
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 5
Diabetic myonecrosis with bilateral psoas inflammation
Sehreen Mumtaz1*; Andrés Felipe Cardona-Cardona2 ; Rupert Stanbourough3 ; Florentina Berianu2 ; Andy Abril2
1Division of Rheumatology, Mayo Clinic, Jacksonville, Florida, USA.
2Division of Rheumatology, University of Antioquia, Medellín, Colombia.
3Division of Radiology, Mayo Clinic, Jacksonville, Florida, USA.
*Corresponding Author : Sehreen Mumtaz
Division of Rheumatology, Mayo Clinic, Jacksonville,
Florida, USA.
Email: Mumtaz.Sehreen@mayo.edu
Received : Jan 13, 2024
Accepted : Jan 31, 2024
Published : Feb 07, 2024
Archived : www.jcimcr.org
Copyright : © Mumtaz S (2024).
Abstract
Citation: Mumtaz S, Cardona AFC, Stanbourough R, Berianu F, Abril A. Diabetic myonecrosis with bilateral psoas inflammation. J Clin Images Med Case Rep. 2024; 5(2): 2845.
Clinical image description
A 37-year-old male with a 30-year history of type 1 Diabetes Mellitus (DM) was hospitalized for acute onset of left lower extremity stiffness and significant myalgias limiting ambulation and standing up from a sitting position. There was no history of prior trauma and no prior skin rash, arthralgia, Raynaud’s phenomenon, or periungual capillary changes. He had been on insulin and HMG-CoA reductase inhibitor for 20 years. Physical examination was notable for pain with passive left hip movement. Strength and sensibility were normal, and there was no atrophy. Creatinine Kinase (CK) was elevated at 1800 U/L, the myositis panel and anti-HMG-CoA reductase antibody were negative. He received intravenous antibiotics for a possible inflammatory myopathy. A Computed Tomography (CT) scan revealed lowdensity regions in the bilateral psoas muscles (Figure 1A) and a CT-guided aspirate found no evidence of infection. Hence antibiotics were suspended, and a trial of corticosteroids was started for a possible inflammatory myopathy with a modest response. A lumbar spine MRI with contrast showed non-enhancing regions in both psoas muscles (Figure 1B) even though he did not have significant right-sided symptoms. Ultimately, bilateral diabetic psoas myonecrosis was diagnosed and was managed with supportive care, including strict glycemic control, with slowly progressive improvement.
Diabetic myonecrosis or diabetic muscle infarction is a rare microangiopathic complication associated with poorly controlled type 1 or type 2 DM [1,2]. MRI features hyperintense signal on T2-weighted images and an isointense to hypointense signal on T1-weighted images from the affected muscle [2]. Muscle biopsy can provide a definitive diagnosis but is currently not recommended due to the risk for an increase in time to symptomatic improvement [2]. The differential diagnosis of diabetic myonecrosis consists of polymyositis, diabetic lumbosacral radiculoplexopathy, and inflammatory myopathies [1]. Psoas muscle involvement in diabetic myonecrosis is not expected, and this unique clinical vignette reinforces the consideration for this differential when suspecting idiopathic inflammatory myopathy.
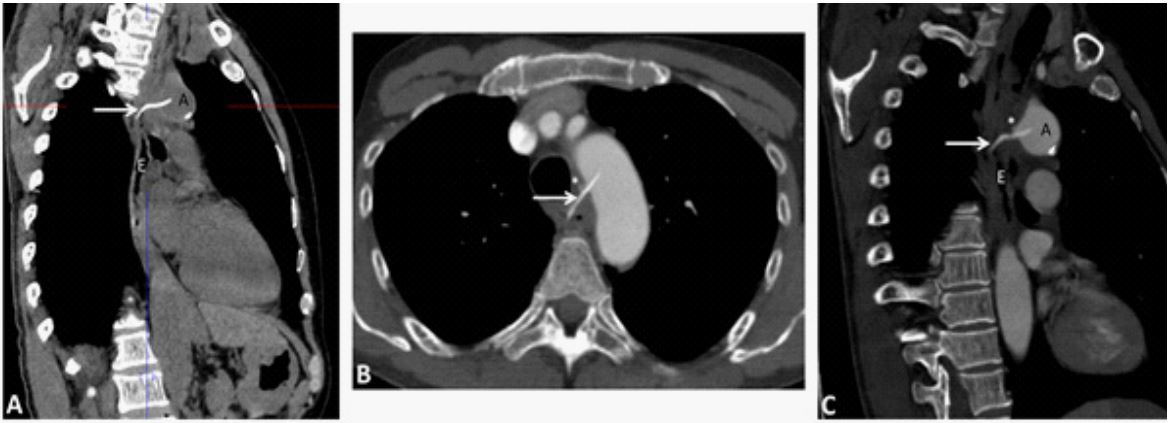
A. Axial CT image of the abdomen obtained post intravenous contrast. There are low-density regions in the peripheral aspects of the bilateral psoas muscles with ill-defined margins (red arrows). The psoas muscles appear.
hypertrophied and there were inflammatory changes in the adjacent fat (blue arrow heads). B. Axial T1-weighted fat-saturated MRI image of the lumbar spine obtained post intravenous contrast showed non-enhancing regions in both psoas muscles (red arrows) consistent with avascular necrotic material.
Declarations
Author contributions: All the authors were involved in the care of the patient, conception and design, drafting, editing, and approval of the final manuscript.
Availability of data and materials: Not applicable.
Consent: Written consent for publication was obtained from the patient.
Competing interests and funding: This research received no specific grant from any funding agency in the public or commercial sectors.
Conflict of interest: None declared.
References
- Bunch TJ, Birskovich LM, Eiken PW. Diabetic myonecrosis in a previously healthy woman and review of a 25-year Mayo Clinic experience. Endocr Pract. 2002; 8: 343-346. 10.4158/ep.8.5.343.
- Horton WB, Taylor JS, Ragland TJ, Subauste AR. Diabetic muscle infarction: a systematic review. BMJ Open Diabetes Res Care. 2015; 3: 000082. 10.1136/bmjdrc-2015-000082.