
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Report - Open Access, Volume 5
Spondylodiscitis related to SAPHO syndrome: A spine dilemma?
Maroua Slouma, MD1,3; Wided Lahmar, MD1,3*; Hiba Bettaieb, MD1,3*; Lamjed Msoli, MD2,3; Imen Gharsallah1,3
1Department of Rheumatology, Military Hospital, Tunis, Tunisia.
2Department of Radiology, Military Hospital, Tunis, Tunisia.
3University of Tunis El Manar – Tunisia.
*Corresponding Author : Wided Lahmar
Department of Rheumatology, Military Hospital,
Tunis, Tunisia.
Email: widedlahmar2@gmail.com
Received : Jan 28, 2024
Accepted : Feb 15, 2024
Published : Feb 22, 2024
Archived : www.jcimcr.org
Copyright : © Lahmar W (2024).
Abstract
Background: The diagnosis of spondylodiscitis related to SAPHO syndrome is challenging.
Findings: This is illustrated by the case of a 44-year-old woman with SAPHO syndrome who presented with a two-month history of inflammatory back pain. A spinal MRI revealed spondylodiscitis affecting multiple dorsal levels. Infectious spondylodiscitis was ruled out based on clinical, biological, and imaging features. Zoledronic acid and nonsteroidal anti-inflammatory drugs led to a significant improvement.
Conclusion: Ensuring infection exclusion in spondylodiscitis, even in inflammatory disease contexts, is crucial and zoledronic acid’s efficacy in this condition is noteworthy.
Keywords: SAPHO syndrome; Spondylodiscitis; Zoledronic acid.
Citation: Slouma M, Lahmar W, Bettaieb H, Msoli L. Gharsallah I. Spondylodiscitis related to SAPHO syndrome: A spine dilemma?. J Clin Images Med Case Rep. 2024; 5(2): 2875.
Introduction
Synovitis, Acne, Pustulosis, Hyperostosis, and Osteitis (SAPHO) syndrome is an inflammatory disease characterized by both osteoarticular and dermatological manifestations. The underlying pathogenesis remains unclear, although genetic, infectious, and immunological factors have been suggested [1]. SAPHO syndrome is rare, affecting one among 10,000 Caucasians. Bone involvement, a characteristic feature of SAPHO syndrome, typically affects the anterior chest wall and the axial skeleton. Axial manifestations encompass sacroiliitis and spinal abnormalities, such as vertebral body corner lesions, hyperostosis, and paravertebral ossification [2]. Osteolytic lesions leading to variable degrees of vertebral body collapse resulting in vertebral compression, have been reported [3]. Spinal features include mainly hyperostosis, erosions, sclerotic changes, and syndesmophytes [2,4]. Spondylodiscitis related to SAPHO is scarce and differentiating it from infectious spondylodiscitis is sometimes challenging [4]. Despite its rarity, awareness of this complication is necessary due to its potential to cause spinal cord compression [3]. Herein, we report here a case of SAPHO syndrome with spondylodiscitis. We emphasize clinical manifestations, imaging features, and management of this specific presentation.
Case presentation
A 44-year-old woman with no medical history presented with inflammatory pain affecting the anterior chest wall, left elbow, and the buttock, evolving gradually over 4 months.Physical examination revealed localized tenderness in the left elbow and positive sacroiliac provocative tests. She did not exhibit synovitis or arthritis in the peripheral joints. Spinal examination revealed no abnormalities. Dermatological manifestations were absent. Inflammatory biomarkers were normal. Radiographs showed left elbow osteitis (Figure 1) and right sacroiliitis. Bone scintigraphy demonstrated symmetric uptake in the chondrosternal, manubriosternal, sternoclavicular articulations, left elbow, and right sacroiliac joint. The diagnosis of SAPHO syndrome was established based on clinical, biological, and radiological findings. The patient showed a favorable response to bisphosphonates (60 mg pamidronic acid infusions over three consecutive days) from 2003 to 2009. Subsequently, the patient was lost to followup. Twelve years later, the patient presented with a two-month history of inflammatory back pain. She had a preserved general condition, with no history of fever or weight loss. Physical examination revealed restricted dorsolumbar spine motion and sternoclavicular tenderness. Neurological and pulmonary examinations were normal, with no cutaneous infections detected. Laboratory findings revealed increased levels of C reactive protein (CRP) (34 mg/L, Normal value (N)<6) and erythrocyte sedimentation rate (ESR) (40 mm, N<15 mm). Blood cell counts, liver tests, and renal function were unremarkable. Radiographs of the dorsal spine showed T6, T7, and T8 erosive lesions, sclerotic remodeling of the endplates, disc space narrowing, and T5 and T6 large syndesmophytes extending from the anterior and lateral margins and spinal magnetic resonance imaging (MRI) demonstrated spondylodiscitis from T5 to T9 (Figure 2). Serum levels of calcium, albumin, and phosphorus were within the normal range. Blood cultures, urine analysis, tumor markers, and brucella serodiagnosis were negative. Tuberculosis skin test and chest radiograph were both negative. With no overall health decline, absence of infectious entry sites, and negative investigations, infectious spondylodiscitis was ruled out. The diagnosis of spondylodiscitis related to SAPHO was made based on clinical, biological, and radiological features. The patient was prescribed zoledronic acid (a single dose of 5 mg) and celecoxib (200 mg daily), leading to symptom alleviation and a reduction in CRP levels from 34 mg/L to 8 mg/L (N<6 mg/L).

B: Pelvis radiograph showing left sacroiliitis (arrow).
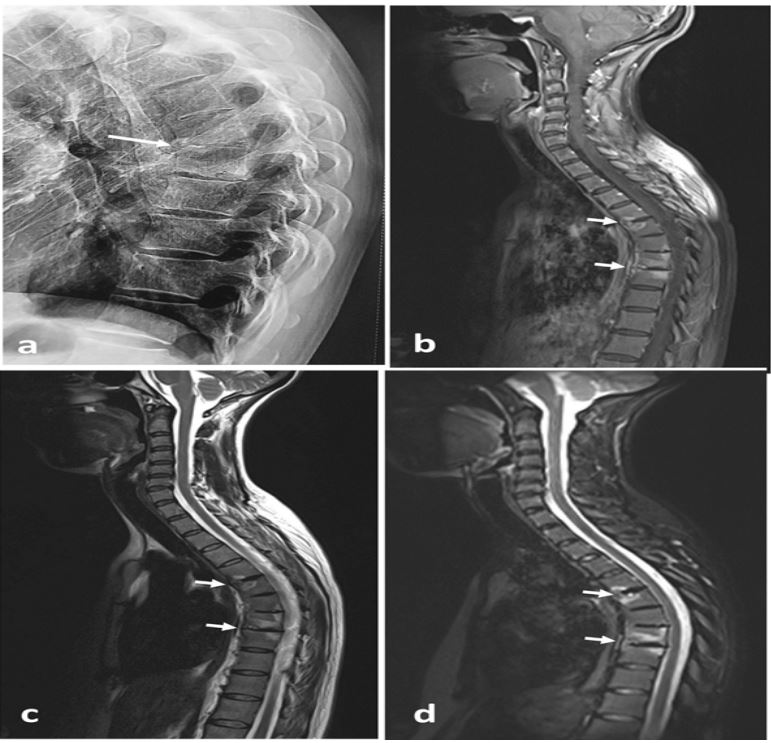
B: Magnetic resonance imaging of the spine (lateral view) T1 FAT SAT weighted post gadolinium sequence showing high T1 signal in the T5/T6 endplates (white arrow) and T7/T8 vertebral body (arrow) and low T1 signal in the T5/T6, T6/T7, T7/T8 and T8/T9 disks.
C: Magnetic resonance imaging of the spine (lateral view) T2 weighted sequence showing high T2 signal in the T5/T6 endplates and T7/T8 vertebral body and low T2 signal in the T5/T6, T6/T7, T7/T8 and T8/T9 disks.
D: Magnetic resonance imaging of the spine (lateral view) weighted sequences showing an increasing of T2 signal in the T5/T6 endplates and T7/T8 vertebral body after fat saturation.
Discussion
We report a case of SAPHO-related spondylodiscitis. Axial skeleton manifestations are frequently reported in patients with SAPHO (70-90%) [5]. The spine is the second most commonly affected site after the anterior chest wall [4]. Nonetheless, spondylodiscitis related to SAPHO syndrome is rare. It can manifest as an initial presentation or develop during the disease, as seen in our case. This condition may cause inflammatory back pain, kyphosis, or neurological manifestations [6]. Its diagnosis is challenging since imaging features can mimic infectious spondylodiscitis. In SAPHO syndrome, involvement of two or more adjacent vertebrae may occur in 30% of cases [7]. Adjacent cortical erosions in the endplates on both sides of an intervertebral disc, underlying subchondral sclerosis in the endplates, and narrowing of the adjacent disc space may be taken for an early disk space infection [5]. In these cases, the absence of both fluidlike signal intensity on T2-weighted signal and disc space enhancement on gadolinium-enhanced T1-weighted images strongly suggests SAPHO-related spondylodiscitis. Nevertheless, some cases (up to 30%) may exhibit disc space involvement with high T2-weighted signal and gadolinium enhancement, complicating differentiation from infectious spondylodiscitis [2,8]. MRI allows specifying the extent of the surrounding bone marrow edema which may be localized on the endplate erosions or diffuse [8]. The diagnosis of SAPHO syndrome can be established based on clinical presentation like non-erosive synovitis, bone pain, palmoplantar pustulosis and severe nodular acne, biological findings, and imaging features such as hyperostosis, sclerotic lesions or osteolysis. However, the diagnosis remains difficult in several situations leading to the consideration of a disco vertebral biopsy. This latter can reveal chronic sterile nonspecific inflammation [4]. It’s worth mentioning that spondylodiscitis related to SAPHO can even be life-threatening. Indeed, it can be responsible for spinal cord compression [3]. During SAPHO syndrome, around 63.5% of patients exhibit palmar and plantar pustulosis and acne [6]. However, 15% of adults never display skin involvement [1]. In this case, the absence of skin manifestations compounded the challenge in diagnosing SAPHO-associated spondylodiscitis. As of now, there are no standardized treatment protocols for the management of SAPHO syndrome. It mainly depends on the clinical manifestations of the disease [9]. Nonsteroidal anti-inflammatory drugs are suggested as first-line therapy for patients with axial involvement, and bisphosphonates are mainly recommended for patients with predominant bone lesions. Treatment for sterile spondylodiscitis is not specific and hinges on controlling the underlying disease activity. Surgery should be considered in cases with complications such as spinal cord compression or severe kyphosis [10]. Accordingly, our patient received nonsteroidal anti-inflammatory drugs and bisphosphonates with spectacular evolution.
Conclusion
This case highlights a challenging spondylodiscitis presentation in SAPHO syndrome patient, emphasizing the need for MRI to differentiate from tumors or infectious spondylodiscitis. Hence, a greater awareness of the radiological features of spine involvement related to SAPHO syndrome is highly required.
Ethical consideration: Informed consent was obtained and signed from the patient regarding the use of patient health information for the purposes of writing a case report publication.
References
- Nguyen MT, Borchers A, Selmi C, Naguwa SM, Cheema G, Gershwin ME. The SAPHO Syndrome. Seminars in Arthritis and Rheumatism. 2012; 42(3): 254-65.
- Leone A, Cassar-Pullicino VN, Casale R, Magarelli N, Semprini A, Colosimo C. The SAPHO syndrome revisited with an emphasis on spinal manifestations. Skeletal Radiol. 2015; 44(1): 9-24.
- Rekik S, Slouma M, Sahli ̇ H, Cheour E, Elleuch M. Spinal Cord ̇Compression: An Infrequent Complication of SAPHO Syndrome. Arch Rheumatol. 2015; 30(3): 247-52.
- Toussirot E, Dupond JL, Wendling D. Spondylodiscitis in SAPHO syndrome. A series of eight cases. Annals of the Rheumatic Diseases. 1997; 56(1): 52-8.
- Laredo JD, Vuillemin-Bodaghi V, Boutry N, Cotten A, Parlier-Cuau C. SAPHO Syndrome: MR Appearance of Vertebral Involvement. Radiology. 2007; 242(3): 825- 31.
- Govoni M, Colina M, Massara A, Trotta F. “SAPHO syndrome and infections”. Autoimmunity Reviews. 2009 ; 8(3): 256-9.
- Parlier-Cuau C, Laredo J. [Vertebral involvement in SAPHO syndrome]. J Radiol. 2010; 91(9 Pt 2): 1068-78.
- Nachtigal A, Cardinal E, Bureau NJ, Sainte-Marie LG, Milette F. Vertebral involvement in SAPHO syndrome: MRI findings. Skeletal Radiol. 1999; 28(3): 163-8.
- Slouma M, Bettaieb H, Rahmouni S, Litaiem N, Dhahri R, Gharsallah I, et al. Pharmacological Management of Synovitis, Acne, Pustulosis, Hyperostosis, and Osteitis Syndrome Syndrome: A Proposal of a Treatment Algorithm. JCR: Journal of Clinical Rheumatology. 2022; 28(2): 545.
- Takigawa T, Tanaka M, Nakahara S, Sugimoto Y, Ozaki T. SAPHO syndrome with rapidly progressing destructive spondylitis: two cases treated surgically. Eur Spine J. 2008; 17: 331-7.