
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Report - Open Access, Volume 5
A rare case report of bifid or double uvula in a 45-year-old woman
Vandna Bharti1*; Pratibha Sahoo1; Sanjana Prakash2; Saransh Tyagi2
1Department of Anesthesiology, Assistant Professor, Prasad Institute of Medical Sciences, Lucknow, India.
2Department of Anesthesiology, Junior Resident, Prasad Institute of Medical Sciences, Lucknow, India.
*Corresponding Author : Vandna Bhart
Department of Anesthesiology, Assistant Professor, Prasad Institute of Medical Sciences, Lucknow,
India.
Email: doc.mevanna@gmail.com
Received : Jan 28, 2024
Accepted : Feb 15, 2024
Published : Feb 22, 2024
Archived : www.jcimcr.org
Copyright : © Bharti V (2024).
Abstract
Bifid uvula, a congenital anatomical variation characterized by the splitting of the uvula into two distinct lobes is a relatively uncommon condition in adults and often considered a marker for submucous cleft palate. This case report contributes to the limited body of literature on bifid uvula by describing a unique clinical presentation and highlighting the need for thorough assessment in individuals with this anatomical variation.
Case report: A 45-year-old female presented for pre-anaesthetic check-up for laparoscopic cholecystectomy was found to have bifid uvula. She underwent surgery under general anaesthesia uneventfully.
Conclusion: This case report presents an unusual and intriguing instance of bifid uvula along with a discussion of its clinical significance and requirement of continuous peri-operative vigilance.
Keywords: Bifid uvula; Cleft palate; Velopharyngeal.
Citation: Bharti V, Sahoo P, Prakash S, Tyagi S. A rare case report of bifid or double uvula in a 45-year-old woman. J Clin Images Med Case Rep. 2024; 5(2): 2874.
Introduction
Bifid uvula is an abnormal split or division in the uvula or tissue that hangs down at the end of soft palate in the roof of mouth. Compared to a normal one it has fewer amounts of mucosal tissue. It is commonly noticed in marker for submucous cleft palate. It can be associated with problems of speech, swallowing and recurrent ear infections [1]. A bifid or bifurcated uvula exists in 2% of the white population [2]. Sometimes it may be associated with systemic problems like aneurysms in different vascular beds like coronary, aortic or abdominal but it does not cause problems in view of airway management. Bifid uvula can be a manifestation of a rare disorder known as cornelia de Lange syndrome [3,4]. Cornelia de Lange syndrome is a rare congenital syndrome associated with bifid uvula and sub mucous cleft palate that causes problems in airway due anatomical distortion [4]. It is a congenital anomaly characterized by distinctive facial dysmorphism (arched eyebrows, long eyelashes, small widely spaced teeth and microcephaly), primordial short stature, hirsutism, and upper limb reduction defects that range from subtle phalangeal abnormalities to oligodactyly [5]. This case report presents an unusual and intriguing instance of bifid uvula along with a discussion of its clinical significance.
Case report
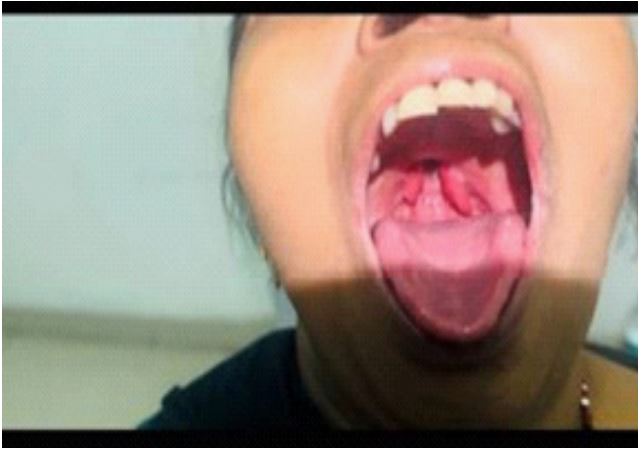
A 45-year-old female weighing 50 kg, presented for pre-anaesthetic check-up for laparoscopic cholecystectomy. She was American Society of Anaesthesiologist’s –Physical status grade 1 and while taking history, nasal tone was noticed in the patient. There was no history of difficulty in swallowing, breathing, pain abdomen. There was no significant family history present. Airway examination was normal except for full bifid uvula and few buck teeth in upper jaw with loose lateral incisors as shown in Figure 1. Ear nose and throat consultation was sought for nasopharyngoscopy examination of pharynx and palate due to its association with submucous cleft palate which was also unremarkable. Her blood reports, ECG and chest X ray were within normal range. She was advised for brain and abdominal imaging because of its rare presentation of aneurysm but the patient refused due to financial constraints. No other clinical features were suggestive of any syndrome. Patient was cleared by the anaesthetist for surgery. She was pre medicated with Tablet Ranitidine 150 mg and Tablet Alprazolam 0.25 mg one night prior to the surgery. Intravenous line was secured using an 18 Gauge cannula. She was induced under stable vitals with inj. Fentanyl 100 microgram, Propofol 100 mg and inj. Vecuronium 4 mg. Cormack-Lehane grade was 1 as shown in Figure 2. Intubation done with cuffed endotracheal tube measuring 7.5 mm internal diameter using videolaryngoscope in single attempt. Anesthesia was maintained with oxygen, nitrous oxide, sevoflurane and injection vecuronium. Her surgery was smooth, without any complications and was extubated with injection Neostigmine 2.5 mg and injection glycopyrrolate 0.4 mg. She was then shifted to post operative recovery room and monitored there for 2 hours.

Discussion
The term bifid uvula means the partial or full bifurcation of the uvula. Submucous cleft palate shows malpositioning of the palate muscles and may result in velopharyngeal insufficiency, inability to form a seal with pharyngeal wall leading to frequent regurgitation, hypernasality etc [4,7]. Bifid uvula can be a warning sign of syndromes with internal anatomical or functional changes without any external manifestation as reported by Samanta. In 2013, a 16-year-old boy with only bifid uvula underwent for retinal surgery with failed awakening and extubation. CT revealed a ruptured aneurysm in the brain, following which immediate craniotomy and clipping were performed as a lifesaving procedure [2]. In the year 2017, Khasbage SD found an incidental bifid uvula in a 58-year-old man along with both of his sons showing familial predisposition [6]. Cornelia de Lange syndrome is a rare congenital syndrome associated with bifid uvula and sub mucous cleft palate that causes problems in airway due anatomical distortion. It may be associated with increased risk of schizophrenia, mild mental retardation, and chromosomal disorder [3,4]. Management may not be challenging in all the cases with bifid uvula but all the patients must be looked for any anatomical variation and features of associated syndromes as they can be easily overlooked.
Conclusion
This case highlights the need for thorough assessment and pre-anaesthetic check-up in individuals with this anatomical variation, continuous peri-operative vigilance. Detailed history of the patient along with complete family history should be taken to rule out any genetic predisposition anaesthetists should be aware of its presence and potential implications of the complications that may arise intra operatively.
Acknowledgement: I would like to acknowledge the contribution made by all the authors in conception, designing and image acquisition of this case.
Consent from patient: Informed consent obtained.
References
- Shprintzen RJ, Schwartz RH, Daniller A, Hoch L. Morphologic significance of bifid uvula. Pediatrics. 1985; 75: 553-61.
- Samanta S, Samanta S. Bifid uvula: Anaesthetists don’t take it lightly. Saudi J Anaesth. 2013; 7: 482-484.
- Vorstman JA, de Ranitz AG, Udink ten Cate FE, Beemer FA, Kahn RS. A bifid uvula in a patient with schizophrenia as a sign of 22q11 deletion syndrome. Ned Tijdschr Geneeskd. 2002; 146: 2033-6.
- Callea M, Montanari M. Bifid uvula and submucous cleft palate in cornelia de lange syndrome. J Int Dent Med Res. 2011; 4: 74.
- Gupta D, Goyal S. Cornelia de-Lange Syndrome. J Indian Soc Pedod Prev Dent. 2005; 23(1): 38-41.
- Khasbage SD. Bifid Uvula in three members of a family. Int J Oral Craniofac Sci. 2017; 3: 017-9.
- Prasad P, Khalil E, Desai VB, Varma SR, Gunasekaran L, Kumar K, Pradeep S. Bifid Uvula—An Enigma. Journal of Pharmacy and Bioallied Sciences. 2023; 15(1): 806-9.