
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Carcinoma squamous cell, are healthcare professionals prepared to identify it?
*Corresponding Author : David Hadson Arroyo
Department of Dental Surgery, São José do Rio
Preto, SP, Brazil.
Email: david.hadson.arroyo@gmail.com
Received : Jan 23, 2024
Accepted : Feb 08, 2024
Published : Feb 15, 2024
Archived : www.jcimcr.org
Copyright : © Arroyo DH (2024).
Abstract
Squamous Cell Carcinoma (SCC), is a type of cancer that originates in the squamous cells of the skin and has different stages according to the involved cellular layer. In the early stage, the process begins with chronic sun exposure, leading to DNA damage in the squamous cells of the epidermis. Initiating in pre-cancerous lesions such as actinic keratosis, occurring in the outermost layers of the epidermis. In the intermediate stage, squamous cells undergo additional mutations, becoming cancerous but still restricted to the epithelial layer without invading deeper structures. While it is only in the epidermis, it is considered carcinoma in situ, as it is confined to this cellular layer and has not invaded the basement membrane. In the advanced stage, cancer cells invade the deeper layers of the epidermis, crossing the basement membrane, becoming basal cell cancer and can reach the dermis. After reaching the dermis, cancer cells have the potential to spread to distant areas from the primary site, where the metastasis process begins and occurs, potentially affecting regional lymph nodes and other organs. In addition to the layers of the skin, cancer cells can spread to other tissues and organs, forming metastases that are cellular copies of their site of origin. At all stages, it is crucial to emphasize that the progression of squamous cell carcinoma involves progressive genetic mutations that confer malignant characteristics to the cells. Early diagnosis and treatment are essential to improve recovery prospects. Furthermore, prevention by avoiding alcohol, tobacco, and adequate sun protection plays a crucial role in reducing the risk of developing this type of cancer.
Keywords: Squamous cell carcinoma; Oral cancer; Spikes protocol.
Citation: Arroyo DH. Carcinoma squamous cell, are healthcare professionals prepared to identify it?. J Clin Images Med Case Rep. 2024; 5(2): 2861.
Introduction
Labial squamous cell carcinoma is a form of skin cancer that affects the lips, primarily the lower lip [16]. It develops from squamous cells, which compose the outermost layer of the skin [20]. The main cause of this type of cancer is associated with chronic sun exposure and ultraviolet radiation, being more common in individuals with fair skin. The progression of labial squamous cell carcinoma goes through various stages [33]. Initially, cells begin to undergo genetic mutations that make them abnormal, leading to the formation of pre-cancerous lesions, such as actinic keratosis [29,30]. Over time and continued exposure to risk factors, these lesions can progress to potentially malignant [16,34]. Initial symptoms may include persistent sores on the lips, red or white patches, swelling, or hardening of the skin. As the cancer advances, there may be ulceration, bleeding, and pain. Spread to surrounding tissues and even to the lymph nodes is possible, increasing the severity of the condition. Diagnosis typically involves clinical examinations, biopsies, and, in some cases, imaging tests. Treatment may include surgery to remove the tumor, radiotherapy, or even chemotherapy. Early detection is crucial to improving the chances of successful treatment. Prevention of labial squamous cell carcinoma involves adequate sun protection, especially in areas of high sun exposure, such as the lips. The use of hats and lip balm with Sunscreen (SPF) is recommended, avoiding excessive sun exposure, especially during peak hours [16].
Case report
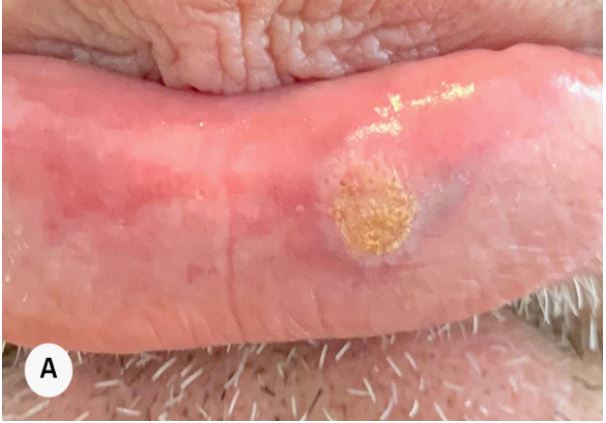
A 47-year-old male, an Agronomist Engineer and tobacco user, who spends a significant part of his day under unprotected sun exposure to the head and lips, where harmful rays directly affect his skin, was a determining factor for the appearance of neoplastic tissue on his lower lip [1,3,6,10,31]. Upon noticing the neoplastic tissue, he immediately sought medical help. Initially measuring around 1 mm, he consulted six healthcare professionals seeking guidance, but none of them could evaluate him significantly, recommending the use of Omcilon-A, a topical ointment with anti-inflammatory purposes. Persisting in the treatment without improvement, the patient sought more professionals as the lesion showed no regression, developing each week. In a short period, regardless of age being a relevant factor [11], the initially 1mm lesion progressed significantly to 9 mm in just 2 months.
The case illustrates that contemporary men are more concerned about health for a better quality of life [13], and the professionals assisting them must adapt to this change, especially in the method of information delivery, as the patient demonstrated significant fear and extreme concern about previous consultations. Therefore, the SPIKES protocol was applied to the patient [27,12].
During the consultation, visibly worried, he came to the office and was promptly attended to, with all information and hypotheses provided with confidence to avoid worsening the initial situation, especially since a biopsy would be performed at the site, leading to substantial tissue loss on the lower lip, compromising its aesthetics [4], as this approach is mandatory and adopted in all lesions in the oral cavity that do not regress within 14 days [14].
An excisional biopsy was performed, and the sample was sent to the pathology center, confirming a Squamous Cell Carcinoma (SCC). SCC is the sixth most common malignancy [9] in the oral cavity, with a 5-year survival rate reducing by 50% in the presence of lymph node metastasis [2]. SCC affects unevenly [5], being 7 times more common in male patients [7], and it has been reported that 70% to 90% of these cancers are related to tobacco [16]. Head and neck cancers represent 80% to 90% of malignancies in the Brazilian population [32].
After the diagnosis, the patient was referred to an Oncologist, where staging was performed, and no metastasis was demonstrated in the cervical lymph nodes [8,28].
Treatment
Before the surgical procedure, the patient underwent antiinflammatory medication (oral administration of 8 mg dexamethasone 2 hours before the procedure [15], Teuto Brasileiro SA, Anápolis, GO, Brazil) and gargles with 0.12% chlorhexidine gluconate (Colgate-Palmolive Company, New York, United States). An extraoral disinfection with 10% iodopovidone (São José do Rio Preto, São Paulo, Brazil) was performed, and local anesthesia with 4% articaine with 1:100,000 adrenaline (DFL Indústria e Comércio S/A, Rio de Janeiro, RJ, Brazil) was applied [22]. For a surgical approach and considering the aesthetic region, an elliptical incision was chosen as described by Mohs [23,24] with a number 15 blade, where safety margins were only 3mm in all axes after lesion delimitation, a high risk since publications inform 5mm [28], but the patient was made aware of the situation. Performing a wedge biopsy in this region would significantly alter the patient’s emotional aspect, and it is already known in the technical field that unhappy patients have poor recovery. In a study with 1,314 patients, it reported a statistically significant effect of preoperative depression [35]. The neoplastic tissue was fixed in 4% formaldehyde solution diluted in 0.1M phosphate-buffered saline (pH-7.4) and submitted to histopathological analysis (DAP - Pathology Laboratory, São José do Rio Preto, São Paulo, Brazil). Microscopic images showed a highly invasive Squamous Cell Carcinoma (SCC), where SCC originates from squamous cells of the epidermis, the outermost layer of the skin, composed of various cell layers. SCC usually develops from squamous cells located in the most superficial layer of the epidermis [20]. The involved tissues were repositioned with nylon 6-0 thread (Shalon, Sertix, São Luís de Montes Belos, Goiás, Brazil). For topical use over the post-suture wound to prevent possible edema, the patient could bite the region; Omcilon-A Orabase (Aspen Pharma, South Africa) was applied. Antibiotic (oral administration of 500 mg amoxicillin, every 12 hours for 3 days, Sanofi Medley Pharmaceuticals Ltd, Campinas, São Paulo, Brazil) and anti-inflammatory (oral administration of 100 mg nimesulide, every 12 hours for 3 days, Eurofarma, São Paulo, São Paulo, Brazil) were indicated for postoperative therapy, with 0.12% chlorhexidine gluconate (Colgate-Palmolive Company, New York, United States). It is important to mention that the patient agreed with the indicated treatment plan for his specific case.
Results and follow-up
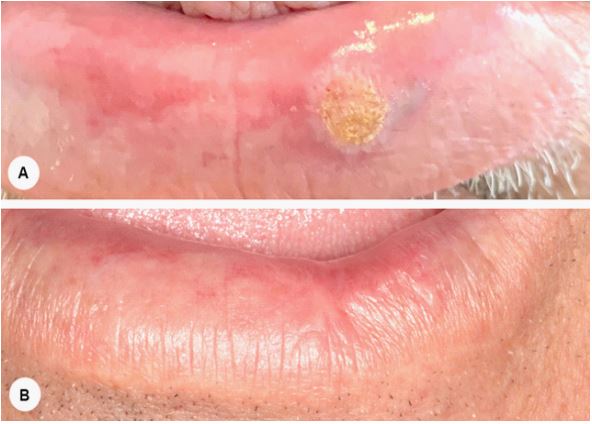
The patient returned after 7 days for clinical evaluation and suture removal. No changes in soft tissues were observed, and he reported no pain, redness, or any abnormalities related to cardinal signs of inflammation [36]. The patient reported some discomfort when trying to hydrate the lip with lip sunscreen. This occurred due to the suture in the region and was expected because it is a very sensitive area. The patient was advised to consult a head and neck oncologist to monitor the case’s progression and staging [16]. After examinations, no tactile changes were identified in the lymph nodes, blood tests, and ultrasound. Twelve months have passed, with two returns to the oncologist repeating these exams, and the patient has progressed well, showing no signs of neoplasia or any recurrence, positively corroborating the surgical technique where the lesion was removed.
Discussion
In this study, it was possible to observe one of the most common head and neck cancers, mainly affecting patients exposed to the sun without using sun protection such as hats and topical products on the skin or lips [16]. One-third of oral carcinomas are close to transforming into a malignant lesion, ranging from 1.4% to 12% of cases [16]. This will vary depending on clinical appearance, gender, location, etiological factors, and age.
With approximately 1,500,000 head and neck cancer patients worldwide, the mortality rate is 500,000. In Brazil, 20% of cancer-related deaths are associated with malignant tumors, with about 60,000 new cases. Head and neck cancer in Brazil ranks 3rd in causing deaths. Men have a prevalence 4 times higher in cancer incidence than females, with approximately 7,000 deaths per year in the country [17,18]. The most well-known risk factors include smoking and alcohol consumption, with the risk being 30 times higher for individuals who smoke and drink than for those who do not [19,20]. Among other risk factors is exposure to the sun without protection (significant risk for lip cancer), excess body fat, HPV infection (related to oropharyngeal cancer), and factors related to occupational exposure [20]. Under intense sun exposure, such patients should use sunscreen significantly reducing the occurrence of cancers [21], protecting healthy tissue against ultraviolet waves [22].
In the laboratory analysis, it was possible to observe the invasion of squamous cells very deeply but not reaching the basal layer. Several techniques could be used in the case at hand, such as Conventional Excision Surgery, Mohs Surgery, Electrosurgery (Curettage and Electrocoagulation), Cryosurgery, Radiotherapy, Topical Chemotherapy, Topical Immunotherapy [25,26]. However, due to professional expertise, excisional biopsy was chosen, as other techniques fall under the competence of the Oncologist [8,28]. The treatment of choice was defined by some factors, such as emotional aspect, clinical aspects, and anatomical characteristics.
Finally, after patient follow-up, he did not lose sensitivity in the region. Caution was still taken regarding the patient’s desire not to leave him looking “disfigured” since appearance could significantly compromise his self-esteem. On the second return at 12 months, the patient quit smoking, maintained a healthy diet, engaged in physical activity, losing about 15 kilograms. This demonstrates the importance of conducting a thorough evaluation for each specific case, as all patients are unique with individual characteristics.
References
- Rezende HD, Oliveira D, Campos MS, Fukuma LO, Delgado JC, Dinato SLM. Actinic cheilitis or squamous cell carcinoma of the lip? Practical recommendations on how to avoid a trap. Rev Assoc Med Bras (1992). 2022; 68(7): 877-878. doi: 10.1590/1806-9282.20220435. PMID: 35946758; PMCID: PMC9574951.
- Lack of documentation of lymph node examination in patients Eickstaedt JB, Fancher W, Havighurst T, Xu YG. Lack of documentation of lymph node examination in patients with squamous cell carcinoma of the lower lip. Arch Dermatol Res. 2022; 314(10): 1003-1006. doi: 10.1007/s00403-021-02281-4. Epub 2021 Sep 25. PMID: 34562138.
- Hwang JR, Khachemoune A. Lower lip basal cell and squamous cell carcinomas: a reappraisal of the similarities and differences in clinical presentation and management. Arch Dermatol Res.2023; 315(2): 117-125. doi: 10.1007/s00403-022-02345-z. Epub 2022 Mar 21. PMID: 35312855.
- Lozev I, Pidakev I, Batashki I, Kandathil LJ, Oliveira N, Tchernev G. Karapandzic flap as most adequate surgical approach for squamous cell carcinoma of the lower lip. Dermatol Reports. 2022; 14(3): 9439. doi: 10.4081/dr.2022.9439. PMID: 36199898; PMCID: PMC9527682.
- Tan B, Seth I, Fischer O, Hewitt L, Melville G, Bulloch G, Ashford B. Sex Disparity for Patients with Cutaneous Squamous Cell Carcinoma of the Head and Neck: A Systematic Review. Cancers (Basel). 2022; 14(23): 5830. doi: 10.3390/cancers14235830. PMID: 36497312; PMCID: PMC9740937.
- Roberts FW. Review of Cases of Squamous Cell Carcinoma of the Lip at the New Haven Hospital from January 1, 1920, to November 1, 1931. Yale J Biol Med. 193; 4(2): 187-98. PMID: 21433514; PMCID: PMC2606358.
- ZAVAREZ, Larrissa Balbo. Análise de recidiva em pacientes com carcinoma espinocelular de boca e orofaringe. 2011. 26 f. Trabalho de conclusão de curso (bacharelado - Odontologia) - Universidade Estadual Paulista Julio de Mesquita Filho, Faculdade de Odontologia de Araçatuba. 2011.
- BASSO, Juliana Maria. Fatores prognósticos do carcinoma espinocelular de boca. 2009. 21 f. +. Trabalho de conclusão de curso (bacharelado - Odontologia) - Universidade Estadual Paulista Julio de Mesquita Filho, Faculdade de Odontologia de Araçatuba. 2009.
- Oliveira, Maykon Kennedy Schulz. Expressão de CD10, Vimentina, Ki-67 e Ciclina D1 em carcinomas espinocelulares de cabeça e pescoço: avaliação clínico-patológica. Dissertações - Ciências Odontológicas - FOAR -Universidade Estadual Paulista Julio de Mesquita Filho, Faculdade de Odontologia de Araçatuba. 2018.
- FRARE, Juliana Cristina. Análise das características clinicopatológicas de carcinomas espinocelulares orais e pacientes jovens provenientes de Cascavel - Paraná: Analysis of clinicopathological features of oral squamous cell carcinoma in young patients from Cascavel - Paraná. 2015. 57 f. Tese (doutorado) - Universidade Estadual de Campinas, Faculdade de Odontologia de Piracicaba, Piracicaba, SP. Disponível em: https://hdl.handle.net/20.500.12733/1624653. Acesso em. 2023.
- SANTOS-SILVA, Alan Roger. Analise das caracteristicas clinico-patologicas e da ploidia do DNA em pacientes jovens com carcinoma espinocelular de lingua: um estudo colaborativo internacional. 2010; 57. Tese (doutorado) - Universidade Estadual de Campinas, Faculdade de Odontologia de Piracicaba, Piracicaba, SP. Disponível em: https://hdl.handle.net/20.500.12733/1611795. Acesso em: 20 mar. 2023.
- Martins BNFL, Migliorati CA, Ribeiro AC, Martins MD, Brandão TB, Lopes MA, et al. The barriers dentists face to communicate cancer diagnosis: self-assessment based on SPIKES protocol. Med Oral Patol Oral Cir Bucal. 2023; 28 (2): 191-8.
- Araújo DSMS de, Araújo CGS de. Aptidão física, saúde e qualidade de vida relacionada à saúde em adultos. Rev Bras Med Esporte [Internet]. 2000; 6(5): 194-203. Available from: https://doi.org/10.1590/S1517-86922000000500005.
- NEVILLE, B.; et al. Patologia Oral e Maxilofacial. 4. ed. Rio de Janeiro: Elsevier. 2016.
- Alexander RE, Throndson RR. Uma revisão do uso perioperatório de corticosteróides em cirurgia dentoalveolar. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2000; 90: 406-415.
- Almeida, Oslei; Abeno 5 - Patologia Oral Paes De Artes Medicas. ABENO-5-Cap6-REV 30set. 2016.
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018 Nov;68(6):394-424. doi: 10.3322/caac.21492. Epub 2018 Sep 12. Erratum in: CA Cancer J Clin. 2020; 70(4): 313. PMID: 30207593.
- Speight PM, Khurram SA, Kujan O. Oral potentially malignant disorders: risk of progression to malignancy. Oral Surg Oral Med Oral Pathol Oral Radiol. 2018; 125(6): 612-627. doi: 10.1016/j.oooo.2017.12.011. Epub 2017 Dec 29. PMID: 29396319.
- American Cancer Society. Cancer Facts & Figures 2019. Atlanta: American Cancer Society. 2019.
- Instituto Nacional de Câncer José Alencar Gomes da Silva. Estimativa 2020: incidência de câncer no Brasil / Instituto Nacional de Câncer José Alencar Gomes da Silva. – Rio de Janeir: INCA. 2019.
- Lundeen RC, Langlais RP, Terezhalmy GT. Sunscreen protection for lip mucosa: a review and update. J Am Dent Assoc. 1985; 111(4): 617-21. doi: 10.14219/jada.archive.1985.0157. PMID: 3877087.
- Busick TL, Uchida T, Wagner RF Jr. Preventing ultraviolet light lip injury: beachgoer awareness about lip cancer risk factors and lip protection behavior. Dermatol Surg. 2005; 31(2): 173-6. doi: 10.1111/j.1524-4725.2005.31040. PMID: 15762210.
- Denadai R, Saad-Hossne R, Todelo AP, Kirylko L, Souto LR. Low-fidelity bench models for basic surgical skills training during undergraduate medical education. Rev Col Bras Cir. 2014; 41(2): 137-45. English, Portuguese. doi: 10.1590/s0100-69912014000200012. PMID: 24918729.
- Trost LB, Bailin PL. History of Mohs surgery. Dermatol Clin. 2011; 29(2): 135-9. vii. doi: 10.1016/j.det.2011.01.010. PMID: 21421139.
- Laranjeira FF, Nunes AGP, Oliveira HM, Machado G, Moreira LF, Corleta OC. Fatores prognósticos de recidiva no carcinoma basocelular da face. 35 Jornada Sul Brasileira de Cirurgia plástica. Rev. Bras. Cir. Plást. [Internet]. 2019 2021; 34(1): 37-39. Disponível em: http://www.rbcp.org.br/details/2376/ptBR/fatores-prognosticos-de-recidiva-no-carcinoma-basocelular-daface.
- Wells Gregory L. MD, Ada West Dermatology and Dermatopathology Revisado/Corrigido. 2022. https://www.msdmanuals.com/pt-br/profissional/dist%C3%BArbios-dermatol%C3%B3gicos/c%C3%A2ncer-de-pele/carcinoma-de-c%C3%A9lulas-escamosas.
- Baile WF, Buckman R, Lenzi R, Glober G, Beale EA, Kudelka AP. SPIKES-A six-step protocol for delivering bad news: application to the patient with cancer. Oncologist. 2000; 5(4): 302-11. doi: 10.1634/theoncologist.5-4-302. PMID: 10964998.
- Amin MB, Greene FL, Edge SB, Compton CC, Gershenwald JE, Brookland RK, Meyer L, Gress DM, Byrd DR, Winchester DP. The Eighth Edition AJCC Cancer Staging Manual: Continuing to build a bridge from a population-based to a more “personalized” approach to cancer staging. CA Cancer J Clin. 2017; 67(2): 93-99. doi: 10.3322/caac.21388. Epub 2017 Jan 17. PMID: 28094848.
- Speight PM, Khurram SA, Kujan O. Oral potentially malignant disorders: risk of progression to malignancy. Oral Surg Oral Med Oral Pathol Oral Radiol. 2018; 125(6): 612-627. doi: 10.1016/j.oooo.2017.12.011. Epub 2017 Dec 29. PMID: 29396319.
- Müller S. Oral lichenoid lesions: distinguishing the benign from the deadly. Mod Pathol. 2017; 30(s1): S54-S67. doi: 10.1038/modpathol.2016.121. PMID: 28060366.
- Marks R, Rennie G, Selwood TS. Malignant transformation of solar keratoses to squamous cell carcinoma. Lancet. 1988; 1: 795-797.
- Pires FR, Barreto ME, Nunes JG, Carneiro NS, Azevedo AB, Dos Santos TC. Oral potentially malignant disorders: clinicalpathological study of 684 cases diagnosed in a Brazilian population. Med Oral Patol Oral Cir Bucal. 2020 Jan 1; 25(1): e84-e88. doi: 10.4317/medoral.23197. PMID: 31880285; PMCID: PMC6982984.
- Slootweg PJ, El-Naggar AK. World Health Organization 4th edition of head and neck tumor classification: insight into the consequential modifications. Virchows Arch. 2018; 472(3): 311-313. doi: 10.1007/s00428-018-2320-6. Epub 2018 Feb 15. PMID: 29450648.
- van der Waal I. Potentially malignant disorders of the oral and oropharyngeal mucosa; terminology, classification and present concepts of management. Oral Oncol. 2009; 45(4-5): 317-23. doi: 10.1016/j.oraloncology.2008.05.016. Epub 2008 Jul 31. PMID: 18674954.
- Dadgostar A, Bigder M, Punjani N, Lozo S, Chahal V, Kavanagh A. Does preoperative depression predict post-operative surgical pain: A systematic review. Int J Surg. 2017; 41: 162-173. doi: 10.1016/j.ijsu.2017.03.061. Epub 2017 Mar 27. PMID: 28359955.
- Rather LJ. Disturbance of function (functio laesa): the legendary fifth cardinal sign of inflammation, added by Galen to the four cardinal signs of Celsus. Bull N Y Acad Med. 1971; 47(3): 303-22. PMID: 5276838; PMCID: PMC1749862.