
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
A complex case of severe acute hepatitis with cholestasis in a genetically predisposed woman: Could curcumin be the trigger?
Gabriele Domenico Gallina1*†; Giovanni Gobbin1†; Teresa D’Aliberti2; Luisa Ronzoni3; Luca Valenti3,4*; Federica Pedica1,5
1Università Vita-Salute San Raffaele, Milan, Italy.
2General Medicine with a Specialized and Continuity of Care Focus, IRCCS San Raffaele Scientific Institute, Milan, Italy.
3Biological Resource Center Unit, Transfusion Medicine, Fondazione IRCCS Ca’ Granda Major Hospital Polyclinic, Milan, Italy.
4Department of Pathophysiology and Transplantation, University of Milan, Milan, Italy.
5Pathology Unit, IRCCS San Raffaele Scientific Institute, Milan, Italy.
†Equal Contribution.
*Corresponding Author : Luca Valent
Biological Resource Center Unit, Transfusion Medicine, Fondazione IRCCS Ca’ Granda Major Hospital
Polyclinic, Milan, Italy.
Email: luca.valenti@unimi.it
Received : Jan 19, 2024
Accepted : Feb 02, 2024
Published : Feb 09, 2024
Archived : www.jcimcr.org
Copyright : © Valenti L (2024).
Abstract
Drug-Induced Liver Injury (DILI) can present as cholestatic hepatitis and differential diagnosis with other etiologies is often challenging. The established trend of growth in consumption of Herbal Dietary Supplements (HDS) by the general population underlines the necessity of timely suspicion and early recognition of its complications. In this context, turmeric-derived substances, such as curcumin, are among the most consumed. Some case reports have already described incidents of DILI induced by these substances. Moreover, genetic variants in genes encoding for the canalicular hepatobiliary transporters, mainly the phospholipid flippase MDR3 (encode by the ABCB4 gene) and the canalicular bile salt export pump BSEP (encoded by the ABCC11 gene), have been involved in the pathogenesis of DILI. We report the case of a woman, genetically predisposed to cholestatic events, who experienced a severe incident of acute cholestatic hepatitis, at least partially imputable to the consumption of multiple HDS, including turmericderived compounds.
Citation: Gallina G, Gobbin G, D’Aliberti T, Ronzoni L, Valenti L, et al. A complex case of severe acute hepatitis with cholestasis in a genetically predisposed woman: Could curcumin be the trigger?. J Clin Images Med Case Rep. 2024; 5(2): 2850.
Introduction
The differential diagnosis of intrahepatic cholestasis is often challenging and requires a thorough clinical and instrumental investigation [1]. Herbal Dietary Supplements (HDS) induced liver damage can manifest with patterns of hepatocellular or cholestatic injury, but commonly is mixed hepatocellular and cholestatic [2]. An accurate investigation on the recent intake of new substances is crucial, since iatrogenic causes may induce acute liver failure. The use of HDS has been steadily increasing in recent years. The variety and unpredictability of their compositions, the lack of rigorous regulations governing their production and marketing, together with the occasional reluctance of patients in revealing their usage, contribute to important challenges in the pharmacovigilance of their singular chemical components [3]. Moreover, genetic variants have been identified not only as direct causes of liver disease, but also as sensitizers to environmental toxic effects [2,4,5].
Case report
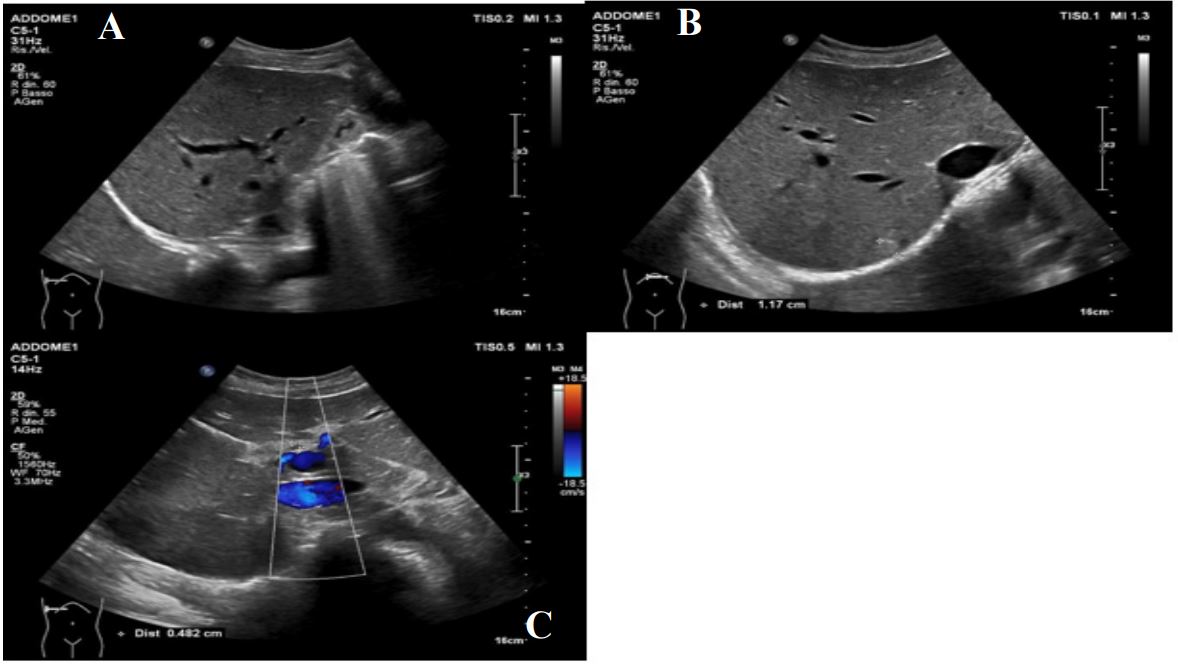
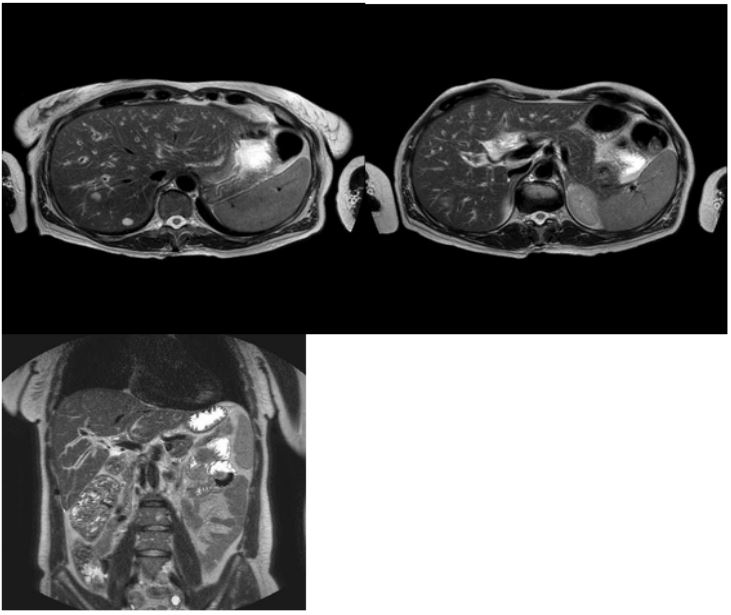
A 46-year-old woman presented to the Emergency Department complaining jaundice and pruritus, which had been developing gradually during the previous month. She had hyperchromic urine and hypocholic stools. During the same period, she reported occasional right-upper quadrant abdominal pain and mild nausea. No fever, no alcohol consumption. She was admitted to our General Medicine ward for further investigation. The laboratory test confirmed a mixed hepatocellular and cholestatic liver damage (Table 1), diagnosis of hemochromatosis was confidently ruled out. The biochemical panel and family history of the patient were not suggestive for any etiology (Tables 1, 2), but the patient remembered an episode of jaundice which affected one of her brothers during his childhood. The personal history of the patient was positive for a previous diagnosis of Gilbert’s syndrome and two previous episodes of Intrahepatic Cholestasis of Pregnancy (ICP), which were treated with UrsoDeoxycholic Acid (UDCA). An abdominal Ultrasound (US) Magnetic Resonance Cholangiopancreatography (MRCP) ruled out any obstructive causes of jaundice and signs of portal hypertension showing interstitial edema and reactive lymph nodes (Figures 1A, 1C and 2A-2C). Later on, the patient reported taking oral contraceptives without complications. In the previous 5 months, the patient had undertaken a ketogenic diet, with an impressive 35-kilogram drop in body weight (resulting in a body mass index drop from 38.87 to 29.34 kg/m² upon admission). The patient reported also the sporadic intake of several dietary supplements during that period, such as barberry, milk thistle, pineapple derived formulations, diosmin, alpha-lipoic acid, omega-3 fatty acids, group B vitamins, taurine, magnesium. Turmeric-based supplementations were taken instead for the whole period. They consisted of capsules containing 100 mg of curcumin (alongside with smaller quantities of ginger extract, vitamin C and D) and were consumed on a daily basis. A liver biopsy was ultimately performed on the ninth day of hospital stay. The liver biopsy showed a severe panlobular cholestasis together with the presence of an inflammatory population consisting of macrophages, neutrophils, eosinophils and lymphocytes, with rare plasma cells, affecting mainly the portal tract and involving the surrounding hepatocytes. This was associated with mild fibrosis and a minor involvement of the biliary ductal epithelium, ductular reaction and numerous metaplastic hepatocytes. The liver content of iron and copper was normal. Steatosis involved less than 5% of hepatocytes. These results were deemed to be consistent with acute cholestatic hepatitis and suggestive for a toxic iatrogenic effect (Figures 3A-3D).
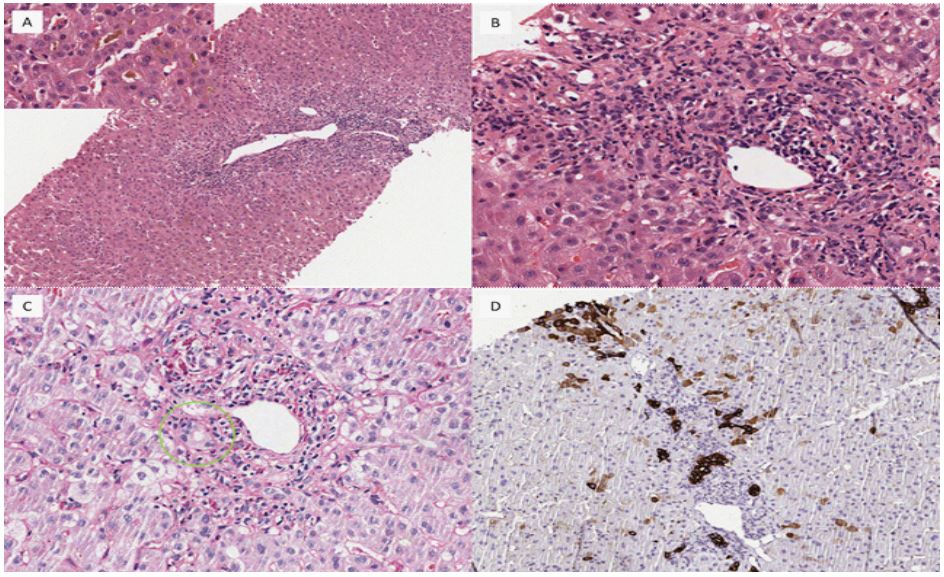
A - Hematoxylin-Eosin (HE) staining, 10x, showing panlobular, but mainly portal-based, inflammation in the context of a brownish parenchyma because of cholestasis; the latter is canalicular with bile plugs (high power view), and can be found in the hepatocytes as well.
B - HE staining, 20x, displaying a portal tract with dense inflammatory infiltrate including lymphocytes, macrophages, plasma cells, and numerous neutrophils and eosinophils.
C - Periodic acid-Schiff plus diastase (PAS-D), 10x, highlighting the presence of ceroid laden macrophages in the portal tract and some suffering cholangiocytes and clarified cytoplasm of the hepatocytes, because of feathery degeneration.
D - Immunohistochemistry for cytokeratin 7 (CK7), 20x, showing mild ductular reaction and numerous intermediate metaplastic hepatocytes positive for CK7 around the portal tract.
Table 1: Time course of blood counts and biochemical workup.
| Reference values |
AT admission (ED and 1st DAY) |
Middle (8th DAY) of hospital day |
AT discharge (18th DAY) |
3-Months folow-up | |
|---|---|---|---|---|---|
| B-Hb (g/dL) | 12-16 | 12.7 | 11.3 | 11.9 | |
| MCV (fL) | 81-99 | 85.6 | 86.1 | 100.0 | |
| WBC (cells/μL) | 4,800-10,800 | 7,000 | 8,800 | 9,200 | |
| PLTs (cells/μL) | 130,000-400,000 | 231,000 | 308,000 | 284,000 | |
| ESR (mm/h) | 1-20 | 24 | 27 | ||
| S-CRP (mg/L) | <6 | 2.4 | |||
| S-Sodium (mEq/L) | 135-148 | 139 | 136 | ||
| S-Potassium (mEq/L) | 3.5-5 | 4.4 | 4.1 | ||
|
S-Calcium (total - mmol/L) |
2.1-2.6 | 2.27 | 2.18 | ||
| S-AST (IU/L) | 5-33 | 469 | 109 | 81 | 111 |
| S-ALT (IU/L) | 6-41 | 798 | 236 | 90 | 90 |
| S-Total bilirubin (mg/dL) | 0.1-1 | 18.88 | 20.65 | 17.24 | 5.30 |
| S-Direct bilirubin (mg/dL) | 0.01-0.25 | 14.85 | 18.22 | 15.28 | 3.81 |
| S-Indirect bilirubin (mg/ dL) | 0.01-0.8 | 4.03 | 2.43 | 1.96 | 1.49 |
| S-GGT (IU/L) | 6-40 | 62 | 38 | 51 | 379 |
| S-ALP (IU/L) | 33-98 | 141 | 125 | 126 | 167 |
| S-LDH (IU/L) | 125-220 | 266 | |||
| S-Ammonium (μmol/L) | 9-50 | 38 | 31 | ||
| S-Creatinine (mg/dL) | 0.5-1.1 | 0.63 | 0.66 | 0.55 | |
| S-Albumin (g/L) | 35-50 | 31.9 | 32.6 | 37.9 | |
| S-pCHE (kIU/L) | 5.4-13.2 | 3.07 | 2.05 | 4.17 | |
| S-Iron (μg/dL) | 50-170 | 273 | |||
| S-TRF (mg/dL) | 200-330 | 221 | |||
| S-TSAT (%) | 15-45 | 88 | |||
| S-Ferritin (ng/mL) | 15-150 | 927 | 280 | ||
| S-Copper (μg/dL) | 56-165 | 173 | |||
| S-Ceruloplasmin (g/L) | 0.2-0.6 | 0.3 | |||
| S-Triglycerides (mg/dL) | <190 | 328 | |||
| S-Total cholesterol (mg/dL) | <150 | 201 | |||
| P-Fibrinogen (mg/dL) | 150-400 | 342 | |||
| PT (s) | <15 | 12.3 | 13.4 | 15.6 | 15.0 |
| aPTT (s) | <35 | 30.2 | 27.8 | 34.1 |
S-: Serum concentration; P-: Plasma Concentration; B-: Blood Concentration; Hb: Hemoglobin; MCV: Mean Corpuscular Volume; WBC: White Blood Cells; PLTs: Platelets; ESR: Erythrocyte Sedimentation Rate; CRP: C-Reactive Protein; AST: Aspartate Aminotransferase; ALT: Alanine Ami- notransferase; GGT: Gamma-Glutamyltransferase; ALP: Alkaline Phosphatase; LDH: Lactate Dehydrogenase; pCHE: pseudocholinesterase; TRF: Transferrin; TSAT: Transferrin Saturation; PT: Prothrombin Time; aPTT: activated Partial Thromboplastin Time.
Table 2: Serology with autoimmune panel, and molecular tests performed during hospitalization.
| Reference value | Result | |
|---|---|---|
| S-HbsAg | negative | negative |
| S-anti-HBs (mIU/mL) | — | >1000 |
| S-anti-HBc | negative | negative |
| S-anti-HAV (IgG and IgM) | negative | negative |
| S-anti-HEV (IgG and IgM) | negative | negative |
| S-anti-HCV | negative | negative |
| S-HCV RNA (mIU/mL) | <15 | negative |
| B-EBV DNA (IU/mL) | negative | negative |
| P-CMV DNA (IU/mL) | negative | negative |
|
S-Total gamma globulins (g/L) |
7-16 | 6.67 * |
| S-ANA (titer) | absent <1:80 | absent |
| S-ASMA (titer) | absent <1:40 | absent |
| S-anti-LKM (titer) | absent <1:40 | absent |
| S-p- and c-ANCA | absent | absent |
| S-AMA (AU) | <20 | 0.3 |
|
B-HFE gene C282Y and H63D mutations |
absent | absent |
HBsAg: Hepatitis B s Antigen; HBc: Hepatitis B c Antigen; HAV: Hepa- titis A Virus; HEV: Hepatitis E Virus; HCV: Hepatitis C Virus; EBV: Ep- stein-Barr virus; CMV: Cytomegalovirus; ANA: Antinuclear Antibodies; ASMA: Anti-Smooth Muscle Antibodies; Anti-LKM: Anti-liver/kidney Microsomal Antibodies; p- and c-ANCA: Perinuclear and Cytoplasmic Antineutrophil Antibodies; AMA: Anti-Mitochondrial Antibodies; HFE: Homeostatic iron regulator; AU: Arbitrary Units. *12.6% of the total serum proteins; no monoclonal peak was described at the electrophoretic run.
During the hospital stay, the patient remained symptomatic for pruritus, requiring the administration of antihistamine drugs, cholestyramine and off-label gabapentin, and mild nausea. An initial transitory progression of the already severe hyperbilirubinemia (Table 1) made it necessary to refer the patient for urgent liver transplant, with a Model for End-Stage Liver Disease (MELD) score of 18. However, the jaundice then gave initial signs of reversion, and the patient was discharged after 18 days of hospitalization. During the following weeks she experienced a very slow resolution of jaundice and, 3 months after discharge, direct bilirubinemia and cholestasis markers still remained above the upper normal limits, even if far below what we had observed (Table 1).
In the meantime, we also referred the patient for genetic counseling at the Biological Resource Center Unit, Transfusion Medicine, Fondazione IRCCS Ca’ Granda Ospedale Maggiore Policlinico, Milan, Italy. A high-resolution Array-Comparative Genomic Hybridization assay (Array-CGH, resolution 12.5 Kb, Agilent Technologies) ruled out clinically relevant deletions and duplications abnormalities. Next Generation Sequencing (NGS) of a targeted panel of 82 liver-related genes, comprising cholestatic genes, was performed [6]. A rare heterozygous variant in the Tight Junction Protein 2 (TJP2) gene (p.R24H, rs4493966), actually classified as benign according to ACMG guideline, was detected. Moreover, the patient carried a homozygous polymorphism in ABCB4 gene (c.540T>C; p.N168N; rs1202283) and a heterozygous one in ABCB11 gene (c.1331T>C: p.V444A; rs2287622), previously reported as common variants predisposing to ICP and DILI [7,8].
Discussion
The Roussel Uclaf Causality Assessment Method (RUCAM) scale is a pharmacovigilance tool commonly used to esteem the likelihood of hepatotoxicity in the setting of acute liver injury [9]. In our case, the result was 7, meaning that HDS-induced liver injury was the most probable cause of illness. In our case, the most suspicious HDS turned out to be curcumin, which is a natural yellow polyphenol extracted from the rhizome of turmeric (Curcuma longa). It has low bioavailability in its pure form, but turmeric drug supplements often contain piperine, a major active component of black pepper, increasing 20-fold the bioavailability of curcumin [10]. Some reports suggest potential adverse effects of curcumin on liver function [11-14]. Our patient had also two polymorphisms in ABCB4 and ABCB11 that could constitute a genetic background for recurrent episodes of liver injury, exacerbated by triggering factors such as pregnancy and HDS. The rare variant in TJP2, though classified as benign, could have had a role in genetic predisposition. Contextually, curcumin has been signaled as a substrate of the MDR3 transporter, expressed by the ABCB4 gene [15]. It is important to raise concern about tolerability and safety of HDS to prevent incidents of acute liver injury. Further studies are needed to investigate the toxicity spectrum of these compounds, which need regulamentation and medical surveillance [3].
References
- Assy N, et al. World Journal of Gastroenterology. 1999; 5(3): 252-262.
- Hoofnagle JH, et al. New England Journal of Medicine. 2019; 381(3): 264-273.
- Navarro VJ, et al. Hepatology. 2017; 65(1): 363-373.
- Stephens C, et al. Clinical Liver Disease. 2020; 24(1): 11-23.
- Stättermayer AF, et al. Journal of Hepatology. 2020; 73(3): 651-663.
- Ronzoni L, et al. Frontier Genetics. 2023; 14: 1137016.
- Falcão D, et al. Digestive and Liver Disease. 2022; 54(2): 221-227.
- Jüngst C, at al. Digestion. 2014; 90(2): 81-88.
- Danan G, et al. International Journal of Molecular Sciences. 2015; 17(1): 14.
- Vera-Ramirez L, et al. Biofactors. 2013; 39(1): 88-100.
- Chand S, Hair C, et al. Internal Medicine Journal. 2020; 50(2): 258-259.
- Lukefahr AL, et al. BMJ Case Reports. 2018.
- Lee BS, et al. ACG Case Reports Journal. 2020; 7(3): e00320.
- Luber RP, et al. Case Reports Hepatology. 2019.
- Wen C, et al. Molecular Medicine Reports. 2019; 19(6): 5162-5168.