
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Concurrent meningioma and schwannoma; An uncommon presentation of common tumors
Shaarif Bashir*; Usman Hassan; Sajid Mushtaq; Asif Loya; Hina Maqbool
Department of Pathology, ShaukatKhanum Memorial Cancer Hospital and Research Centre, Lahore, Pakistan.
*Corresponding Author : Shaarif Bashir
Department of Pathology, ShaukatKhanum Memorial Cancer Hospital and Research Centre, Lahore,
Pakistan.
Tel: +92-3334245144;
Email: shaarifbashir@yahoo.com
Received : Jan 08, 2024
Accepted : Feb 15, 2024
Published : Feb 22, 2024
Archived : www.jcimcr.org
Copyright : © Bashir S (2024).
Abstract
Citation: Bashir S, Hassan U, Mushtaq S, Loya A, Maqbool H. Concurrent meningioma and schwannoma; An uncommon presentation of common tumors. J Clin Images Med Case Rep. 2024; 5(2): 2873.
Introduction
Meningiomas and schwannomas are relatively common tumors of the nervous system, however, concurrent tumors are rare. These concurrent tumors are usually associated with Neurofibromatosis type 2, Von Hippel-Lindau disease and sometimes with radiation therapy [1-3].
Several mechanisms underlying the development of these concurrent tumors have been proposed including metaplastic change and bidirectional differentiation. However, the precise pathogenesis is unknown [4]. Only 9 cases of such concurrent tumors have been reported till date. Here we report a case of a 55 year old male patient presenting with a space occupying lesion at C1/C2 level.
Case presentation
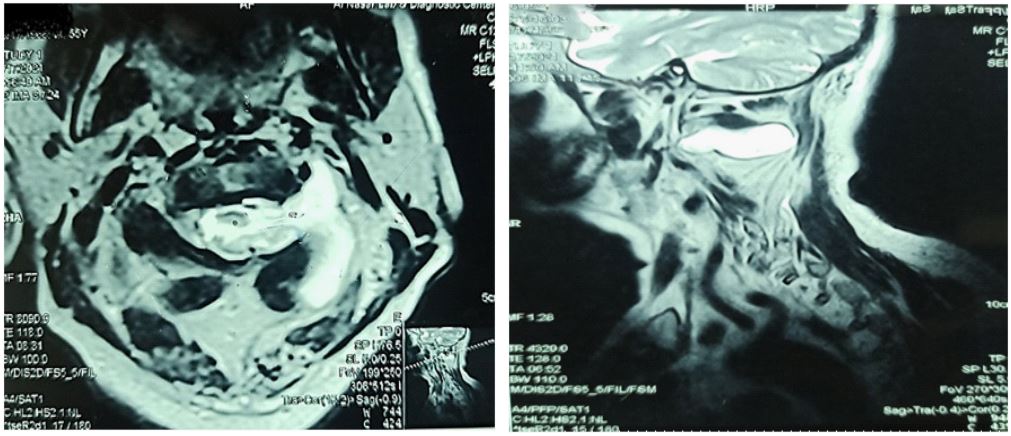
A 55 year old male patient presented with back pain and quadriparesis, which developed gradually over a period of 4 months. On examination, no other nodules or spots were identified suggesting any syndromic association. No family history of Neurofibromatosis or Von Hippel-Lindau disease was present. There was no history of prior radiation therapy. Magnetic resonance imaging revealed a dumbbell shaped space occupying lesion with intradural and extradural components as well as mixed signal intensity (Figure 1). Clinical and radiological differential of neurofibroma was raised. The tumor was removed via C1 C2 laminectomy. Peroperatively, the tumor was attached to dura on one side and C2 nerve root on the other.
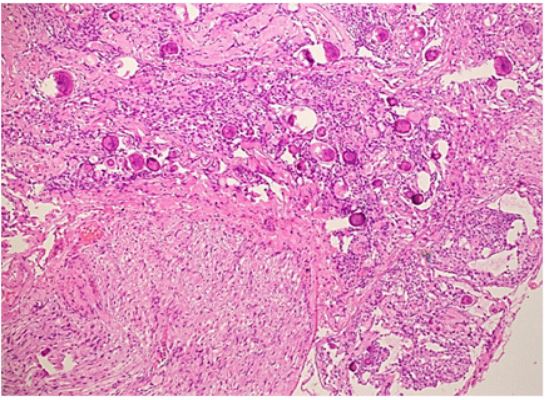
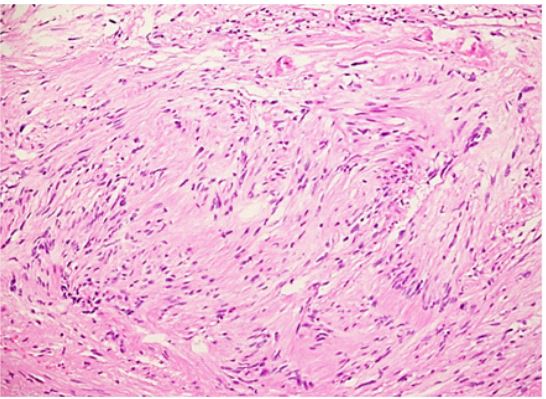
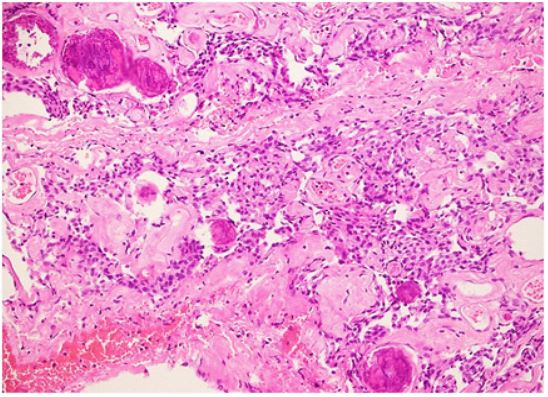
The specimen was sent for histopathological examination to our laboratory and grossly comprised of multiple fragments measuring approximately 2 cm. Sections taken from the tumor revealed a neoplastic proliferation composed of two definite components. First component showed proliferation of spindled to wavy cells arranged in vague hypocellular and hypercellular areas with verocay body formation. The second component showed whorls of meningothelial cells with abundant intercellular collagen and scattered psammoma bodies (Figure 2A, 2B and 2C).
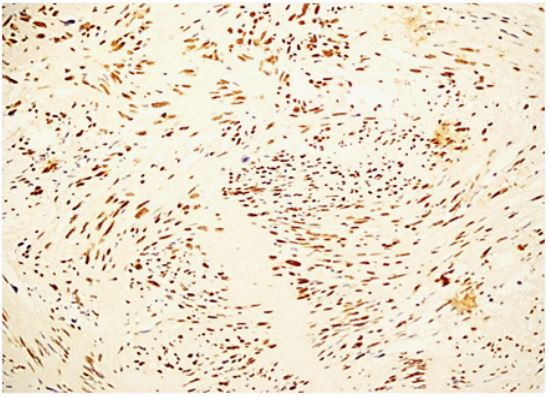
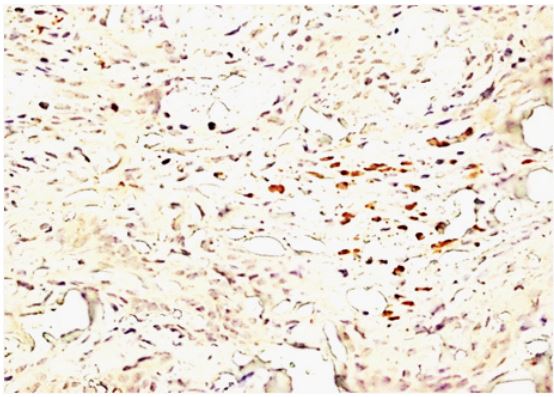
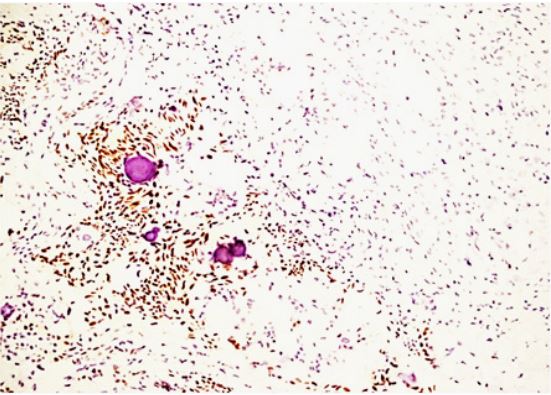
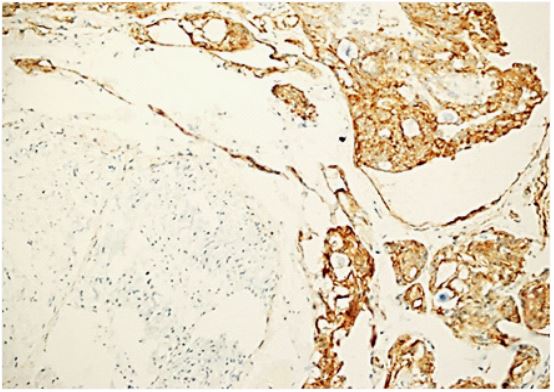
No definite necrosis, mitosis or high grade features were noted in the submitted specimen. Due to rarity of this diagnosis, immunohistochemistry was also performed for confirmation of the diagnosis despite unequivocal histological features. Sox 10, which is a very specific and sensitive marker of neural differentiation showed strong nuclear staining in the schwannoma component (Figures 3A and 3B). EMA and PR bothhighlighted the meningioma componentonly (Figures 4A and 4B). The patient had an uneventful post-operative course.
Discussion
The simultaneous development of two tumors at the same location is very rare and a few cases have been reported at the cerebellopontine angle and cervical spine, mostly in association with Neurofibromatosis (NF) or prior radiation therapy. NF2 is a rare disorder affecting about 1 in 40000 newborns and has a autosomal dominant inheritance [4].
Although unclear, multiple underlying mechanisms have been proposed for this rare occurrence [4,5]. One hypothesis is that meningothelial hyperplasia or reactive meningeal changes develop in the vicinity of a Schwannoma [4,6]. Other proposed mechanisms include collision of two separate tumors, metaplastic change in one original tumor or multi directional differentiation of the same progenitor cell into different neoplastic components [4,7,8]. Schwannomas are neuroectodermal tumors that are assumed to originate from Schwann cells of dorsal nerve roots in the subarachnoid space, hence, forming dumbbell shaped tumors along the nerve roots [4,7,8]. Meningiomas are mesodermal neoplasms that are supposed to arise from the arachnoid membranes and that is why almost 90% are present in an intradural location [4]. Some authors believe that schwannoma and meningioma cells arise from the same mesenchymal cell [8-13]. Another hypothesis involves the exposure of two separate neoplastic cell types at the same location as a result of same oncogenic stimulus, with consequent development as a composite tumor [12-15].
Although, MRI is the best preoperative imaging technique for the evaluation of neurological neoplasms, the differentiation between mixed and composite tumors remains a challenging task because both tumors are homogenously contrast enhancing [15]. Preoperative extensive imaging analysis is fundamental as the surgical treatment approachvaries depending on the type of the tumor [14].
Conclusion
In conclusion, our case had no prior radiological or clinical suspicion of a composite tumor. However, histology alongwith immunohistochemistry was quite convincing. Gross total resection was achieved via laminectomy and patient had an uneventful postsurgical course.
Funding Sources: No funding involved.
Conflicts of interest: Authors declare no conflicts of interest.
References
- Liebelt BD, Haider AS, Steele WJ, Krishna C, Blacklock JB. Spinal schwannoma and meningioma mimicking a single mass at the craniocervical junction subsequent to remote radiation therapy for acne vulgaris.World neurosurgery. 2016; 93: 484-e13.
- Dorizzi A, Crivelli G, Marra A, Scamoni C, Dario A, Bonfanti N, Brianza ML. Associated cervical schwannoma and dorsal meningioma. Case report and review of the literature.Journal of Neurosurgical Sciences. 1992; 36(3): 173-6.
- Rasheed F, Fatima S, Ahmad Z. Triad of Intraspinal Meningioma, Schwannoma, and Ependymoma: Report of an Extremely Rare Case. International journal of surgical pathology. 2016; 24(1): 55-8.
- Nakamizo A, Suzuki SO, Shimogawa T, Amano T, Mizoguchi M, Yoshimoto K, Sasaki T. Concurrent spinal nerve root schwannoma and meningioma mimicking single-component schwannoma. Neuropathology. 2012; 32(2): 190-5.
- Zheng GB, Hong Z, Wang Z. Diagnostic value of MRI in coexistence of schwannoma and meningioma mimicking a single dumbbell-shaped tumor in high cervical level. Case series and literature review. The Journal of Spinal Cord Medicine. 2021; 7: 1-6.
- Geddes JF, Sutcliffe JC, King TT. Mixed cranial nerve tumors in neurofibromatosis type 2. Clinical neuropathology. 1995; 14(6): 310-3.
- Matyja E, Kunert P, Grajkowska W, Marchel A. Coexistence of meningioma and schwannoma in the same cerebellopontine angle in a patients with NF2. Folia Neuropathologica. 2012; 50(2): 166-75.
- Oichi T, Chikuda H, Morikawa T, Mori H, Kitamura D, Higuchi J, Taniguchi Y, Matsubayashi Y, Oshima Y, Tanaka S. Concurrent spinal schwannoma and meningioma mimicking a single cervical dumbbell-shaped tumor: case report. Journal of Neurosurgery: Spine. 2015; 23(6): 784-7.
- Ogihara S, Seichi A, Iwasaki M, Kawaguchi H, Kitagawa T, Tajiri Y, Nakamura K. Concurrent spinal schwannomas and meningiomas: case illustration. Journal of Neurosurgery: Spine. 2003; 98(3): 300
- Verma SK, Kumar S, Deb P, Yadav KK. Rare case of radiologically distinct but pathologically admixed vestibular schwannoma and meningioma in the cerebellopontine angle: A case report. Journal of Cancer Research and Therapeutics. 2015; 11(4): 1029.
- Izci Y, Secer HI, Gönül E, Ongürü O. Simultaneously occurring vestibular schwannoma and meningioma in the cerebellopontine angle: case report and literature review. Clinical neuropathology. 2007; 26(5): 219-23.
- Zhao LY, Jiang YN, Wang YB, Bai Y, Sun Y, Li YQ. Coexistent vestibular schwannoma and meningioma in a patient without neurofibromatosis: A case report and review of literature. World Journal of Clinical Cases. 2021; 9(24): 7251.
- Porčnik A, Žele T, Prestor B. Concurrent intradural meningioma and schwannoma at the same lumbar level in a patient without neurofibromatosis: a case report. British Journal of Neurosurgery. 2020; 34(1): 104-6.
- Suematsu Y, Tsuji O, Nagoshi N, Nori S, Suzuki S, Okada E, Yagi M, Kameyama K, Fujita N, Watanabe K, Nakamura M. Concurrent dorsal subpialschwannoma and ventral meningioma arising at the same upper cervical level: a case report. Spinal Cord Series and Cases. 2020; 6(1): 1-6.
- Moussalem C, Abou-Mrad Z, El Houcheimy M, Amine A, Bsat S, Alomari SO, Tabbarah A, Darwish H. Coexisting schwannoma and meningioma simulating a single cerebellopontine angle lesion: Case report and review of the literature. Interdisciplinary Neurosurgery. 2021; 25: 101169.