
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
An unusual instance of traumatic occult pharyngeal fistula
Lu-Lu Li1; Zhi-Hai Liu1; Tong Li2*
1Department of Emergency Medicine, The First Affiliated Hospital, School of Medicine, Zhejiang University, Hangzhou, 310003 Zhejiang, People’s Republic of China.
2Department of Critical Care Medicine, The First Affiliated Hospital, School of Medicine, Zhejiang University, Hangzhou, 310003 Zhejiang, People’s Republic of China.
*Corresponding Author : Tong Li
Department of Critical Care Medicine, The First
Affiliated Hospital, School of Medicine, Zhejiang
University, Hangzhou, 310003 Zhejiang, People’s
Republic of China.
Email: drli@zju.edu.cn
Received : Jan 19, 2024
Accepted : Feb 05, 2024
Published : Feb 12, 2024
Archived : www.jcimcr.org
Copyright : © Tong L (2024).
Abstract
Pharyngeal fistula is the most frequent complication after total laryngectomy, which is rare to occur in closed trauma and is also rarely reported in China. Traumatic pharyngeal fistula is a severe and rare disease that remains a diagnostic challenge nowadays. We present a 26-year-old male trauma case,two weeks later we discovered a pharyngeal fistula during a surgery for an axial fracture.
Keywords: Trauma; Pharyngeal fistula; Axial fracture.
Citation: Lu-Lu L, Zhi-Hai L, Tong L. An unusual instance of traumatic occult pharyngeal fistula. J Clin Images Med Case Rep. 2024; 5(2): 2852.
Introduction
Pharyngeal fistula refers to the accumulation of saliva under the skin or incision tissue, forming a purulent cavity that ruptures to the skin or incision edge, allowing the pharyngeal and esophageal cavities to connect with the skin and form a sinus. Through this sinus, saliva can overflow outside the skin, forming a skin fistula [1]. Traumatic pharyngeal fistula is rare. There has been only one detailed report of an aquired laryngo-pharyngeal fistula [2]. In this case, the fistula resulted from neck trauma caused by a dislocated cervical vertebra. The symptom was persistent aspiration. We describe a trauma-induced case without aspiration or other symptoms of pharyngeal fistula.
Case report
A 26-year-old man, with non significant past medical history, admitted to our department for a fall from a height of three meters four hours ago. Physical examination revealed body temperature: 37OC, pulse: 59 beats/min, respiration: 19 beats/min, blood pressure: 110/82 mmHg. GCS score 3+2+4. Multiple skin abrasions can be reached throughout the body. Examination of the abdomen, respiratory and cardiovascular systems revealed no abnormalities.
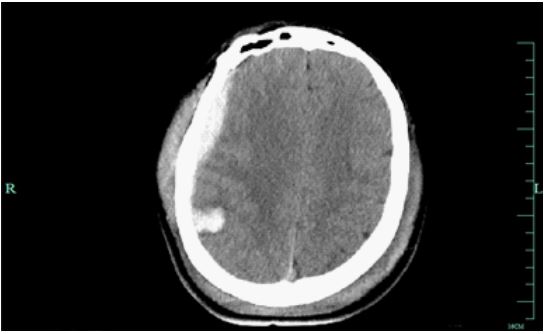
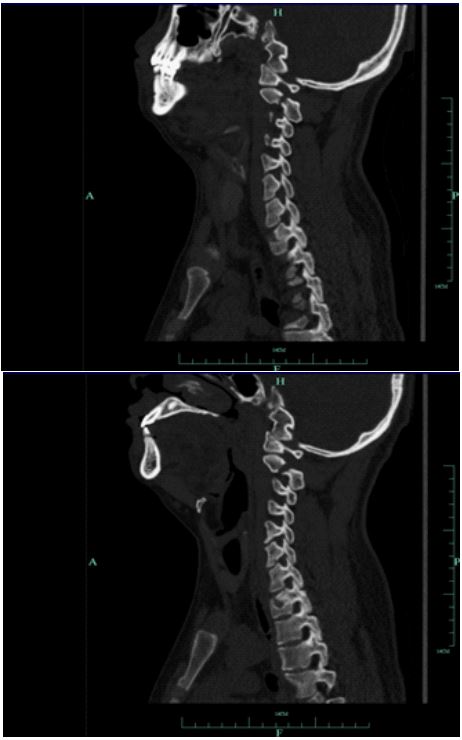
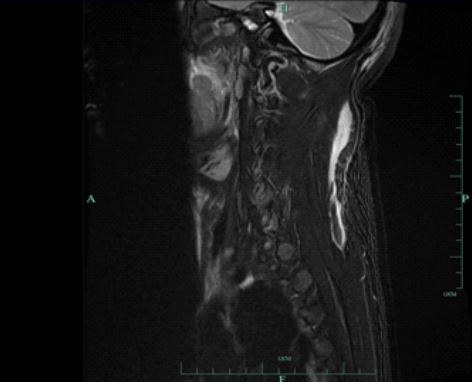
A brain Computed Tomography (CT) showed a right rated temporal subdural hematoma and an epidural hematoma, as well as a right parietal lobe hematoma. Subarachnoid hemorrhage. Fracture of both parietal bones. Extensive swelling of scalp soft tissue (Figure 1). A Cervicalvertebrae computed tomography (CT) + 3D reconstruction showed C2 bilateral vertebral arch fractures with surrounding soft tissue swelling (Figure 2). Magnetic resonance imaging of the cervical spinal cord showed fluid accumulation between the right trapezius muscle and the head muscle (Figure 3).
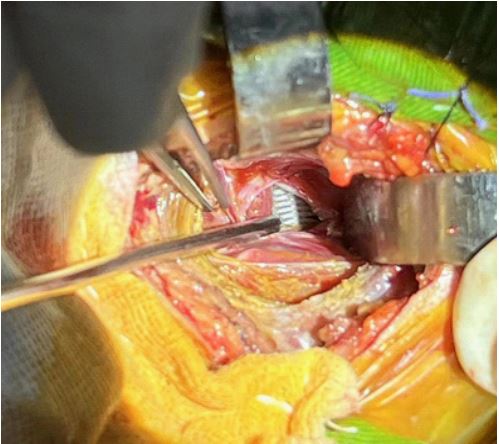
Patient was treated by emergency treatment for intracranial hematoma removal. Two weeks later, the patient planned to undergo surgery for an axial fracture. During the surgery, the chief orthopedic surgeon discovered a small, one centimeterlong tear in the pharyngeal posterior wall of the epiglottis, accompanied by a large amount of mucus exudation. The edge of the tear was a yellow ulcer, with visible tracheal cannula and fluid leaking into the surrounding soft tissue gap (Figure 4). During the emergency consultation between otolaryngology and general thoracic surgery, it was decided through multidisciplinary team to terminate the surgery for axial fractures and perform pharyngeal fistula flap repair. A month later, he was referred for rehabilitation treatment. He was conscious and coherent when discharged.
Discussion
Pharyngeal fistula is a common complication after head and neck tumor surgery, most commonly seen after total laryngectomy for hypopharyngeal and laryngeal cancer. The incidence of postoperative pharyngocutaneous fistula after major pharyngolaryngeal surgery ranges from 18 to 21% [3,4].
Here, we disclose an acquired case of traumatic occult pharyngeal fistula in a 26-year-old patient. Two weeks later, during the surgery for the axis fracture, we discovered the presence of pharyngeal fistula and promptly terminated the surgery for the fracture, repairing the pharyngeal fistula. This decision was made by a multidisciplinary team for better outcomes consider pharyngeal fistula as a result of trachea and surrounding soft tissue rupture after cervical hyperextension injury. It was decided to terminate the surgery for axial fractures and perform pharyngeal fistula flap repair.
The characteristics of the pharyngeal fistula in this case are that there are few or even no defects in the pharyngeal mucosa, and the direct closure tension is small, which is beneficial for healing; the fistula site has a certain degree of inflammation due to contact with saliva for up to two weeks. Although the patient’s prognosis in this case is good, the discovery of pharyngeal fistula two weeks later delayed the diagnosis and treatment of other traumas.
After the diagnosis and treatment of this patient, our experience is that for patients with neck trauma, whether it is open or closed trauma, the possibility of pharyngeal fistula should be considered; Pharyngeal fistula caused by neck trauma should be diagnosed and treated early after injury, properly sutured, and strive for primary healing.
This report clarified a rare and significant case of occult pharyngeal fistula caused by a high-altitude fall injury, so as to improve doctors’ attention to Pharyngeal fistula. This type of trauma should be diagnosed and treated as soon as possible to prevent its development into refractory pharyngeal fistula or even life-threatening. Future case reports are needed to provide a better overview of traumatic pharyngeal fistula, and clinical doctors need to be vigilant about the possibility of missed diagnosis.
Conclusion
The diagnosis of a laryngo-pharyngeal fistula should be considered in the diagnosis of trauma to the cervical vertebrae. Unfortunately, however, this situation is easily overlooked in clinical practice. We have reported this case in the hope that clinical doctors will be more vigilant.
Declarations
Data availability: Data can be provided on reader’s request.
Contributors: Lu-Lu Li, Zhi-hai Liu,Tong Li.
Patient consent: Obtained.
Financial support and sponsorship: Nil.
Conflicts of interest: There are no conflicts of interest.
Acknowledgements: We would like to thank for ShengZhang, Ph.D., providing the help on statistical analyses.
References
- Liu Yinan, Li Dan. The causes and management of pharyngeal fistula after laryngeal cancer surgery [J] Jilin Medicine. 2009; 30(1): 70-72.
- Hirano M, Ohkubo H. Acquired laryngo-pharyngeal fistula. J Laryngol Otol. 1986; 100(6): 719-22.
- White H N, Golden B, sweeny L, et al. Assessment and incidence of salivary leak foUowing 1aryngectomy[J], Laryngoscope, 2012; 122(8): 1796-1799.
- Makitie A A, Niemensivu R, Hero M, et al. Pharyngocutaneous fistula following total laryngectomy: A single institution’s 10- year experience[J]. Eur Arch Otorhinolaryngol. 2006; 263(12): 1127-1130.