
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Seborrheic keratosis, solar lentigo and syringoma: A case report of this uncommon collision tumor
El Boukili Hafsa1*; Douhi Zakia1; Soughi Meryem1; Elloudi Sara1; Baybay Hanane1; Mouna Rimani2 ; Mernissi Fatima Zahra1
1Department of Dermatology and Venerology, University Hospital Hassan II, Fez, Morocco.
2Hassan Anatomical Pathology Center, Rabat, Morocco.
*Corresponding Author : El Boukili Hafsa
Department of Dermatology and Venerology,
University Hospital Hassan II, Fez, Morocco.
Email: hafsaboukili@gmail.com
Received : Jan 24, 2024
Accepted : Feb 09, 2024
Published : Feb 16, 2024
Archived : www.jcimcr.org
Copyright : © Hafsa EB (2024).
Abstract
When two or more distinct tumors occur in a single lesion, at one site, it is termed a collision or contiguous tumors, they are often an unexpected finding and may represent a diagnostic challenge, as clinical and histological presentations do not always coincide. Various combinations of collision tumors have been described: We present an unusual case involving a solar lentigo, seborrheic keratosis; and a clinicallyinapparent syringoma, which, to the best of our knowledge, is the first report of this combination.
Keywords: Collision tumor; Syringoma; Seborrheic keratosis; Solar lentigo.
Citation: Hafsa EB, Zakia D, Meryem S, Sara E, Hanane B, et al. Seborrheic keratosis, solar lentigo and syringoma: A case report of this uncommon collision tumor. J Clin Images Med Case Rep. 2024; 5(2): 2863.
Introduction
Cutaneous skin collision with two or more distinct cell populations are rare but well documented, and may pose a diagnostic challenge to clinicians and pathologists. Diagnosis of a collision tumor may be an accidental and unexpected histological finding. Many combinations of collision tumors have been described, with the most frequently reported being the combination of nevus and Basal Cell Carcinoma (BCC). A melanocytic tumor in collision with a benign or malignant epithelial neoplasm is less commonly documented. Some collision tumors involve melanomas, most frequently in combination with a BCC [1] even more exceptional is the involvement of an adnexal tumor in a collision tumor. Syringomas are relatively common benign tumors that originate in the sweat glands, the most familiar clinical presentation of which is the presence of multiple lesions on the eyelids. They present clinically as 1 to 5 mm yellowish, rounded or flat-topped dermal papules [2].
Case presentation
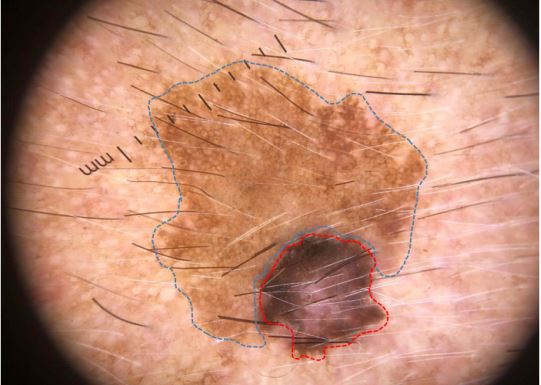
A multimorbid patient in his 80s; presented with long-standing pigmented lesion on his left temple that had been progressive for several years, he reported occupational exposure to the sun and presented skin phototype VI. Clinical findings temporally to the left, adjacent to the auricular region, an asymmetric, heterochromous pigmented lesion, partially slightly elevated on palpation, with a maximum diameter of approximately 15*10 mm (Figure 1). There were no other skin lesions and no palpable locoregional lymph nodes.
Dermoscopic study revealed an asymmetric pigmented lesion with 3 different colors (light brown, dark brown and black). A large part of the lesion showed faint structureless pigmented homogenous network with numerous openings of hair follicle Ostia and adnexal structures; close to which in the periphery there were an asymmetrical dark brown and black network with amorphous area (Figure 2). The clinical impression was of lentigo solar with melanoma and a punch biopsy was performed to confirm the diagnosis. Histological study of the surgical specimen revealed 3 distinct histological components types of lesion in continuity: First there were epidermal acanthosis with infundibular cysts, second, epidermal hyperplasia with elongated rete ridges with Basal layer hyperpigmentation. In the upper and middle dermis there were clusters of small ducts, occasionally with comma-shaped extensions, lined by a double-layered epithelium typical of a syringoma; and there were no signs of malignancy within the limits of the sample communicated (Figure 3).
Based on these findings, a diagnosis of collision tumor (lentigo solar and seborrheic keratosis with syringoma) was established.

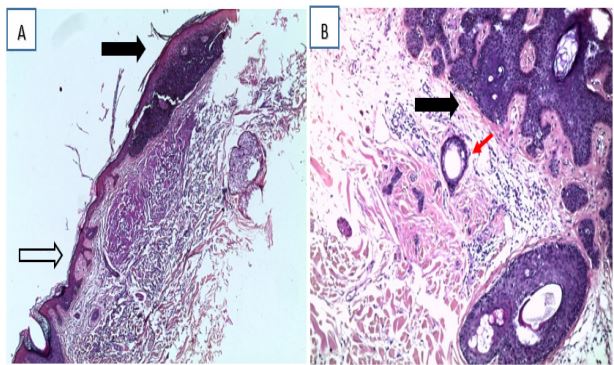
A: Histologic section showing the association between seborrheic keratosis and solar lentigo (H&E x100).
B: Histologic section showing the association between seborrheic keratosis and syringoma (In the superficial dermis, a proliferation of ductal structures embedded in fibrotic stroma is seen. Some of the ducts have comma-like tails) (H&E x100).
Discussion
The human skin is made up of several layers containing different types of cells comprising melanocytic, epithelial, dermal or adnexal [1]. Any kind of intrinsic or extrinsic stimulation can contribute to the likelihood of having two or many unrelated skin lesions occurring adjacent and contiguous with each other, which may lead to various combinations of development of various skin tumors, both benign and malignant: Collision tumors or combination tumors are terms used to refer to this association in time and space [3]. However, the exact etiology of these tumors has not yet been clearly clarified [4] undoubtedly, they are increasingly found in the ageing population with higher cumulative lifetime UV exposure [1]. The clinical diagnosis in these cases is usually extremely difficult, particularly if one of the lesions is pigmented. The development of dermoscopy has helped to improve diagnostic accuracy, as it incorporates a series of distinctive dermoscopic features that, in this case presented here, the blackened portion of the lesion showed criteria suspicious for melanoma whose absence was eliminated by histological analysis. To date, a few cases of collision tumors involving a syringoma have been reported in association with intradermal nevi, BCCs, epidermal cyst, Spitz nevus and melanoma in-situ [5-9]. In our patient, the syringoma was not clinically apparent and there were no syringomas in other facial areas. The three components were close but separated, indicating a collision tumor. Reactive eccrine gland ductal proliferation has been reported in a variety of inflammatory skin diseases (e.g. scarring alopecia) and benign and malignant neoplasms. Guitart et al. proposed the term of ‘syringomatous dermatitis’ for those cases of reactive hyperplastic response of the eccrine duct resulting from an inflammatory skin reaction [10]. In our case we found sclerotic dermal changes in the area of the syringoma, the ducts were located in the middle dermis and some presented with typical comma-shaped structures. These findings, along with the absence of a previous inflammatory cutaneous process, are distinguishable from reactive eccrine gland ductal proliferation and confirm the diagnosis of a syringoma.
Conclusion
CSLs consist of a heterogeneous group of lesions of varying cell types. They manifest a complex morphology making it challenging to diagnose correctly.
We report the first case of a collision tumor involving a syringoma, KS and solar lentigo. Syringomas are common, but their association with other types of tumor is rare. Histopathology staining were very helpful in distinguishing between the three components. Complete excision biopsies are necessary to establish the diagnosis of collision tumors, and long-term follow up is recommended.
References
- Blum A, Siggs G, & Marghoob A. Collision skin lesions-results of a multicenter study of the International Dermoscopy Society (IDS). Dermatology Practical & Conceptual. 2017; 7(4): 51-62. doi: 10.5826/dpc.0704a12.
- Ciarloni L, Frouin E, Bodin F, & Cribier B. Syringoma: A clinicopathological study of 244 cases. Annales de Dermatologie et de Vénéréologie. 2016; 143(8-9): 521-528. doi: 10.1016/j.annder.2015.06.025.
- Fernández-Canedo I, Blázquez N, de Troya M, & Pérez-Salguero T. Collision Tumor Detected by Dermoscopy. Actas Dermo-Sifiliográficas (English Edition). 2009; 100(7): 617-619. doi:10.1016/s1578-2190(09)70133-7.
- Sterz H, Kendler M, Simon JC, & Ziemer M. Maligner Kollisionstumor der Haut. Der Pathologe. 2019. doi:10.1007/s00292-019-0622-3.
- Piana S, Ragazzi M, Zalaudek I, Argenziano G. A curious serendipitous finding: Spitz naevus combined with a syringoma. Australas J Dermatol. 2013; 54: 64-6.
- Spitz DF, Stadecker MJ, Grande DJ. Subclinical syringoma.7. Stefanato CM, Simkin DA, Bhawan J. An unusual melanocytic lesion associated with eccrine duct fibroadenomatosis and syringoid features. Am J Dermatopathol. 2001; 23: 139-42.
- Zhu WY. Vulvar syringoma associated with epidermal cyst. Int J Dermatol. 1989; 28: 142-3.
- Umbert-Millet P, Quintana-Codina M, & Salleras-Redonnet M. Melanoma in situ and syringoma: a rare collision tumor. Clinicalpathological report of a case. Anais Brasileiros de Dermatologia. 2017; 92(5-1): 101-103. doi:10.1590/abd1806-4841.20176324.
- Guitart J, Rosenbaum MM, Requena L. ‘Eruptive syringoma’: a misnomer for a reactive eccrine gland ductal proliferation. J Cutan Pathol. 2003; 30: 202 205.