carefully to prevent complications.
Keywords: Endotracheal intubation; General anesthesia; Latrogenic diseases; Intraoperative complications; Otorhinolaryngologic surgical procedures; Retropharyngeal dissection.
Citation: Kang L, Ha K, Yu S, Kim TY, Jeong MA. Submucosal retropharyngeal dissection during nasotracheal intubation: A case report. J Clin Images Med Case Rep. 2024; 5(2): 2842.
Introduction
Nasotracheal intubation is an airway management method commonly used in operating rooms and is known to have several advantages than orotracheal intubation. Nasotracheal intubation is an alternative in situations where orotrachaeal intubation cannot be implemented such as head and neck surgery (including oropharyngeal, microlaryngeal, and dental surgery), and can also be used as during awake fiberoptic procedures in patients with cervical spine instability, structural abnormalities of orotracheal airway, or obstructive lesions in the oral cavity [1].
Despite the advantages of nasotracheal intubation, a variety of complications can arise due to the inability to directly observe the tube’s passage through the nasotracheal cavity. Reported complications range from common and mostly benign conditions such as epistaxis and nasotracheal mucosal injury to rare and serious conditions, such as turbinectomy and retropharyngeal dissection [1,2]. Retropharyngeal dissection is of the greatest concern, as it can lead to cervical vascular injury, cervicofacial and mediastinal emphysema, and even deep neck infection [3]. Here, we present a rare case of retropharyngeal dissection during nasotracheal intubation for maxillectomy, along with a brief review of the literature.
Case report
Written informed consent was obtained for publication of this case report. A 52-year-old male patient, weighing 76 kg and 173 cm in height, with left upper alveolus cancer was scheduled for left inferior maxillectomy, selective dissection of the left neck level II and III lymph nodes, and reconstruction of surgical defect with anterolateral thigh free flap. The patient was a hepatitis C virus carrier and had underlying hypertension, resulting in their being considered Class 2 according the American Society of Anesthesiology (ASA) physical status classification system. The initial airway management plan for surgery was to perform nasotracheal intubation through the right nostril, followed by conversion to tracheostomy mid-procedure. Airway examination indicated the airway was consistent with a Mallampatti Class II score. The physical examination (neck extension and flexion), preoperative computed tomography (CT) and fiberoptic laryngoscopy showed no remarkable abnormalities in the airway.
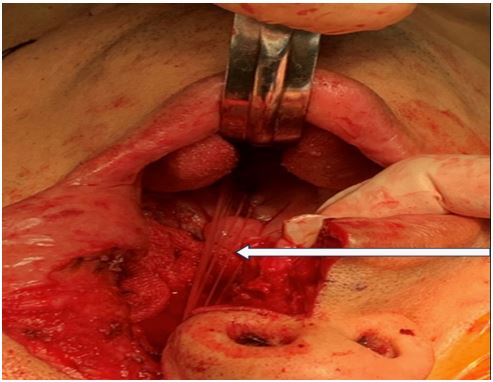
Before inducing general anesthesia, the otolaryngologist packed the patient’s right nostril with epinephrine (Bosmin, Jeil Pharmaceutical Co., Seoul, Korea) gauze. A 7.0-mm right-angle endotracheal tube (ShileyTM Nasotracheal RAE endotracheal tube with TaperGuardTM cuff, Medtronic, Fridley, MN, USA) was lubricated and prepared for subsequent intubation. Then, general anesthesia was induced under standard ASA monitoring using a continuous intravenous infusion of remifentanil followed by intravenous injection of 20 mg remimazolam and 50 mg rocuronium. Bag and mask ventilation was performed for two minutes. Then, after visualizing the vocal cords (considered Cormack-Lehane Grade I) using a video laryngoscope (McgrathTM MAC Video Laryngoscope, Medtronic, Fridley, MN, USA), the epinephrine gauze was removed and the lubricated tube was gently inserted along the bottom of the nasotracheal cavity by pushing it down in a postero-inferior direction through right nostril. However, even after advancing to a sufficient depth, the tip of the tube could not be detected on video laryngoscopy, so the tube was removed immediately. Bag and mask ventilation was performed for an additional minute before re-intubation. Assuming that an inadequate sniffing position was the cause of failure, the neck was extended to a greater degree. During the second attempt, the tip of the tube was still not visible, and a bulging contour at right submandibular area was noticed at this time. False passage of the nasotracheal tube and subsequent retropharyngeal dissection was suspected (Figure 1A, 1B), so the tube was immediately removed followed by an additional two minutes of bag and mask ventilation. Since repeated intubation through the same nostril may aggravate the dissection and bleeding, and because access to the opposite nostril was impossible due to the surgical plan, immediate oral intubation using a video laryngoscope was performed for patient safety. After successful oral intubation, blood within oral cavity and oropharynx was removed by suction, and a fiberoptic endoscope with a nasotracheal endotracheal tube was inserted through the right nostril. After navigation of the fiberoptic tip to the vocal cords, the oral endotracheal tube was removed and the nasotracheal tube was successfully inserted under fiberoptic guidance. To prevent airway edema, 10 mg of dexamethasone was injected intravenously. Suspected pharyngeal dissection was reported to the surgeon, and sufficient oral povidone disinfection was performed to prevent deep neck infection. The otolaryngologist discovered a submucosal laceration from the nasopharynx to the hypopharynx resulting from the initial nasotracheal intubation attempts, but there were no notable collateral injuries to adjacent blood vessels or other vital structures. Since there was no evidence of active bleeding, the surgery proceeded as originally planned. After successful conversion to tracheostomy during surgery, the iatrogenic laceration was sutured (Figure 2) and surgery continued. The patient underwent an uneventful wide excision and free-flap reconstruction of the left upper alveolar lesion. No delayed hematoma or other complications associated with the retropharyngeal dissection occurred during or immediately after surgery. After the surgery, 160 mg sugammadex was injected intravenously to restore the patient’s spontaneous respiration. The patient was transferred to the Intensive Care Unit (ICU) with 9 L of 35% O2 administered through the t-piece. All vital signs and respiration were stable at the time of transfer.
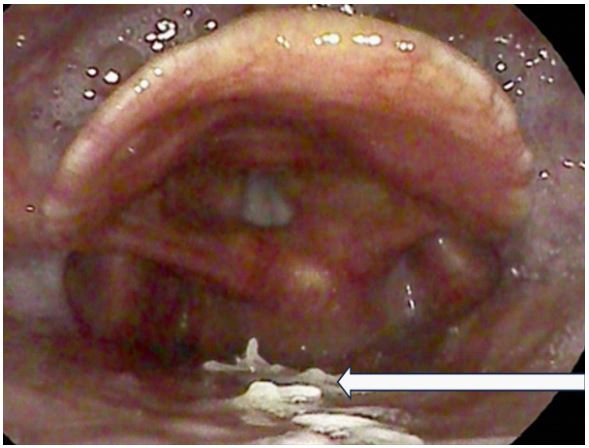
Antibiotic treatment was initiated with injection of 1.5 g ampicillin/sulbactam TID and flomoxef 500 mg QID intravenously for two weeks. Thereafter, 100 mg cefdinir QID was administered orally for one week. Contrast-enhanced neck CT was performed on the seventh postoperative day, and no delayed complications, such as subcutaneous emphysema, retropharyngeal hematoma, deep neck infection, or injury of adjacent vital structures (e.g., carotid artery, internal jugular vein, etc.), were detected. Moreover, follow-up fiberoptic endoscopic examinations were clear without indications of suture dehiscence or other complications (Figure 3). The patient was discharged without remarkable complications.
Table 1: Literature review of retropharyngeal dissection during nasotracheal intubation.
| References | Age/sex | Intra-operative findings | Resistance | Special notes |
|---|---|---|---|---|
|
Landess WW et al. (1994) |
90/F |
Bulging of posterior pha- ryngeal wall. |
+ | |
|
Pena MT et al. (2004) |
6/F |
Failure of positive pres- sure ventilation. |
+ | |
|
Ghaffari S et al. (2006) |
7/F |
Tube piercing pharyngeal mucosa and re-entering oropharynx. |
+ | |
|
Bozdogan N et al. (2008) |
67/M |
Tube piercing pharyngeal mucosa and re-entering oropharynx. |
N/D | |
|
Krebs MJ et al. (2008) |
54/F |
Bulging of posterior pha- ryngeal wall. |
- | |
|
Ersoy B et al. (2011) |
25/M |
Subcutaneous bulging below the right angle of mandible. |
- | |
|
Kamatani T et al. (2013) |
58/F |
Audible crepitus in neck region. |
+ | RPE* |
|
Hakim M et al. (2015) |
4/F |
Oropharyngeal hema- toma. Bulging of posterior pha- ryngeal wall. |
Minimal | |
| 6/M |
Bulging of posterior pha- ryngeal wall. |
+ | Use of CTT |
|
|
Devarakonda BV et al. (2019) |
22/M |
Oropharyngeal hema- toma. Swelling of posterior pharyngeal wall. |
N/D | |
|
Okamoto A et al. (2023) |
81/F |
Subcutaneous bulging of right submandibular region. |
N/D |
Use of CTT, Injury near RCCA* |
*Confirmed by postoperative computed tomography CTT: Curved-Tip Tube; N/D: Not Described; RCCA: Right Common Carotid Artery; RPE: Retropharyngeal Emphysema
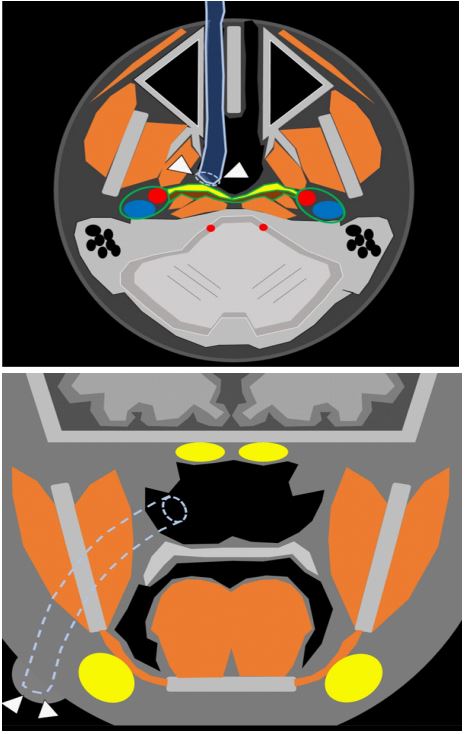
A. Schematic axial image at the patient’s nostril level. Note that the endotracheal tube falsely enters into the submucosal layer (arrowheads) of the posterior wall of nasopharynx. Adjacent structures included the retropharyngeal space (yellow colored space), adjacent muscle spaces (dark brown-colored space), internal carotid artery (red) and internal jugular vein (blue). LP: lateral pterygoid muscle; Max S: maxillary sinus; MP: medial pterygoid muscle; Mss: masseter muscle.
B. Schematic coronal image of the patient shows the nasotracheal tube inserted through a false passage. Note the tube tip within the right submandibular space, creating a bulging contour (arrowheads). MH: mylohyoid muscle; MP: medial pterygoid muscle; Mss: masseter muscle; Pal: palate; SLG: sublingual gland; SMG: submandibular gland.
Discussion
The authors unexpectedly identified retropharyngeal dissection during nasotracheal intubation of a patient without any pathological or anatomical abnormalities of the airway, and the dissection was sutured during surgery. We report this case along with a literature review to once again emphasize the prevention, diagnosis, and treatment of retropharyngeal dissection.
Nasotracheal intubation is often requested in order to improve the visibility and accessibility of the surgical field for head and neck surgery; however, nasotracheal intubation has a higher failure rate and greater risk of complications than conventional orotracheal intubation. Epistaxis is the most frequent complication. Although other complications of varying severity have also been reported, such as sinusitis, bacteremia, iatrogenic turbinectomy, and even intracranial tube placement [1].
Retropharyngeal dissection is another possible but rare complication, occurring in approximately 2% of cases [4,5]. Serious sequelae of retropharyngeal dissection include airway obstruction due to hematoma in the retropharyngeal space, cervicofacial or mediastinal emphysema [3], and carotid artery injury followed by dissection or thrombosis [6].
A unique feature of our case is that the dissection was easily revealed and repaired during a planned maxillectomy due to the common surgical field and the availability of an otolaryngologist. Because access to the retropharyngeal space is generally difficult, in the absence of severe bleeding, surgery is continued in most cases without first making a definitive diagnosis or treating the dissection [2,3,6]; postoperative imaging studies, such as plain radiograph or CT, are generally used to monitor possible delayed complications.
In the case presented here, the anesthesiologists correctly suspected a retropharyngeal dissection during the second intubation attempt, but were unable to diagnose dissection with confidence or evaluate the exact extent of the injury even with the aid of subsequent fiberoptic examination. Nonetheless, the surgeon diagnosed and repaired dissection easily during the surgery. Thus, it is important to consult an otolaryngologist without hesitation once the complication is suspected.
We reviewed the available literature and case reports regarding retropharyngeal dissection during nasotracheal intubation. As a result of searching keywords such as “retropharyngeal dissection”, “retropharyngeal injury”, and “retropharyngeal perforation” using PubMed, 11 articles related to nasotracheal intubation was identified among a total of 980 results, after exclusion of duplicate or irrelevant results. Brief summaries of each patient’s demographic data and characteristics as reported in these articles are presented in Table 1 [2,3,6-9].
According to the literature, risk factors for retropharyngeal dissection include resistance during nasotracheal intubation, multiple intubation attempts, overinflation of the cuff, tube malposition, use of a stylet, and inappropriate tube size [1,10]. The following are recommended measures to prevent retropharyngeal dissection and other complications during nasotracheal intubation: [1] before surgery, the anatomical structure of the nasotracheal cavity and nasopharynx should be assessed to select the appropriate nostril for intubation; [2] a tube of the appropriate size and type must be selected; [3] topical vasoconstrictors such as low-concentration epinephrine or phenylephrine should be applied before intubation; [4] warming the tube with warm saline solution to soften it prior to placement may reduce damage to the nose [11]; and [5] once resistance is felt, insertion should be stopped immediately [1,12]. With regard to the type of nasotracheal tube, there are several options to consider: silicone-based tubes are associated with fewer complications and less postoperative pain than PVC-based tubes [13], and a Magill tube, which has a shorter and more blunt tip than a Murphy tube, may also reduce nasotracheal trauma [14]; and use of a specialized tube with a curved tip (e.g., the Parker FlexTip™ tracheal tube, Parker Medical, Highlands Ranch, CO, USA) may also be helpful [7]. A few other measures, such as finger cot, nasogastric tube, urinary catheter, or gum elastic bougieassisted intubation may also reduce nasotracheal trauma [2,15].
Once retropharyngeal dissection is suspected, an alternative airway should be secured immediately and an otolaryngologist should be consulted. A fiberoptic examination should be performed to exclude severe complications, such massive hematoma or damage to vital structures [2]. Care should be taken to not cause additional collateral damage when removing the endotracheal tube. Positive-pressure ventilation through an incorrectly placed tube is absolutely contraindicated, as it can cause severe pneumomediastinum or pneumothorax [3].
Additionally, late postoperative hematomas may cause delayed airway obstruction or subcutaneous emphysema, necessitating chest X-ray or postoperative CT follow-up and observation in the ICU.
In this case, several routine pre-operative precautions were taken, such as careful investigation of preoperative CT anatomy, selection of appropriately sized tubes, and application of topical vasoconstrictors; however, further measures, such as using a tube with a curved tip or softening of tube in warm saline, were not undertaken. The lack of significant resistance during the first two attempts caused additional confusion; regardless, the authors correctly suspected retropharyngeal dissection due to the appearance of a submandibular protrusion, and subsequent management was excellent.
Conclusion
In summary, retropharyngeal dissection is an unusual complication of nasotracheal intubation that can lead to serious consequences such as cervical vessel injury, subcutaneous emphysema, and airway obstruction [3,6]. Therefore, anesthesiologists must be aware of the recommended pre-operative assessments and procedures, and proceed with caution even if there no risk factors are identified. In addition, as noted in several other publications, when retropharyngeal dissection is suspected, it is critical to immediately evaluate the area and take appropriate measures to avoid serious consequences. After surgery, close monitoring of the patient’s condition and vital signs, and appropriate testing (e.g. plain radiographs, CT, and laboratory tests) must be performed.
References
- Park DH, Lee CA, Jeong CY, Yang H-S. Nasotracheal intubation for airway management during anesthesia. Anesthesia and Pain Medicine. 2021; 16: 232-47.
- Hakim M, Cartabuke RS, Krishna SG, Veneziano G, Syed A, Lind M, et al. Submucosal dissection of the retropharyngeal space during nasotracheal intubation. Middle East J Anaesthesiol. 2015; 23: 309-14.
- Kamatani T, Kohzuka Y, Kondo S, Shirota T, Iijima T, Shintani S. Retropharyngeal dissection: a case report of cervicofacial subcutaneous emphysema and mediastinal emphysema during attempted nasotracheal intubation. Journal of Anesthesia. 2013; 27: 785-6.
- Robert Pierre I, Dym H. Endotracheal tube obstruction via turbinectomy during nasotracheal intubation. Anesthesia Progress. 2018; 65: 255.
- Tintinalli JE, Claffey J. Complications of nasotracheal intubation. Annals of Emergency Medicine. 1981; 10: 142-4.
- Okamoto A, Kawaraguchi Y, Fujita M, Goto Y, Shimokawa M. Accidental retropharyngeal dissection extending close to the right common carotid artery during nasotracheal intubation: a case report. JA Clinical Reports. 2023; 9: 11.
- Terumitsu M, Hirahara M, Seo K. Retropharyngeal dissection by Parker Flex-Tip nasotracheal endotracheal tube. Anesthesia Progress. 2017; 64: 240-3.
- Ersoy B, Gürsoy T, Çelebiler Ö, Umuroglu T. A complication of nasotracheal intubation after mandibular subcondylar fracture. Journal of Craniofacial Surgery. 2011; 22: 1527-9.
- Devarakonda BV, Issar Y, Goyal R, Vadapalli K. ‘Where did the tube go?’ A case of retropharyngeal submucosal false passage during nasotracheal intubation. Medical Journal Armed Forces India. 2019; 75: 476-8.
- Krebs MJ, Sakai T. Retropharyngeal dissection during nasotracheal intubation: a rare complication and its management. Journal of Clinical Anesthesia. 2008; 20: 218-21.
- Kim YC, Lee SH, Noh GJ, Cho SY, Yeom JH, Shin WJ, et al. Thermosoftening treatment of the nasotracheal tube before intubation can reduce epistaxis and nasotracheal damage. Anesthesia & Analgesia 2000; 91: 698-701.
- Ghaffari S. Forceful insertion of nasotracheal tube may pierce the posterior nasopharyngeal mucosa. Pediatric Anesthesia. 2006; 16: 997-.
- Kihara S, Komatsuzaki T, Brimacombe JR, Yaguchi Y, Taguchi N, Watanabe S. A silicone-based wire-reinforced tracheal tube with a hemispherical bevel reduces nasotracheal morbidity for nasotracheal intubation. Anesthesia & Analgesia. 2003; 97: 1488-91.
- Lee J-H, Kim C-H, Bahk J-H, Park K-S. The influence of endotracheal tube tip design on nasotracheal trauma during nasotracheal intubation: magill-tip versus murphy-tip. Anesthesia & Analgesia. 2005; 101: 1226-9.
- Wong A, Subar P, Witherell H, Ovodov KJ. Reducing nasopharyngeal trauma: the urethral catheter–assisted nasotracheal intubation technique. Anesthesia Progress. 2011; 58: 26-30.