
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Presentation of multiple myeloma through cranial pair atrophy
Anabela De Carvalho*; Ângela Almeida; Ussumane Embaló; Jorge Cotter
Internal Medicine Department, Hospital Senhora da Oliveira, Guimarães, Portugal.
*Corresponding Author : Anabela De Carvalho
nternal Medicine Department, Hospital Senhora da
Oliveira, Guimarães, Portugal.
Email: belinha_carvalho_7@hotmail.com
Received : Jan 22, 2024
Accepted : Feb 08, 2024
Published : Feb 15, 2024
Archived : www.jcimcr.org
Copyright : © Carvalho AD (2024).
Abstract
Multiple Myeloma (MM) accounts for 1% of all cancers and approximately 10% of all hematologic malignancies. The diagnosis of multiple myeloma requires the presence of one or more Myeloma Defining Events (MDE) in addition to evidence of either 10% or more clonal plasma cells in bone marrow examination or a biopsy-proven plasmacytoma. Bone involvement is the most frequent clinical manifestation. Other common manifestations include hypercalcemia, renal failure and normocytic normochromic anemia. A limited number of patients develop extramedullary disease over the course of the disease. Here, we present a case of a 53-year-old women who presented to the emergency department with dysphonia and dysphagia. On clinical exam she presented atrophy of the left hypoglossal, vagus and glossopharyngeal cranial nerves. The analytical study and computed tomography showed no significant changes. The extensive study documented the presence of an intracranial plasmacytoma and posterior confirmation of MM. Primary presentation with neurological symptoms due to intracranial plasmacytomas are rare. The aim of this case report is to highlight the importance of considering atypical presentations of MM for a rapid diagnosis and referral to a multidisciplinary team.
Keywords: Multiple myeloma; Cranial nerve atrophy; Plasmacytoma.
Citation: Carvalho AD, Almeida A, Embaló U, Cotter J. Presentation of multiple myeloma through cranial pair atrophy. J Clin Images Med Case Rep. 2024; 5(2): 2860.
Introduction
Multiple Myeloma (MM) is responsible for approximately 1 percent (%) of all neoplasms and approximately 10% of hematological neoplasms [1]. Worldwide, there are approximately 160,000 cases and 106,000 deaths per year attributed to MM [2]. The average age of diagnosis is 65 years, being more common in men [1]. Bone disease is the most frequent clinical manifestation, affecting 70 to 95% of patients. Other clinical manifestations include hypercalcemia (13%), renal failure (25%), and usually normocytic normochromic anemia (80%) [3,4]. Approximately 1 to 2% of patients have extramedullary disease at the time of initial diagnosis, while 8% develop extramedullary disease over the course of the disease [5]. Almost all MM patients progress from asymptomatic premalignant disease (monoclonal gammopathy of undetermined significance - MGUS) to MM at a rate of 1% per year [1]. The diagnosis is confirmed by the presence of 10% of plasma cells in the bone marrow and monoclonal proteins in the plasma or urine, associated with the presence of myeloma-defining events (organic lesions described by the CRAB mnemonic: Calcium, Renal insufficiency, Anemia, Bone lesions) [6,7].
The aim of this article is to describe a rare case of a woman with atypical clinical manifestations whose diagnosis was based on lesions identified on Magnetic Resonance Imaging (MRI) that had not been evaluated until then.
Case description
A 53-year-old woman with a history of hypertension, atrial fibrillation, colloid thyroid nodule, post-menopausal hemorrhages, chronic gastritis, reflux esophagitis and depression, presented to the Emergency Department (ED) because of dysphonia and dysphagia with 8 days duration. On clinical exam, she was noted to have atrophy of the left half of the tongue, paralysis of the left hemilarynx, loss of the vomiting reflex on the left and decreased taste sensitivity at the base of the tongue on the left, corresponding to the hypoglossal (XII), vagus (X) and glossopharyngeal (IX) cranial nerves (Figure 1).

At admission, there were no significant analytical changes and the Cranioencephalic (CE) and neck vessels Computed Tomography (CT) with angiography was normal. She was admitted to the Internal Medicine Department for study.
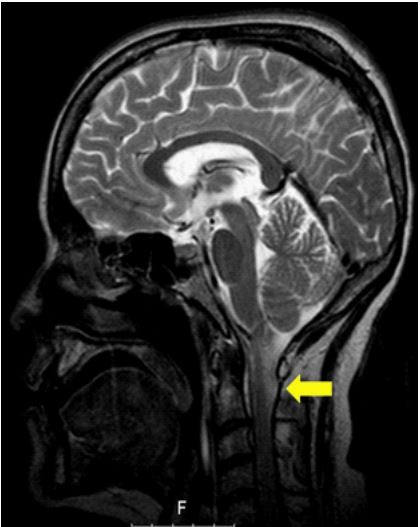
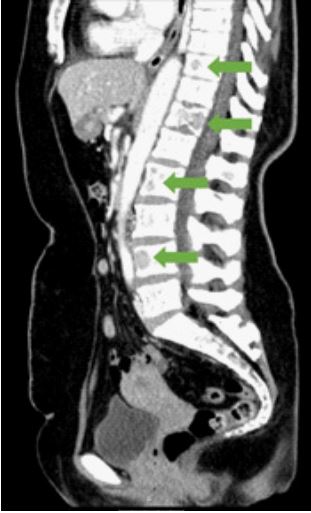
The patient underwent a lumbar puncture with a request for investigation of oligoclonal bands in the cerebrospinal fluid, which was negative. On suspicion of a compressive cause, a cervical and thoracic CT was performed, which revealed multiple lucent images, the most evident occupying almost the entire body of the Thoracic spine (Th) vertebra 12. CE Magnetic Resonance Imaging (MRI) showed a contrast-enhancing lesion measuring 2.6x1.7 centimeters (cm) on the left anterolateral margin of the foramen magnum and occipital condyle (Figure 2), with focal bone expansion and invasion of the jugular hole, small lesions in the skullcap and lytic lesions of the bodies of Th8, Th10- Th12, lumbar spine (L) vertebra 2 and L4 (Figure 3).
In view of the bone lesions, a more targeted and extended study was performed and a set of hematological and biochemical alterations were documented (Table 1): normochromic normocytic anemia, increased sedimentation velocity, Immunoglobulin (Ig) A deficiency, narrow-base monoclonal beta-2 peak (40.1%), increased beta-2 microglobulin, immunoelectrophoresis with IgG monoclonal peak of kappa chains with an increase in the Kappa/Lambda ratio, and 37% of plasma cells with atypical morphology in the bone marrow.
Table 1: Documented hematological and biochemical alterations.
| Laboratory test | Patient value | Normal value |
|---|---|---|
|
Hemoglobin - MCV; MCHC |
11.4 g/dL - 86 fL; 35.1 g/dL |
12-16 g/dL - 83-103 fL; 32-36 g/dL |
| Sedimentation velocity | 120 mm | 0-19 mm |
| IgA | 5 mg/dL | 114-457 mg/dL |
| IgG | 4150 mg/dL | 793-1500 mg/dL |
| Beta-2 microglobulin | 0.39 mg/dL | 0.19-0.253 mg/dL |
|
Immunoelectrophoresis: - Kappa - Lambda - Kappa/Lambda ratio |
848 mg/dL 34.3 mg/dL 24.72 |
0.76-1.46 mg/dL 90-210 mg/dL 1.35-2.70 |
dL: deciliter; fL: femtoliters; g: gram; Ig: immunoglobulin; MCV: Mean Corpuscular Volume; MCHC: Mean Corpuscular Hemoglobin Concentration; mg: milligram; mm: millimeter.
During hospitalization, the patient did not reveal renal damage or hypercalcemia. Still in hospital, due to severe dysphagia, the patient underwent percutaneous endoscopic gastrostomy.
Due to the diagnosis of MM, she was transferred to the hematological oncology service, having started treatment with cyclophosphamide, dexamethasone and bortezomib and radiotherapy directed at the plasmacytoma. During the third cycle, the disease progressed with hypercalcemia, acute kidney injury and a new expansive lesion in the occipital bone and another extra-axial lesion in the right great wing of the sphenoid, with moderate intracranial expression, deforming the anterior and right lateral temporal parenchyma, having to be hospitalized for intensive chemotherapy with cisplatin, adriamycin, cyclophosphamide and etoposide (PACE), having performed 2 cycles. The patient also developed numb-chin syndrome, with paresthesia in the chin region due to a myeloma lesion in the left mandibular ramus, compromising the inferior alveolar nerve and with atrophy and fat infiltration of the left hemilarynx, documented in CE and facial MRI. The patient underwent bone marrow autotransplantation, however she died shortly afterwards from disease progression.
Discussion
Osteolytic lesions are seen in 70 to 80% of patients with MM. Bone involvement, often associated with tumor extension into the surrounding soft tissues, can manifest as bone pain, pathological fractures and neurological impairment when spinal cord and/or cranial nerves are compressed [3,4]. Plasmacytomas are malignant neoplasms of mature B cells characterized by abnormal immunoglobulin secretion. Intracranial plasmacytomas are rare and almost always represent extensions of myelomatous lesions of the skull or plasmacytomas involving the clivus or the base of the skull [8].
This case describes a patient with dysphonia and dysphagia that presented with neurological alterations. Despite initial investigation being normal (blood analysis, head CT and lumbar puncture), the unusual presentation led to the suspicion of a possible compressive cause. CE MRI documented a lesion in the cranial base and multiple bone lesion that motivated an extensive etiological investigation. The final diagnosis of MM in a patient that only presented anemia during hospitalization, without hypercalcemia or renal failure made this diagnosis challenging. The presence of a plasmacytoma causing neurological symptoms as clinical presentation makes this case rarer and demonstrates the importance of investigation of hematological diseases.
Conclusion
MM is a hematological neoplasm that typically presents with haemoglobin, renal and calcium changes and bone lesions. Physicians should be alerted to the fact that a rare number of patients may present with neurological defects as an initial form of the disease due to intracranial plasmacytomas. Hence, it is crucial to alert physicians about this presentation to allow an early diagnosis, as well as referral to multidisciplinary care to initiate treatment, prevent complications, and reduce morbidity.
Declarations
Conflict of interest: The authors declare no conflict of interest.
Patient consent: Written informed consent from patients was obtained, to secure permission for publishing their clinical history.
Acknowledgments: No support or funding was received.
References
- Rajkumar SV: Multiple myeloma: 2020 update on diagnosis, riskstratification and management. American journal of hematology. 2020; 95: 548-567.
- Cowan AJ, Allen C, Barac A, et al.: Global Burden of Multiple Myeloma: A Systematic Analysis for the Global Burden of Disease Study 2016. JAMA Oncology. 2018; 4: 1221-1227.
- Tsang RW, Campbell BA, Goda JS, et al.: Radiation Therapy for Solitary Plasmacytoma and Multiple Myeloma: Guidelines From the International Lymphoma Radiation Oncology Group. International Journal of Radiation Oncology Biology Physics. 2018; 101: 794-808.
- Kyle RA, Gertz MA, Witzig TE, et al.: Review of 1027 patients with newly diagnosed multiple myeloma. Mayo Clinic Proceedings. 2003, 78: 21-33.
- Rajkumar, SV: Multiple myeloma: 2016 update on diagnosis, risk-stratification, and management. American journal of hematology. 2016; 91: 719-734.
- Rajkumar SV, Dimopoulos MA, Palumbo A, et al.: International Myeloma Working Group Updated criteria for the diagnosis of multiple myeloma. The Lancet Oncology. 2014; 15: 538-548.
- Godard H, Hirbe A, Nassif M, Otepka H, Rosenstock A: The Washington Manuel of Medical Therapeutics. Department of Medicine, Washington University School of Medicine (ed): Wolters Kluwer. 2013.
- Gozzetti A, Cerase A, Lotti F, et al.: Extramedullary intracranial localization of multiple myeloma and treatment with novel agents: a retrospective survey of 50 patients. Cancer. 2012; 118: 1574-1584.