
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Research Article - Open Access, Volume 5
In vitro susceptibility of fosfomycin in uropathogens with emerging resistance in enterococcus isolates
*Corresponding Author : Sulmaz Reshi
Department of Microbiology, Sher-I-Kashmir
Institute of Medical Sciences, Srinagar, Jammu and
Kashmir, India.
Email: [email protected]
Received : Jan 25, 2024
Accepted : Feb 12, 2024
Published : Feb 19, 2024
Archived : www.jcimcr.org
Copyright : © Reshi S (2024).
Abstract
Introduction: Urinary tract infection is a very common clinical entity and are the leading causes of nosocomial infections. The options for antibiotics especially for nosocomial infections are very limited. Fosfomycin a good drug to be used in UTI and is recommend as first line agents for acute uncomplicated UTIs. The emergence of resistance to fosfomycin is a concern. Limited resistance data for fosfomycin is available from India. This study was conducted in order to monitor the trends of resistance to Fosfomycin in E coli and Enterococcus faecalis causing UTI.
Methods: Urine samples received in the laboratory from all patients were included in the study. Microscopy of uncentrifuged urine sample was done. Culture and sensitivity was done as per the CLSI guidelines. Susceptibility testing of the isolates to Fosfomycin was performed interpretation done as per CLSI.
Results: 150 isolates were taken for the study which included 100 isolates of E.Coli and 50 isolates of Enterococcus faecalis. None of the E. coli isolates were resistant to Fosfomycin and 82.00% of the isolates were found to be sensitive to Nitrofurantoin. None of the Enterococcus faecalis isolates were resistant to Linezolid. The percentage susceptibility was 52% and 70% for Nitrofurantoin and Fosfomycin respectively
Conclusion: The increasing resistance to fosfomycin is a matter of concern. An increased fosfomycin resistance rate in E. faecalis was observed. Performing antimicrobial susceptibility testing should be the most important criteria before starting the antibiotic to avoid undue usage and more such studies need to be conducted.
Keywords: Antimicrobial resistance; Antimicrobial susceptibility testing; Nosocomial infections; Uropathogens.
Citation: Reshi S. In vitro susceptibility of fosfomycin in uropathogens with emerging resistance in enterococcus isolates. J Clin Images Med Case Rep. 2024; 5(2): 2868.
Introduction
Urinary tract infection is a very common clinical entity, it includes both community acquired and hospital acquired urinary tract infections. UTIs are one of the leading causes of nosocomial infections [1]. Majority of the patients having community acquired UTI take over the counter antibiotics. This has led to an increased antimicrobial resistance globally. Rational antibiotic usage as per the culture and sensitivity testing is the need of the hour. Studying the etiological agents as well as their antimicrobial sensitivity patterns is important to formulate an effective antimicrobial policy. Amongst the bacterial causes of urinary tract infections, the commonest of the urological pathogens is E. Colix [2]. The IDSA (Infectious Diseases Society of America) guidelines as well as the ESCMID (European Society for Clinical Microbiology and Infectious Diseases) recommend the use of fosfomycin, nitrofurantoin and Trimethoprim-Sulfamethoxazole (TMP-SMX) as first line agents for acute uncomplicated UTIs. Fluoroquinolones, amoxicillin-clavulunate and other β-lactams ought to be reserved as a second-line agent [3].
The options for antibiotics especially for nosocomial infections are very limited due to the higher prevalence of Extended Spectrum Beta-Lactamases (ESBLs) and even Carbapenem-Resistant Enterobacteriaceae (CREs) in urological pathogens [4].
Many studies recommend the use of fosfomycin for uncomplicated UTI. Fosfomycin has a broad spectrum of action and an excellent bactericidal activity against both Gram negative as well as Gram-positive organisms. It is not metabolized but excreted unchanged in the urine by glomerular filtration, it attains a higher urinary concentration for more than 72 hours, this allows the single dose regimen for the treatment of uncomplicated UTI. It is a safe drug with literally no drug interaction, in addition, it reduces the adherence of bacteria to uroepithelium. Use of fosfomycin is safe for patients with renal and hepatic impairment and no dosage adjustments are required in elderly patients and in pregnancy [3,5]. These reasons make fosfomycin a good drug to be used in UTI but the increasing resistance is a matter of concern that needs to be looked upon and should be given only to those patients where antibiotic therapy is indicated to avoid the undue usage of fosfomycin. The guidelines for performing antimicrobial susceptibility testing for determination in vitro sensitivity of Gram negative and gram-positive bacteria to fosfomycin given by CLSI and EUCAST include agar dilution, broth dilution, disk diffusion and E test techniques [6]. As per CLSI, disk diffusion and MIC breakpoints apply only to E coli and Enterococcus faecalis urinary isolates only and these should not be extrapolated to other species of Enterobacteriaceae [7].
Fosfomycin acts by inhibiting the synthesis of bacterial cell wall at a step prior to that inhibited by beta lactams. The mechanism of bacterial resistance to fosfomycin commonly involves either a chromosome-associated defective transport system or less commonly plasmid-mediated fosfomycin-inactivating enzymes and MurA mutations [8].
The emergence of resistance to fosfomycin is a reasonable concern when evaluating Fosfomycin for clinical use. Limited resistance data for Fosfomycin is available from India. This study was conducted in order to monitor the trends of resistance to Fosfomycin in E coli and Enterococcus faecalis causing UTI.
Aim of the study: The aim of this study was to evaluate the in vitro Fosfomycin activity against uropathogenic E. coli and Enterococcus faecalis isolated from patients in a tertiary care hospital in New Delhi.
Material and methods
This study was conducted in the department of Microbiology, Govind Ballabh Pant Institute of Medical Education and Research (GIPMER), New Delhi. The study was conducted over a period of 4 months. Ethical clearance was obtained from institutional ethics committee. Reference no F.1/IEC/MAMC /96/02/2023/ No. 362. Urine samples received in the Microbiology lab from all OPD and IPD patients were included in the study. The first isolate of each species from each patient was included in the study. The samples included in our study were processed strictly anonymously. Samples were processed immediately when received. Direct microscopy of the uncentrifuged urine sample was done to look for pus cells and bacteria. Culture was done as per the standard technique and were plated by semi-quantitative culture method on 5% sheep blood agar and MacConkey`s agar. Plates were incubated at 37°C for 18 to 24 hours. The growth of organisms and colony count was noted. The isolates obtained from the samples with significant bacteriuria of ≥105 CFU/ml with supportive clinical signs and symptoms suggestive of UTI, history of UTI and/or the presence of significant pus cells on direct microscopy were processed further.
The isolates were identified using conventional biochemical tests and/or by VITEK 2 automated system (bioMerieux, Marcy l’Etoile, France) system. Duplicate isolates of the same pathogen from the same patient were not included in the study. Antimicrobial susceptibility testing was performed on MuellerHinton agar plate using Kirby-Bauer disc diffusion method and/ or by VITEK 2 automated system and results were interpreted according to the Clinical and Laboratory Standards Institute guidelines. The different antimicrobial agents that were tested included both Gram negative panel and Gram-positive panel. The gram-negative panel included ampicillin (25 µg), norfloxacin (10 µg), ciprofloxacin (5 µg), gentamicin (10 µg), ceftriaxone (30 µg), trimethoprim/sulphamethoxazole (1.25/23.75 µg), amikacin (30 µg), nitrofurantoin (300 µg), piperacillin-tazobactam (100/10 µg), imipenem (30 µg), meropenem (30 µg) and fosfomycin (200 µg). The gram-positive panel included Ampicillin (25 µg), ciprofloxacin (5 µg), Norfloxacin (10 µg), levofloxacin (5 µg), high level gentamicin (120 µg), vancomycin (30 µg), teicoplanin (30 µg), linezolid (30 µg), nitrofurantoin (300 µg) and fosfomycin (disc as well as E strip).
Commercially available Fosfomycin discs (200 μg) containing 50 μg of glucose-6-phosphate were used (HiMedia Laboratories) and fosfomycin E-strips containing fosfomycin (0.064 mcg/ ml to 1024 mcg/ml) and supplemented with glucose-6-phosphate (HiMedia Laboratory Pvt Limited) were used. Commercially available Mueller-Hinton agar (HiMedia Laboratories) was used as testing media. The inoculated plates were incubated in ambient air at 37°C for 18 to 24 hours. E. coli ATCC 25922 and Enterococcus faecalis ATCC 29212 were used as control strains.
Susceptibility testing of the isolates to Fosfomycin was performed by the disc diffusion method followed by E-strip, zone of inhibition and MIC was interpreted using CLSI M100 31st edition, breakpoints of fosfomycin for urinary isolates.
Results of disc diffusion using 200 µg fosfomycin disk containing 50 µg of glucose-6- phosphate are interpreted according to the following criteria:
a) Zone diameter ≥16 mm means a susceptible strain.
b) Zone diameter 13-15 mm means an intermediate strain.
c) Zone diameter ≤12 mm means a resistant strain.
The MIC values were interpreted according to the following criteria: [7].
a) MIC ≤64 mg/ml: Susceptible (S).
b) MIC 128 mg/ml: Intermediate (I).
c) MIC ≥256 mg/ml: Resistant (R).
Statistical analysis: Statistical analysis was done using GraphPad software. P value of <0.05 was considered statistically significant.
Table 1: Profile of organisms causing UTI amongst Culture positive samples (n=399).
| Gram negative organism (235 ) | Gram positive organism (108) | Fungal pathogens | |||
|---|---|---|---|---|---|
| Organism | n(%) | Organism | n(%) | Organism | n(%) |
| E coli | 110 (27.56%) | Enterococcus spp | 89 (22.30%) | Candida spp | 55 (13.79) |
| Klebsiella pneumonia | 80 (20.05 %) | MSSA | 12 (3.00 %) | ||
| Pseudomonas aeruginosa | 27(6.76 %) | MRSA | 07(1.75 %) | ||
| Proteus spp | 11 (2.75%) | ||||
| Citrobacter spp | 06 (1.50%) | ||||
| Acinetobacter baumanii | 02 (0.50%) | ||||
| Total | 236(59.14%) | Total | 108 (27.07%) | Total | 55 (13.79%) |
Table 2: In vitro activities of antimicrobial agents against E. coli and Enterococcus faecalis isolated from urine speci- mens. Drug Tested: No. 100 (%) of Isolates.
|
Susceptibility E. coli (N = 100) |
F0 | NIT | COT | NX | CIP | GEN | AK | NET | AMP | A/S | AMC | CTR | CPM | PIT | MRP | IMP | ETP |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Susceptible | 100 | 82 | 34 | 10 | 16 | 47 | 48 | 52 | 9 | 27 | 22 | 18 | 26 | 53 | 72 | 68 | 67 |
| Resistant | 0 | 18 | 66 | 90 | 84 | 53 | 52 | 48 | 91 | 73 | 78 | 82 | 74 | 57 | 28 | 32 | 33 |
Abrevations: Fo: Fosfomycin; NIT: Nitrofurantoin; Cot: Trimethoprim/Sulphamthoxazole; NX: Norfloxacin; Cip: (Ciprofloxa- cin); Gen: Gentamicin; Ak: Amikacin; Net: Netilmycin; Amp: Ampicilin; A/S: Ampicillin/Sulbactam, AMC: Amoxicillin /Clavu- linic Acid; CTR: Ceftriaxone; CPM: Cefepime; PIT: Piperacillin/Tazobactam; MRP: Meropenem; IMP: Imipenem; ETP: Ertap- enem.
Table 3: In vitro activities of antimicrobial agents against enterococcus faecalis isolated from urine specimens. Drug Tested: No. of Isolates 50(%).
|
Susceptibility Enterococcus faecalis ( N= 50 ) |
Fo | Nit | Amp | HLG | NX | CIP | TE | VA | TEI | LZ |
|---|---|---|---|---|---|---|---|---|---|---|
| Susceptible | 35(70%) | 26(52%) | 14(28%) | 11(22%) | 6(12%) | 7(14%) | 8(16%) | 41(82%) | 43(86%) | 50(100%) |
| Resistant | 15(30%) | 24(48%) | 36(72%) | 39(78%) | 44(88%) | 43(86%) | 42(84%) | 09(18%) | 07(14%) | 0(0.0%) |
Abbrevations: Fo: Fosfomycin; Nit: Nitrofurantoin; Amp: Mampicilin; HLG: High Level Gentamicin; NX: Norfloxacin; Cip: Ciprofloxa- cin; TE: Tetracycline; VA: Vancomycin; TEI: Teicoplanin; LZ: Linezolid.
Table 4: Minimum Inhibitory Concentration (MIC) distribution and susceptibility rates of fosfomycin by gradient testing (E strip) method against 150 isolates (100 E. Coli and 50 Enterococcus faecalis).
| Organism | n | MIC distribution of fosfomycin (mg/L) | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ≤0.5 | 0.75 | 1 | 1.5 | 2 | 4 | 8 | 16 | 32 | 48 | 64 | 128 | 256 | 512 | 768 | 1024 | MIC50 (mg/L) |
MIC90 (mg/L) |
%R | ||
| E coli | 100 | 12 | 8 | 57 | 10 | 13 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 2 | 0% |
| E faecalis | 50 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 8 | 13 | 13 | 0 | 5 | 2 | 6 | 2 | 64 | 768 | 30% |
Table 5:Breakup of antimicrobial susceptibility of Enterococci faecalis for fosfomycin susceptible and resistant isolates.
| Fosfomycin n=50 | Statistical analysis | |||||
|---|---|---|---|---|---|---|
| Sensitive; N=35 | Resistant; N=15 | P value | Significance | |||
| Antibiotics | S (N) | R (N) | S (N) | R(N) | ||
| Nit | 26 | 09 | 0 | 15 | 0.0001 | Significant |
| Amp | 15 | 20 | 0 | 15 | 0.0071 | Significant |
| HLG | 11 | 24 | 0 | 15 | 0.0370 | Significant |
| Cip | 07 | 19 | 0 | 15 | 0.0757 | Not significant |
| Tetra | 08 | 27 | 0 | 15 | 0.1097 | Not significant |
| Vanco | 34 | 01 | 7 | 8 | 0.0001 | Significant |
| Teico | 34 | 01 | 9 | 6 | 0.0025 | Significant |
| Linezolid | 35 | 00 | 15 | 0 | 1.000 | Not Significant |
Results
A total of 2101 urine samples were received for culture and sensitivity during the study period (4 months). Of them 1702 (1702/2101; 81.00%) were culture negative with no growth or growth ≤105 CFU/ml. 399 (399/2101; 18.99%) were culture positive with bacteriuria ≥105 CFU/ml. This included 236 gram negative bacilli, 108 gram positive cocci and 55 candida species. Out of the 236 gram negative organisms, 110 were identified as E.Coli, 80 as Klebsiella pneumoniae, 27 as Pseudomonas aeruginosa, 11 as Proteus spp, 6 as Citrobacter spp, and 02 as Acinetobacter baumannii. Among gram positives 89 as Enterococcus spp (50 Enterococcus faecalis and 39 Enterococcus faecium), 12 as MSSA, and 07 as MRSA.
Isolates identified as E Coli and Enterococcus faecalis were only included in study. Other organisms were excluded from the study due to the lack of CLSI guidelines for fosfomycin susceptibility. A total of 150 isolates were taken for the study which included 100 isolates of E.Coli and 50 isolates of Enterococcus faecalis. The sensitivity for the isolates was performed by manual disk diffusion method and/or by VITEK -2 systems.
Multidrug resistance was defined as resistance to at least one agent in three or more antimicrobial groups.
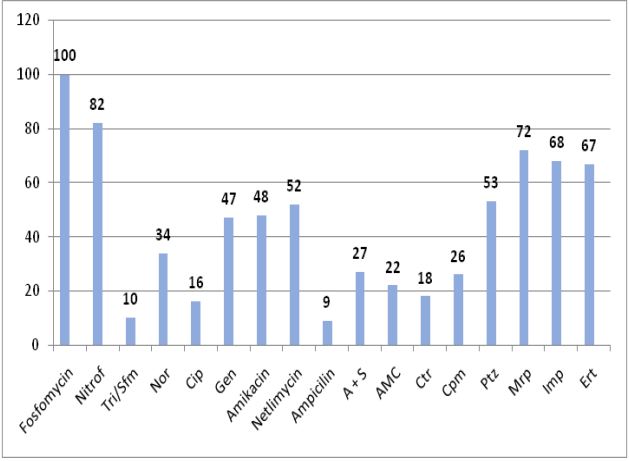
None of the E. coli isolates were resistant to Fosfomycin and 82.00 % of the isolates were found to be sensitive to Nitrofurantoin. The percentage susceptibility was 34%, 10%, 16%, 47%, 48%, 52%, 9%, 27%, 22%, 18%, 26%, 53%, 72%, 68% and 67% respectively for Trimethoprim/Sulphamethoxazole, Norfloxacin, Ciprofloxacin, Gentamicin, Amikacin, Netilmycin, Ampicilin, Ampicilin Sulbactam, Amoxacillin Clavunate, Ceftrixaone, Cefepime, Piperacilin tazobactam, Meropenem, Imipenem and ertapenem.
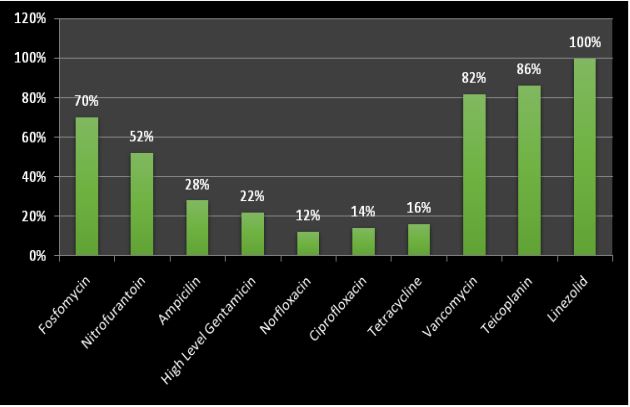
None of the Enterococcus faecalis isolates were resistant to Linezolid. 86% isolates were susceptible to Teicoplanin and 82% of the isolates were found to be sensitive to Vancomycin. The percentage susceptibility was 16%, 14%, 12%, 22%, 28%, 52 % and 70% respectively for Tetracycline, Ciprofloxacin, Norfloxacin, high level gentamicin, Ampicilin, Nitrofurantoin and Fosfomycin.
Discussion
Out of total patients attending outdoor and indoor departments of GB Pant hospital with symptoms suggestive of UTI, 18.99% (399/2101), had culture positivity, which is close to other studies. A study by G. Chooramani, et al. in 2020 recorded positivity of 16.9% [2]. In our study, the most predominant isolated organism was Escherichia coli as is seen in other studies too [1,2,3]. The main finding of the present study is that fosfomycin demonstrated a remarkable antimicrobial activity against all the tested Escherichia Coli isolated from urine, all the isolates were sensitive to fosfomycin (100%). This finding is in concordance with the study by Maraki et al., M Diez-Aguilar et al. and Kumar D et al. they also observed 100% susceptibility of E. coli to fosfomycin [1,9,10]. Behra et al. demonstrated a susceptibility of 99%, Greeshma Hareendranath, also demonstrated promising sensitivity against MDR E. coli, as high as 98% of the E. coli isolates were sensitive to fosfomycin [11,12]. We observed a relatively higher resistance to most of the routinely used antimicrobials against uropathogenic E. coli. This could be because of irrational use of antibiotics with inadequate dosage and duration [2]. The commonly used antibiotics like ampicillin, cotrimoxazole and norfloxacin are mostly resistant, there is a considerable increase in resistance to ceftriaxone and ciprofloxacin also. About (82/100) (82%) and (84/100) (84%) isolates were resistant to ceftriaxone and ciprofloxacin respectively, this is in concordance to many other studies published in and outside India [1,10,11,13].
In theour study Nitrofurantoin, the age-old urinary antibiotic has also shown an effective susceptibility rate. Out of the 100 E. coli isolated 82 (82%) were sensitive to nitrofurantoin. The study by Maraki et al., G. Chooramani et al. and Zhanel GG et al. have also shown a considerable susceptibility rate of E. coli isolates to nitrofurantoin [1-3].
In our study all the MDR strains of E. coli showed 100 % sensitivity to fosfomycin, the antibacterial activity of fosfomycin against uropathogenic E. coli, supports the findings of many other studies on % sensitivity of Fosfomycin to E coli [1,13]. However, in contrast to our study, some studies have reported resistance to fosfomycin in E coli is increasing. These are alarming rates of fosfomycin resistance have been reported in uropathogens in many countries across the world. Studies in China by Li et al. in 2015 found that 7.8% of nonduplicate E. coli clinical isolates collected from 20 geographically dispersed hospitals from July 2009 to June 2010 were nonsusceptible to fosfomycin (MIC. 64 mg per liter) [14]. Similarly in a study by Oteo et al. across twenty-seven Spanish hospitals the overall rate of fosfomycin resistance in E.coli was 9.1%, (5.6% to 15.3%) [15]. They have attributed this increased resistance to the higher prevalence of fosA3 gene which is concurrent with higher transferability of fosA3- harbouring plasmids, this results in further transmission of resistance [14,15].
Fosfomycin susceptibility also depends on the consumption of the antibiotic. A changing trend with the varied result has been reported overtime in places where its consumption rate is high. In a study conducted in Spain showed an increase in resistance (15.3%,) among E. coli urinary isolates where the consumption rate was up to 50% [17]. Enterococcus species are the leading cause of healthcare associated infections. UTI caused by Enterococcus spp account for about 5% in community acquired UTI and about 30% in hospital acquired UTI including catheter associated UTI. In our study we found the prevalence of UTI due to Enterococcus spp is 22.3 (89/399). Our findings are similar to finings of Abbott et al. and Kraszewska et al. [18,19]. We found a remarkable higher resistance to fosfomycin against the tested Enterococcus isolates, (15/50) i.e. 30% resistance and (35/50) i.e. 70% sensitivity. This could be explained by the fact that ours is a super-speciality institute wherein the patients are being referred from other hospitals and have either already taken antibiotics or are on antibiotics at the time of admission. Similar to our study, fosfomycin sensitivity against Enterococci, including VRE strains, varied in the available studies, ranged from 30% to 100% for Enterococcus spp, with some of the studies reporting sensitivity as low as 30% [6,8,18]. This trend of increase in antibiotic resistance to fosfomycin seen in Enterococcus spp could be because of its increasing usage after its revival owing to its minimal side effects and single daily dosage regimen. Similar to our study this increasing antibiotics resistance in uropathognic Enterococcus have also been seen across other countries as well [6,8,9,18].
In the present study the MIC of fosfomycin for Enterococcus faecalis was higher compared to the reported rates in previous other studies. We reported MIC 50/90 of 64/768 for the isolates of Enterococcus tested, while as MIC 50/90 of 32/64 µg/ml was reported by George G. Zhanel et al. and Abbott et al. also noted higher MIC distributions and found MIC50/90 of 64 / 128 µg/ml for E. faecalis [3,18]. Not many studies have been done in India depicting the MIC of Enterococcus faecalis in urinary isolates, so more studies need to be done to have a better understanding.
Nitrofurantoin also showed an increased resistance 48% (24/50) in Enterococcus species. Linda B Ou et al. have also reported reduced susceptibility rate of for nitrofurantoin [5].
The level of resistance to oral antibiotics including fosfomycin and nitrofurantoin in Enterococcus spp although increasing but still these two antibiotics are considered to be better options among the available oral medications, and can still be used in the treatment of UTI, as these are urinary specific antibiotics, but fosfomycin should be used cautiously and should be reserved only for those patients in which other 1st line antibiotics are resistant or contraindicated in order to avoid development of resistance to fosfomycin, to avoid such situation extrapolation of our findings should be done cautiously [1,7,9,17]. None of the Enterococcus faecalis isolates were resistant to Linezolid, this is as per the findings of most of the studies on urinary isolates of Enterococcus including those of Linda B Ou, Chakraborty A et al. [5,20]. While as a study from chennai by Alexander Kiruthiga et al. report sensitivity of only 68.5% to linezolid [21]. The resistance to norfloxacin, ciprofloxacin, tetracycline, High level gentamicin and ampicilin was 88%, 86%, 84%, 78% and 72% respectively. Similar kind of antimicrobial resistance pattern is also noted by Segupatta M et al. and Sharif et al. in their study [22,23]. Emergence of resistance to many regularly used antibiotics can be attributed to their irrational use and to the ease of availability of antibiotics over the counter, moreover in our situation the patients have also been on antibiotics as being referred from other settings.
86% of isolates were susceptible to Teicoplanin and 82% of the isolates were found to be sensitive to Vancomycin. Segupatta M et al. and Sharifi et al. also found 18.6% resistance in vancomycin [22,23]. In our study resistance to fosfomycin did not seem to be associated with vancomycin or teicoplanin resistance as out of 15 fosfomycin resistant isolates, (8/15) were vancomycin resistant and (7/15) were fosfomycin sensitive. And for teicoplanin out of 15 resistant fosfomycin isolates (9/15) were sensitive to teicoplanin and (6/15) were resistant to teicoplanin and statistical analysis also shows fosfomycin resistance was not related to vancomycin or teicoplanin resistance. This finding is in contrast with the findings of F. Allerberger and I. Klare et al. in their study they found Fosfomycin inhibited 97, 94 and 96% of the VR strains tested although MICs of fosfomycin for most of VR isolates were in the intermediate range. However in our study out of 8 vancomycin resistant isolates only 1 was found to be sensitive to fosfomycin [24].
Fosfomycin is used to treat both the susceptible as well as multidrug resistant bacteria. Its mechanism of action is by inhibiting the synthesis of bacterial cell wall at a step prior to that inhibited by beta lactams. Fosfomycin enters the bacterium through membrane channels/transporters and inhibits MurA, which initiates Peptidoglycan (PG) biosynthesis of the bacterial cell wall.
The mechanism of bacterial resistance to fosfomycin commonly involves either a chromosome-associated defective transport system or less commonly plasmid-mediated fosfomycin-inactivating enzymes and MurA mutations. Two important key transporter systems, GlpT and UhpT, mediate the entry of fosfomycin into bacterial cells. Once mutations in the chromosomal glpT and uhpT genes occur, there is reduction in permeability which confers resistance to fosfomycin. Several bacteria display inherent resistance to fosfomycin mainly through MurA mutations. The murA gene mutants exhibit lower affinity for fosfomycin, conferring various degrees of drug resistance. Moreover, fosfomycin-modifying enzymes, coded by the plasmid gene including FosA, FosB, FosC and FosX catalyze the inactivation of fosfomycin. Out of these four only FosB is produced by Gram-positive bacteria. Hence in Enterococcus spp FosB is responsible for the resistance mechanism [3,8].
In India surveillance studies to find out the genotypic mechanism of resistance in Enterococcus are needed to be undertaken as the plasmid mediated resistance is emerging worldwide and is most worrisome [3]. In other countries like China the plasmid mediated resistance to fosfomycin, both in E.Coli and Enterococcus specially in VRE is on rise and this resistance is conferred by fosB and fosB3 has already put a significant burden in healthcare settings [14]. Although our results convey that fosfomycin is the most reliable oral option for treating urinary tract infections due to multidrug-resistant uropathogens but it should be reserved for those where other oral options are resistant or cannot be given as the use of this drug is associated with the development of resistance.
Limitations of the study: There is concern that increased use of this drug is associated with increased resistance [5], however in our study, history of previous exposure to fosfomycin couldnot be taken in all the patients as the records of previous treatment taken were unavailable with patients. Moreover in our present study we have seen the resistance to fosfomycin only by phenotypic tests, genotypic studies to know the gene responsible for the resistance could have been done. To our knowledge, this study is one of the very few studies done from North India to test fosfomycin susceptibility against several multidrug-resistant uropathogens including Enterococcus faecalis from patients with UTIs, however more such studies are needed to know rate of developing resistance to fosfomycin in urinary isolates.
Conclusion
Fosfomycin a good drug to be used in UTI but the increasing resistance is a matter of concern that needs to be looked upon and should be given only to those patients where antibiotic therapy is indicated to avoid the undue usage of fosfomycin and performing antimicrobial susceptibility testing should be the most important criteria before starting the antibiotic. An increased fosfomycin resistance rate in E. faecalis was observed in our present study whereas the susceptibility rate was 100% in urinary isolates of Escherichia coli. Studies on the susceptibility rate of Enterococcus faecalis against fosfomycin are very limited in India, more studies need to be done to know the detailed information on susceptibility rates of Enterococcus species.
Conflicts of interest: None.
References
- Maraki S, Samonis G, Rafailidis PI, Vouloumanou EK, Mavromanolakis E, Falagas ME. Susceptibility of urinary tract bacteria to fosfomycin. Antimicrob Agents Chemother. 2009; 53(10): 4508-4510.
- Chooramani G, Jain B, Chauhan PS. Prevalence and antimicrobial sensitivity pattern of bacteria causing urinary tract infection; study of a tertiary care hospital in North India. Clinical Epidemiology and Global Health. 2022; 8: 890-893.
- Zhanel GG, Walkty AJ, Karlowsky JA. Fosfomycin: A First-Line Oral Therapy for Acute Uncomplicated Cystitis. Can J Infect Dis Med Microbiol. 2016; 2016: 2082693. doi: 10.1155/2016/2082693. Epub 2016 May 10. PMID: 27366158; PMCID: PMC4904571.
- Aprile A, Scalia G, Stefani S, Mezzatesta ML. In vitro fosfomycin study on concordance of susceptibility testing methods against ESBL and carbapenem-resistant Enterobacteriaceae. J Glob Antimicrob Resist. 2020; 23: 286-289.
- Ou LB, Nadeau L. Fosfomycin Susceptibility in Multidrug-Resistant Enterobacteriaceae Species and Vancomycin-Resistant Enterococci Urinary Isolates. Can J Hosp Pharm. 2017; 70(5): 368-374.
- Falagas ME, Vouloumanou EK, Samonis G, Vardakas KZ. Fosfomycin. Clin Microbiol Rev. 2016; 29(2): 321-347.
- M100 Performance Standards for Antimicrobial Susceptibility Testing. 31: 45-75.
- Michalopoulos AS, Livaditis IG, Gougoutas V. The revival of fosfomycin. Int J Infect Dis. 2011; 15(11): 732-739.
- Diez-Aguilar M, Canton R. New microbiological aspects of fosfomycin. Rev Esp Quimioter. 2019; 321(l1): 8-18.
- Kumar D, Das A, Purbey MK, Gupta N, Nath G. Susceptibility of uropathogenic multidrug-resistant Escherichia coli to Fosfomycin. J Acad Clin Microbiol. 2017; 19: 101-104.
- Behera B, Mohanty S, Sahu S, Praharaj AK. In vitro Activity of Fosfomycin against Multidrug-Resistant Urinary and Nonurinary Gram-Negative Isolates. Indian J Crit Care Med. 2018; 22(7): 533-536. doi: 10.4103/ijccm.IJCCM_67_18. PMID: 30111930; PMCID: PMC6069321.
- Hareendranath G, Mukundan A, Kunjappan SP. Fosfomycin susceptibility in multidrug resistant urinary Escherichia coli isolates. J Evolution Med Dent Sci 2021; 10(07): 414- 418, DOI: 10.14260/jemds/2021/92.
- Batra P, Abrol AK, Gupta S, Pushpan P, Kumar R. Susceptibility pattern of oral antimicrobials in uncomplicated UTI: Does fosfomycin still stand effective? J Family Med Prim Care 2020; 9: 850-3.
- Silver LL. Fosfomycin: Mechanism and Resistance. Cold Spring Harb Perspect Med. 2017; 7(2): 025262. doi: 10.1101/cshperspect.a025262. PMID: 28062557; PMCID: PMC5287057.
- Oteo J, Bautista V, Lara N, Cuevas O, Arroyo M, Fernández S, Lázaro E, de Abajo FJ, Campos J; Spanish ESBL-EARS-Net Study Group. Parallel increase in community use of fosfomycin and resistance to fosfomycin in extended-spectrum beta-lactamase (ESBL)-producing Escherichia coli. J Antimicrob Chemother. 2010; 65(11): 2459-63. doi: 10.1093/jac/dkq346. Epub 2010 Sep 16. PMID: 20851815.
- Ríos E, Del Carmen López Diaz M, Culebras E, Rodríguez-Avial I, Rodríguez-Avial C. Resistance to fosfomycin is increasing and is significantly associated with extended-spectrum β-lactamaseproduction in urinary isolates of Escherichia coli. Med Microbiol Immunol. 2022; 211(5-6): 269-272. doi: 10.1007/s00430-022-00749-2. Epub 2022 Sep 3. PMID: 36056943; PMCID: PMC9618510.
- Fajfr M, Louda M, Paterová P, Ryšková L, Pacovský J, Košina J, Žemličková H, Broďák M. The susceptibility to fosfomycin of Gram-negative bacteria isolates from urinary tract infection in the Czech Republic: data from a unicentric study. BMC Urol. 2017; 17(1): 33.
- Abbott IJ, van Gorp E, van der Meijden A, Wijma RA, Meletiadis J, Roberts JA, Mouton JW, Peleg AY. Oral Fosfomycin Treatment for Enterococcal Urinary Tract Infections in a In Vitro Model. Antimicrob Agents Chemother. 2020; 64(6): 00342-20. doi: 10.1128/AAC.00342-20. PMID: 32253214; PMCID: PMC7269476.
- Kraszewska Z, Skowron K, Kwiecińska-Piróg J, Grudlewska-Buda K, Przekwas J, Wiktorczyk-Kapischke N, Wałecka-Zacharska E, Gospodarek-Komkowska E. Antibiotic Resistance of Enterococcus spp. Isolated from the Urine of Patients Hospitalized in the University Hospital in North-Central Poland, 2016-2021. Antibiotics (Basel). 2022; 11(12): 1749. doi: 10.3390/antibiotics11121749. PMID: 36551406; PMCID: PMC9774570.
- Chakraborty A, Pal NK, Sarkar S, Gupta MS. Antibiotic resistance pattern of Enterococci isolates from nosocomial infections in a tertiary care hospital in Eastern India. J Nat Sci Biol Med. 2015; 6(2): 394-7. doi: 10.4103/0976-9668.160018. PMID: 26283837; PMCID: PMC4518417.
- Kiruthiga, Alexander et al. Fosfomycin Susceptibility among Urinary Enterococcus Faecalis with High Level Aminoglycoside and Glycopeptide Resistant Phenotypes. Indian Journal of Public Health Research & Development. 2019; 970-974: 0976-5506.
- Sharifi et al. Virulence and Antimicrobial Resistance in Enterococci Isolated from Urinary Tract Infections, Advanced Pharmaceutical Bulletin. 2013; 3(1): 197-201.
- M Sengupta et al Excellent fosfomycin and linezolid susceptibility among multidrug resistant urinary Enterococcus isolates in Eastern India, World Journal of Advanced Research and Reviews. 2020; 07(02): 331-335.
- Allerberger F, Klare I. In-vitro activity of fosfomycin against vancomycin-resistant enterococci. J Antimicrob Chemother. 1999; 43(2): 211-7. doi: 10.1093/jac/43.2.211. PMID: 11252326.