
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Aortic pseudoaneurysm – Something fishy!
Kavya S Kaushik; Rupa Ananthasivan*; Aamani Chinnappannagari; Sudarshan Rawat
Department of Radiology, Manipal Hospitals, Bengaluru, Karnataka, India.
*Corresponding Author : Rupa Ananthasivan
Department of Radiology, Manipal Hospitals, Bengaluru, Karnataka, India.
Tel: +91 9980156087;
Email: rupanth@yahoo.com
Received : Jan 15, 2024
Accepted : Jan 31, 2024
Published : Feb 07, 2024
Archived : www.jcimcr.org
Copyright : © Ananthasivan R (2024).
Abstract
Accidental ingestion of a fishbone, rarely, when impacted in the esophagus, can cause an unusual range of complications from esophageal perforation to rare catastrophic vascular injuries like aortic pseudoaneurysm and aortoesophageal fistula, necessitating management on an emergency basis with computed tomographic angiography to establish the diagnosis and facilitate timely management with broad spectrum antibiotics and TEVAR with or without combined thoracic surgery. Here, we present one such rare case.
Keywords: Aortic pseudoaneurysm; Aortoesophageal fistula; CT; 3D VR; TEVAR.
Citation: Kaushik KS, Ananthasivan R, Chinnappannagari A, Rawat S. Aortic pseudoaneurysm – Something fishy!. J Clin Images Med Case Rep. 2024; 5(2): 2844.
Case report
A 66-year-old male with small volume hematemesis, low Hemoglobin of 7.3 g/dL and stable vitals was referred for a CT thorax with IV contrast with clinical suspicion of a ruptured aortic aneurysm.
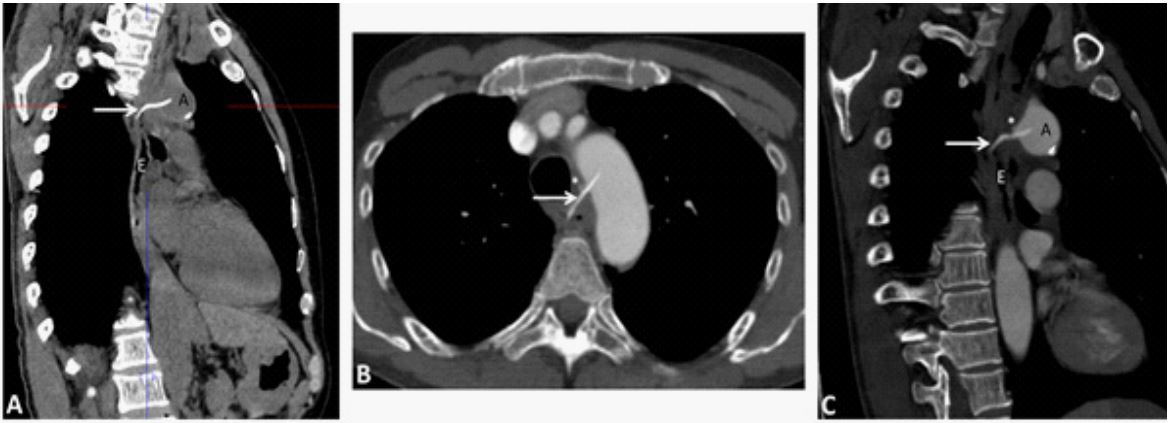
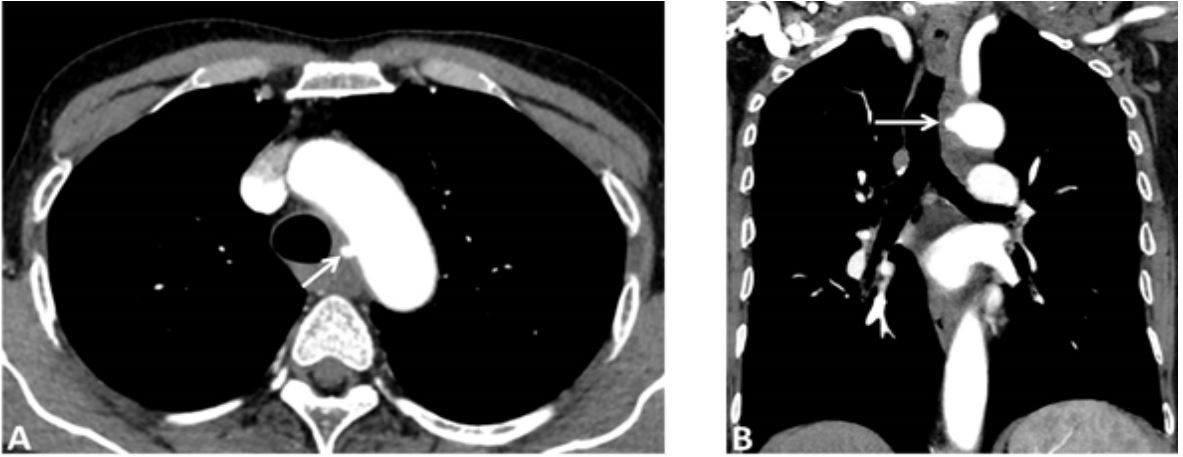
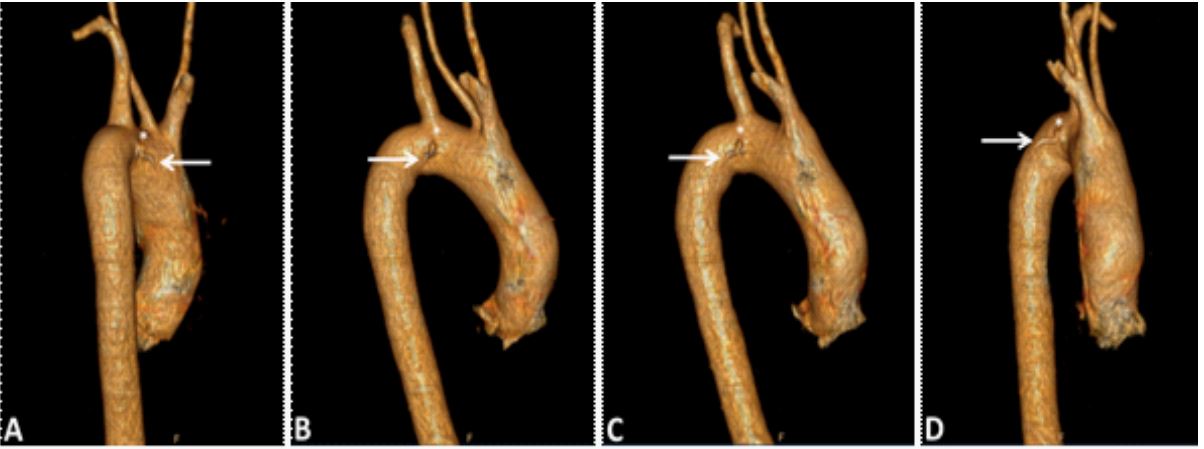
CT imaging showed an approximately 36 mm long thin, linear, high-density foreign body in the thoracic esophagus, above the level of the carina, at C4 vertebral level, piercing the lateral wall of the esophagus and penetrating the adjacent medial wall of the aortic isthmus, directed anterolaterally and superiorly, with 9 mm within the aorta (Figures 1 and 3). Resultant formation of a small 4 mm focal contrast filled outpouching from the aortic isthmus at the site of aortic penetration, suggestive of a pseudoaneurysm (Figure 2).
Surrounding mild fat stranding and few subcentimetric lymphnodes were seen. No abscess/free air/contrast extravasation into the mediastinum or esophagus/mediastinal hematoma/ pleural effusion was visualised. Lungs and rest of the mediastinal structures were normal. The patient recalled consuming fish for a meal about 12 days prior and denied any symptoms of chest discomfort, dysphagia or odynophagia.
The diagnosis of an impacted esophageal foreign body (fish bone) complicated by direct aortic penetration and aortic pseudoaneurysm was made. Possibility of an aorto-esophageal fistula was considered in view of clinical history of sentinel hematemesis. An upper GI endoscopic foreign body removal and stent-graft repair of the aortic pseudoaneurysm was planned. However, the patient declined any active intervention and opted for conservative management elsewhere. Patient was lost to further follow-up at our institution.
Discussion
Accidentally ingested fishbone, when impacted in the esophagus, can result in unusual complications, including esophageal perforation (1-4%) and catastrophic vascular injuries like aortic pseudoaneurysm and aortoesophageal fistula (0.1%), necessitating management on an emergency basis [1].
Impaction at the anatomical narrowing of the thoracic esophagus, the second most common site for foreign body impaction and perforation, is prone to cause vascular injury, most commonly from 1 to 5 cm distal to the left subclavian artery origin, due to its proximity to the aorta [2]. Aortic pseudoaneurysms develop from either direct puncture of the aortic wall by a foreign body, as in our case, or from the extension of mediastinal inflammation, which makes the aortic wall weak and friable. Aortoesophageal fistula, a direct communication between the oesophagus and the aorta, is initially concealed due to occlusion and tamponade of the perforation site by the clot, but rapidly progresses [3].
CT with oral and intravenous contrast is the modality of choice for assessment of foreign body esophageal perforation and its complications, with a sensitivity of 92 to 100% [3].
Rarity precludes standardized guidelines, and management options depend on the patient’s general condition, severity of the mediastinitis, recovery from the esophageal fistula and extent of aortic injury [4], with primary goals being control of hemorrhage and infection, repair of aortic and esophageal defects. Conventional treatment of open surgery with aortic neoplasty [1] is now superseded by thoracic endovascular aortic repair (TEVAR) as a rapid, effective, minimally invasive technique for control of exsanguination and as a bridge for definitive repair and in some cases even as the sole intervention [1,4]. Prompt broad-spectrum antibiotic treatment is essential to counter the inevitable mediastinitis [1]. Additional open or thoracoscopic mediastinal debridement may be necessary [4]. Repair of esophageal defect can be performed at a later stage by open surgery or via thoracoscopic esophageal stenting [5].
Conclusion
In conclusion, urgent computed tomographic angiography is essential to establish the diagnosis and facilitate timely management with broad-spectrum antibiotics and early intervention with TEVAR with or without additional thoracic surgery.
Declarations
Conflict of interest: The authors declare that they have no conflict of interest.
Funding: This study was not supported by any funding.
Ethical approval and consents: This report describes a rare diagnosis from routine diagnostic procedures. Hence, approval from the institutional review board was not obtained. Written informed consents for all the procedures were obtained before they were performed. For this type of study, consent for publication is not required as the data to be published is sufficiently anonymised.
References
- Chen AP, Yu H, Li HM, Xiao XS, & Liu SY. Aortoesophageal fistula and aortic pseudoaneurysm induced by swallowed fish bone: a report of two cases. Cardiovascular and interventional radiology, 2011; 34(2): 17-19. https://doi.org/10.1007/s00270-009- 9764-7.
- Bathla G, Teo LL, Dhanda S. Pictorial essay: Complications of a swallowed fish bone. Indian J Radiol Imaging. 2011; 21(1): 63- 8. doi: 10.4103/0971-3026.76061. PMID: 21431037; PMCID: PMC3056375.
- Zuluaga CP, Aluja Jaramillo F, Velásquez Castaño SA, Rivera Bernal AL, Granada JC, Carrillo Bayona JA. Aortic Pseudoaneurysm Secondary to Mediastinitis due to Esophageal Perforation. Case Rep Radiol. 2016; 2016: 7982641. doi: 10.1155/2016/7982641. Epub 2016 Feb 10. PMID: 26977330; PMCID: PMC4764720.
- Gong H, Wei W, Huang Z, Hu Y, Liu XL, & Hu Z. Endovascular stent-graft treatment for aortoesophageal fistula induced by an esophageal fishbone: Two cases report. World journal of clinical cases. 2022; 10(7): 2206-2215. https://doi.org/10.12998/wjcc. v10.i7.2206.
- Sia KJ, Ashok GD, Ahmad FM, & Kong CK. Aorto-oesophageal fistula and aortic pseudoaneurysm caused by a swallowed fish bone. Hong Kong medical journal. 2013; 19(6): 542-544. https:// doi.org/10.12809/hkmj133668.