Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 5
Multirecurrent hyperparathyroidism due to parathyromatosis
Stiliani Laskou1*; Paraskevi Axi1; Vasilios Rafailidis2; Ioanna Aba Nteka3; Triantafyllia Koletsa3; Konstantinos Sapalidis1
13rd Surgical Department, AHEPA University General Hospital, Aristotle University of Thessaloniki, Thessaloniki, Greece.
2Department of Radiology, AHEPA University General Hospital, Aristotle University of Thessaloniki, Thessaloniki, Greece.
3Department of Pathology, School of Medicine, Faculty of Health Sciences, Aristotle University of Thessaloniki, Thessaloniki, Greece.
*Corresponding Author : Stiliani Laskou
3rd Surgical Department, AHEPA University General Hospital, Aristotle University of Thessaloniki, Thessaloniki, Greece.
Email: stelaskou@gmail.com
Received : Jan 18, 2024
Accepted : Feb 02, 2024
Published : Feb 09, 2024
Archived : www.jcimcr.org
Copyright : © Laskou S (2024).
Abstract
Parathyromatosis is an extraordinary singleton condition, which is characterized by hyperfunctional parathyroid foci, mainly delineated in the neck, mediastinum, and generally in the transplantation site, if the cause is related to previous surgeries. We present the case of a successfully treated 66-year-old female patient suffering from recurrent hyper parathyroidism caused by parathyromatosis.
Citation: Laskou S, Axi P, Rafailidis V, Nteka IA, Koletsa T, et al. Multirecurrent hyperparathyroidism due to parathyromatosis. J Clin Images Med Case Rep. 2024; 5(2): 2851.
Background
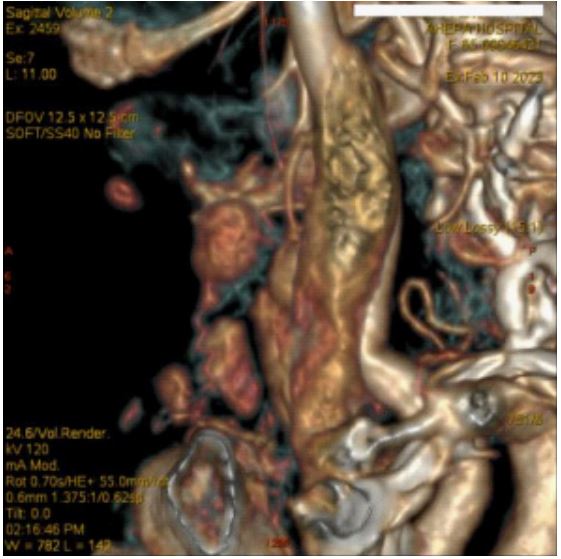
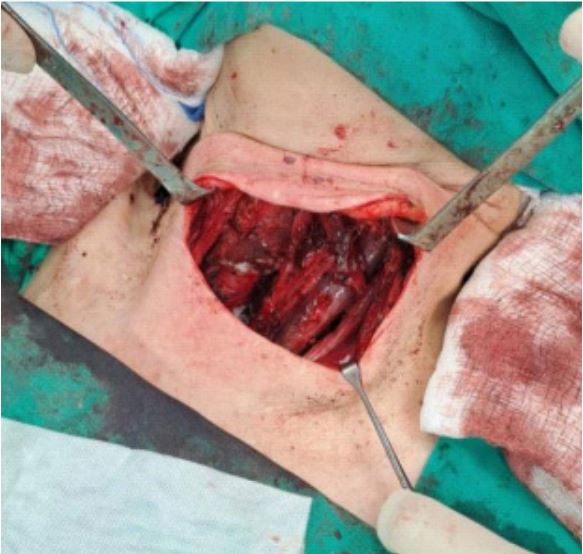
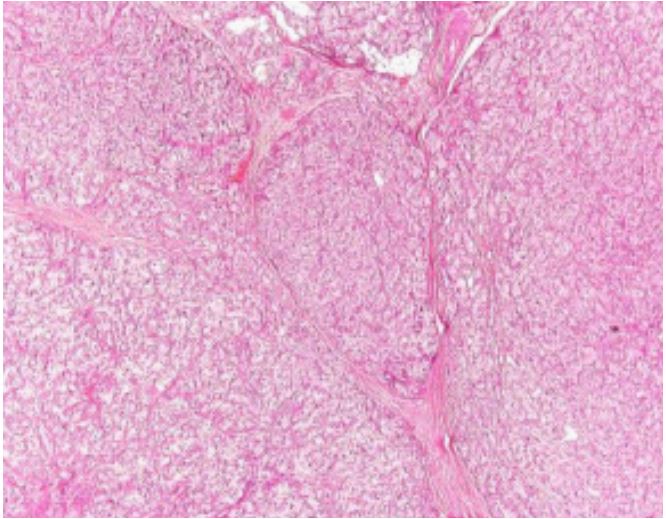
A 66-year-old woman was admitted to the emergency department complaining of nausea and vomiting. She had a clear medical history but a rather vague surgical history of 5 neck operations due to recurrent hyperparathyroidism the last 30 years which not only left her untreated but also with a paretic right vocal cord. On neck examination she had a transverse incision scar while several nodules could be palpated. Laboratory tests revealed a calcium level of 16 mg/dl and Parathormone (PTH) of 577 pg/ml. Neck ultrasonography showed multiple nodules suspicious for parathyromatosis, located along the anterior of the left sternocleidomastoid muscle and in the central neck compartment, findings also confirmed by 4D-CT (Figure 1). Considering the longstanding disease and its complications as well as the failure of medical treatment to succeed normocalcemia, central and left selective neck dissection (compartments II, II, IV) were performed (Figure 2). Intraoperatively, PTH levels decreased adequately to 52.4 pg/ml, while intraoperative neuromonitoring reassured the integrity of the left recurrent nerve. The patient was discharged with normal serum calcium and PTH levels. No signs of recurrence are observed at 1 year follow up. Histopathology report confirmed the diagnosis of parathyromatosis (Figures 3).