
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Multiple high intensity transient signals in a polycythemia vera patient with hemorrhagic infarction: A case report
Jeanie Allen Marie I Beltran*; Laurence Kristoffer J Batino; Jose C Navarro
Department of Neurology, Jose R. Reyes Memorial Medical Center, Manila, Philippines.
*Corresponding Author : Beltran JAMI
Department of Neurology, Jose R. Reyes Memorial Medical Center, Manila, Philippines.
Email: jibeltran.sbcm@gmail.com
Received : Feb 01, 2024
Accepted : Feb 16, 2024
Published : Feb 23, 2024
Archived : www.jcimcr.org
Copyright : © Beltran JAMI (2024).
Abstract
Polycythemia vera is a chronic myeloproliferative disorder characterized by the overproduction of red blood cells, white blood cells, and platelets. Thrombotic complications are common in polycythemia vera; however, hemorrhagic infarction is a rare but potentially life-threatening complication. This case report describes a 48-year-old male who presented with headache, left hemiparesis, and numbness. Neuroimaging revealed acute cerebral infarction with hemorrhagic conversion. Hematologic investigations showed a viscous blood panel and a diagnosis of PV was confirmed with genetic testing. This case aims to show the presence of multiple embolic signals in a transcranial Doppler study in a stroke patient with hemorrhagic infarct on the background of polycythemia vera.
Keywords: Polycythemia vera; Hemorrhagic infarction; Transcranial doppler study; Microembolic signals.
Citation: Beltran JAMI, Batino LKJ, Navarro JC. Multiple high intensity transient signals in a polycythemia vera patient with hemorrhagic infarction: A case report. J Clin Images Med Case Rep. 2024; 5(2): 2876.
Introduction
Polycythemia vera is a chronic Myeloproliferative (MPN) disorder characterized by the overproduction of RBCs, WBCs, and platelets. It is caused by a mutation in the JAK2 gene with an estimated prevalence of 95% [1]. Complications such as transformation to myelofibrosis or acute myeloid leukemia may occur. Thrombotic events, such as deep vein thrombosis, stroke, and myocardial infarction, are also frequent complications. In some PV cases, the initial manifestation is an ischemic stroke. In some cases, this ischemic event may be complicated by hemorrhagic transformation. The precise mechanism underlying this event remains unclear with limited published cases. Here, we present a case of a Filipino male with hemorrhagic infarction and subsequently diagnosed with PV.
Case report
A 48-year-old Filipino male presented to the emergency department with a sudden onset right hemicranial headache accompanied by left-sided weakness and numbness. He had a blood pressure of 160/100 mmHg with an NIHSS of [3]. He is a non-smoker, a regular alcoholic beverage drinker, and poorly compliant hypertensive. Initial laboratory investigations revealed erythrocytosis, leukocytosis, and thrombocytosis (Table 1). The prothrombin time activated partial thromboplastin time and international normalized ratio were within the normal range. Lipid profile and HbA1c were also standard. Cranial Computed Tomography (CT) scan (Figure 1a-c) demonstrated hypodensity at the right frontal and parietal areas with central hyperdensity. Cranial Magnetic Resonance Imaging (MRI) (Figure 2a-h) showed acute cerebral infarction at said areas with restricted diffusion and dark blooming signals on Gradient Echo (GRE) sequence at the right parietal region. Cranial Magnetic Resonance Arteriography (MRA) (Figure 2i) showed short segment stenosis at the petrous portion of the right Internal Carotid Artery (ICA), hypoplastic right vertebral artery with Posterior Inferior Cerebellar Artery (PICA) termination, and hypoplastic A1 segment of the right Anterior Cerebral Artery (ACA). Magnetic Resonance Venography (MRV) (Figure 2j-k) revealed standard variant hypoplastic right transverse sinus and right sigmoid sinus. Transcranial Doppler sonography (TCD) disclosed overall average Mean Flow Velocities (MFV) with no evidence of stenosis (Figure 3, Table 2). Microembolic Signal (MES) monitoring by TCD revealed the presence of numerous bilateral HighIntensity Transient Signals (HITS) with a Spencer Grade V (>300 HITS) (Figure 4). Bubble test by TCD did not reveal any right-toleft shunting, and Carotid Doppler studies (CDS) did not show any stenosis. 2D-echocardiogram with Doppler study and 24- hour Holter monitoring also did not reveal any abnormalities. The D-dimer test yielded a negative result, and polycythemia vera was confirmed with JAK2-V617F mutation. Abdominal ultrasound showed splenomegaly. The patient was managed as acute multiple cerebral infarctions in the right frontal area and right parietal area with hemorrhagic conversion (HI 2 type) and intracranial stenosis at the right internal carotid artery. He was also treated for a case of polycythemia vera. Dual antiplatelet therapy (Aspirin 100 mg tablet and Clopidogrel 75 mg tablet once a day) was started. Hydroxyurea therapy was also initiated, and he underwent therapeutic phlebotomy procedures. He was eventually discharged in stable condition with no progression of symptoms. On a 3-month follow-up, he improved with a Modified Rankin Scale (MRS) score of 0. The TCD, MES, and Bubble tests were normal. In comparison with the admission TCD, the repeat TCD showed diffuse elevation of the MFV with the average direction of flow and pulsatility indices (Figure 5, Table 2). Repeat CBC showed normal values (Table 1). He remained stable during subsequent neurology and hematology outpatient follow-up consultations, with no recurrence of vascular complications.
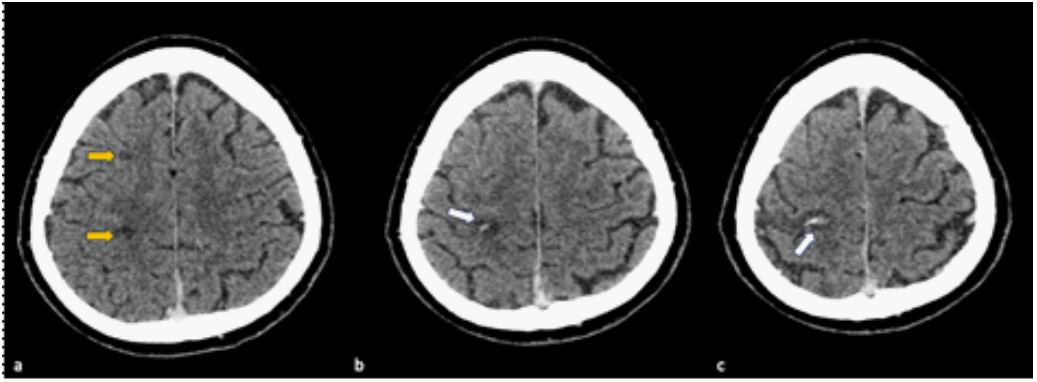
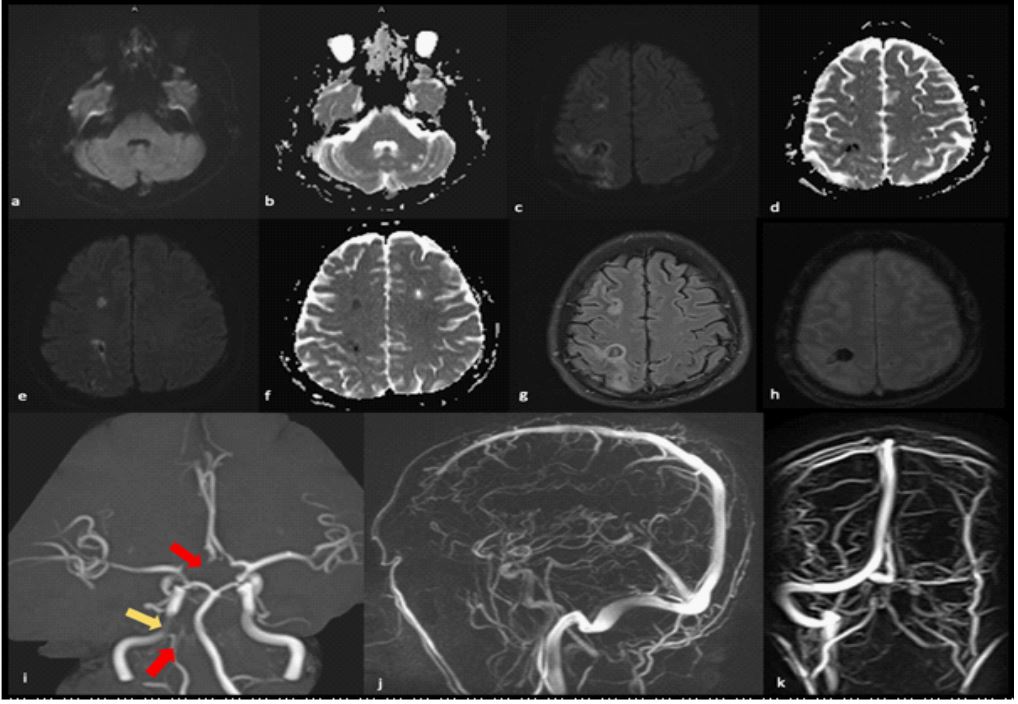
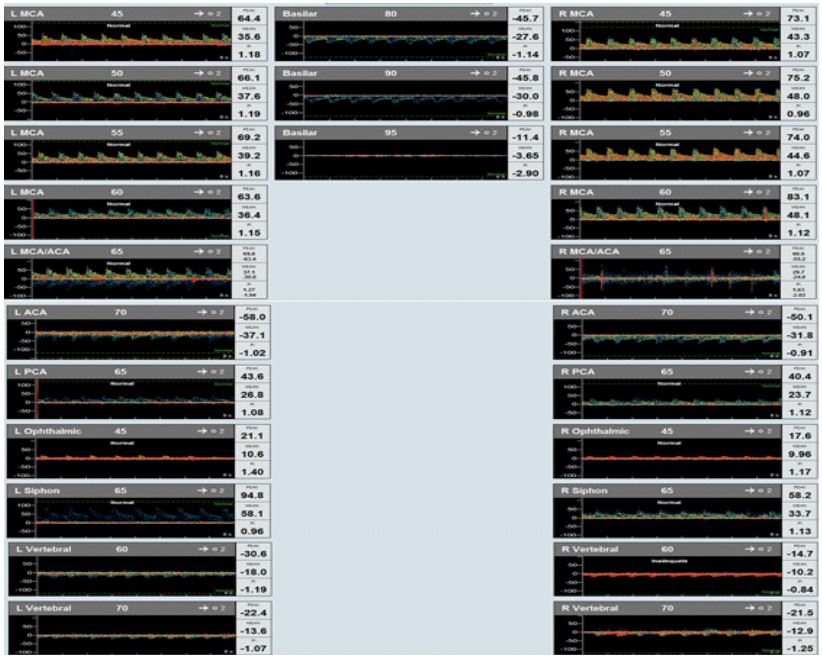
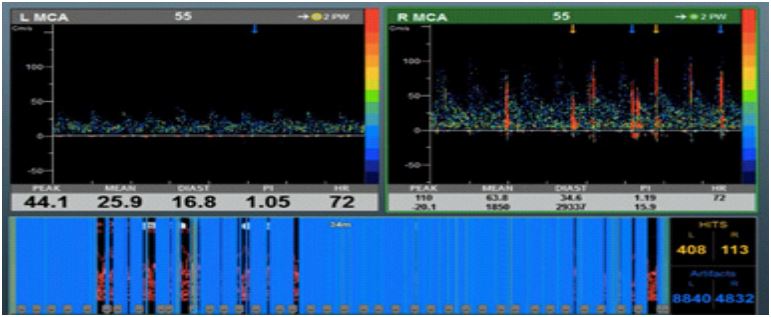
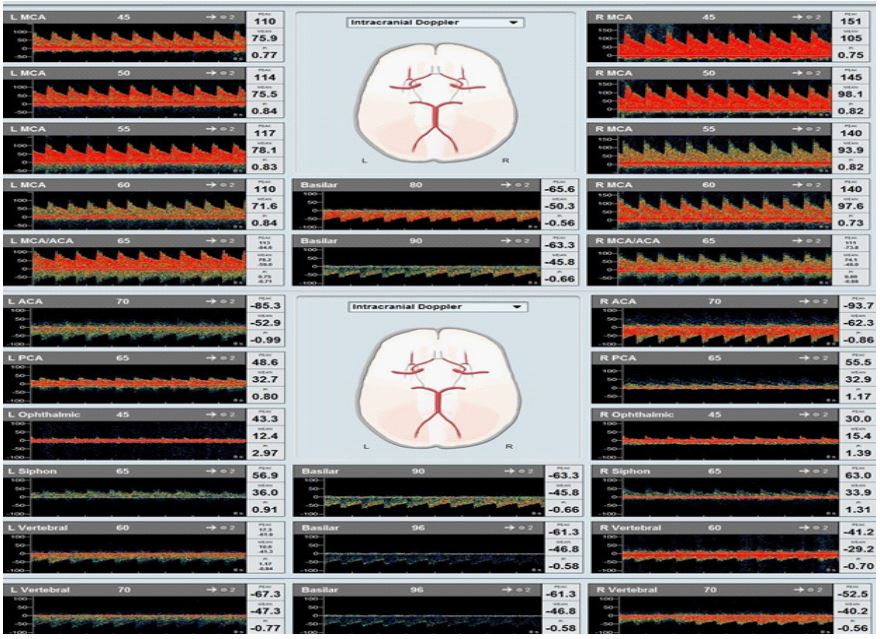
Table 1: Blood count values. Remarkable improvement of blood count values upon follow-up consult compared to baseline values on admission.
| Normal values | Admission | 3-month | |
|---|---|---|---|
| Hemoglobin | 140-170 g/L | 224 | 180 |
| Hematocrit | 0.41-0.51 | 0.68 | 0.52 |
| Red blood cell | 4.5-6 x 1012/L | 9.5 | 6.9 |
| White blood cells | 5.0-10.0 x 109/L | 13 | 9 |
| Platelet | 150-400 x 109/uL | 491 | 327 |
| Interpretation | - | Erythrocytosis, leukocytosis, thrombocytosis | Within normal limits |
Table 2: TCD values.
| TCD | Admission | 3-month follow-up | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Vessel (depth, mm) | MFV (cm/s) | PI | MFV (cm/s) | PI | |||||
| Right | Left | Right | Left | Right | Left | Right | Left | ||
| MCA | 45 | 43.3 | 35.6 | 1.07 | 1.18 | 105 | 75.9 | 0.75 | 0.77 |
| 50 | 48 | 37.6 | 0.96 | 1.19 | 98.1 | 75.5 | 0.82 | 0.84 | |
| 55 | 44.6 | 39.2 | 1.07 | 1.16 | 93.9 | 78.1 | 0.82 | 0.83 | |
| 60 | 48.1 | 36.4 | 1.12 | 1.15 | 97.6 | 71.6 | 0.73 | 0.84 | |
| ACA | -31.8 | -37.1 | -0.91 | -1.02 | -62.3 | -52.9 | 0.86 | -0.99 | |
| OA | 9.96 | 10.6 | 1.17 | 1.40 | 15.4 | 12.4 | 1.39 | 2.97 | |
| CS | 33.7 | 58.1 | 1.13 | 0.96 | 33.9 | 36.0 | 1.31 | 0.91 | |
| PCA | 23.7 | 26.8 | 1.12 | 1.08 | 32.9 | 32.7 | 1.17 | 0.80 | |
| VA | 60 | -10.2 | -18.0 | -0.84 | -1.19 | -29.2 | -41.3 | -0.70 | 0.84 |
| 70 | -12.9 | -13.6 | -1.25 | -1.07 | -40.2 | -47.3 | -0.56 | -0.77 | |
| BA | 80 | -27.6 | -1.14 | - | - | ||||
| 90 | -30.0 | -0.98 | -45.8 | -0.66 | |||||
| 96 | - | - | -46.8 | -0.58 | |||||
|
MCA: Middle Cerebral Artery;
ACA: Anterior Cerebral
Artery; OA: Ophthalmic
Artery; CS: Carotid Siphon;
PCA: Posterior Cerebral
Artery; VA: Vertebral Artery; BA: Basilar Artery; MFV: Mean Flow Velocity; PI: Pulsatility Index. |
|||||||||
Discussion
PV and its association with ischemic stroke have been well documented. In a population-based cohort study, patients had an approximately 3-fold risk of thrombosis at the time of MPN diagnosis, with a 1.5-fold higher risk of ischemic stroke at five years [2]. Hemorrhagic infarction, on the other hand, is rare, and only a few cases have been reported [3,7]. Elevated hematocrit, leukocytes, platelets, increased adhesiveness of RBCs, and a higher burden of the JAK2V617F allele were significant factors in thrombogenesis. In this case report, splenomegaly was also detected; in MPN patients, this correlates to an increased risk of occurrence of thromboembolic event [8]. Multiple territorial infarcts were observed in 35% of MPN cases, with 22% having considerable artery involvement [9]. Studies also suggest that PV might be linked to intracranial stenosis due to endothelial dysfunction resulting from elevated hematocrit levels, which can initiate an inflammatory response similar to atherosclerosis formation. In this case, the stenosis at the petrous portion of the right ICA could account as the embolic source for the acute infarction, but it will not explain the bilateral HITS observed. Cardiac and vascular investigations were unremarkable. Bubble test by TCD to rule out paradoxical embolism through patent foramen ovale, and the Mean Flow Velocities (MFV) of all insonated vessels were average. Repeat TCD showed elevation of MFV on all vessels, which correlated with the normal CBC result. Only a few studies have explored the association of cerebral blood flow and MES by TCD in PV [10,13]. One study reported decreased blood flow velocities with significant improvement after pharmacologic treatment and phlebotomy procedures [10]. Another study reported left MCA stenosis and the occurrence of HITS on the left in a PV patient with left hemispheric stroke. The frequency of HITS was observed to decrease in correlation with clinical improvement and reduction in hematocrit levels, indicating a potential occurrence of spontaneous thrombolysis [11]. In a similar report, significant right intracranial stenosis of the distal ICA and MCA was accompanied by HITS in a recurrent ischemic stroke in the same territory. HITS like wise disappeared after hematocrit reduction but with the persistence of vessel stenosis [12]. These findings provide supporting evidence that PV can contribute to large vessel steno-occlusive disease from hemodynamic compromise and artery-to-artery embolism. In our case, we found numerous bilateral HITS. This is an uncommon finding and is usually associated with cardioembolic stroke and artery-to-artery embolism [13,15]. As mentioned earlier, cardiac, and vascular investigations were unremarkable and there are no other potential sources of microembolic signals. Thus, the HITS detected are unlikely to be attributed to either assumed source. However, there is no direct evidence to substantiate whether these HITS are a characteristic of PV or caused by systemic in-situ thromboembolism.
Conclusion
The case was managed as Embolic Stroke of Undetermined Source (ESUS). A predisposing factor for prothrombotic state of the patient is probably due to its PV which contributed to the formation of microemboli as evidenced by bilateral HITS detection. The exact mechanism of underlying hemorrhagic infarction is still unclear. To the best of our knowledge, this is the only reported case of hemorrhagic infarction showing bilateral microembolic signals in a PV patient in Southeast Asia. We recommend monitoring the cerebral blood flow in patients with PV and expanding the study to include a larger group of PV patients to validate its role in the occurrence of strokes.
Declarations
Financial support: None.
Conflict of interest: None.
References
- Tefferi A, Pardanani A. Evaluation of increased hemoglobin in the JAK2 mutations era: A diagnostic algorithm based on genetic tests. Mayo Clin Proc. 2007; 82: 599-604.
- M. Hultcrantz, M Bjorkholm, PW Dickman, O Landgren, AR Derolf, SY Kristinsson, et al. Risk for arterial and venous thrombosis in patients with myeloproliferative neoplasms; a populationbased cohort study, Ann. Intern. Med. 2018; 168: 317-325,
- Wang N, Liu L, Jiang X, Li D & Chen X. Acute multiple cerebral infarction combined with cerebral microhemorrhage in Polycythemia vera: A case report. Experimental and Therapeutic Medicine.2019; 18: 2949-2955.
- Cao YY, Cao J, Bi ZJ, Xu SB, Liu CC. Hemorrhagic transformation after acute ischemic stroke caused by polycythemia vera: Report of two case. World J Clin Cases. 2021; 9(25): 7551-7557. PMID: 34616825; PMCID: PMC8464450.
- Shao X, Liu Z, Qin C, Xiao F. Acute Myocardial Infarction Followed by Cerebral Hemorrhagic Infarction in Polycythemia Vera: Case Report and Literature Review. Front Cardiovasc Med. 2021; 8: 660999. PMID: 34527707; PMCID: PMC8435622.
- Balagopal K, Mathew A, Koshy AG, Jacob JP. Polycythemia Vera Presenting as Hemorrhagic Stroke. J Neurosci Rural Pract. 2021; 12(3): 601-602. Epub 2021 May 5. PMID: 34295120; PMCID: PMC8289499.
- Inao S, Furuse M, Hotta T, Asai H, Yoshida K, Saso K, Kaneoke Y, Motegi Y. [Hemodilutional therapy in raised intracranial pressure; observations in a case of cerebral infarction associated with polycythemia vera]. No To Shinkei. 1986; 38(3): 219-24. Japanese. PMID: 3707772.
- A Kaifie, M Kirschner, D Wolf, C Maintz, M Hanel, N Gattemann, et al. Bleeding, thrombosis, and anticoagulation in myeloproliferative neoplasm (MPN): analysis from the German SAL-MPNresistry, J. Hematol. Oncol. 2016; 9: 18.
- Nagai K, Shimoyama T, Yamaguchi H, Sakamoto Y, Suda S, Wakita S, Kimura K. Clinical characteristics and brain MRI findings in myeloproliferative neoplasms. Journal of the Neurological Sciences. 2020; 416: 116990.
- Fiermonte G, Aloe Spiriti MA, Latagliata R, Petti MC, Giacomini P. Polycythaemia vera and cerebral blood flow: a preliminary study with transcranial Doppler. J Intern Med. 1993; 234(6): 599-602. PMID: 7903108.
- Del Sette M, Finocchi C, Angeli S, Conti M & Gandolfo C. Transcranial Doppler Detection of Microemboli in a Stroke Patient with Polycythemia rubra vera. Cerebrovascular Diseases.1995; 5(3): 208-211.
- M.F. José. Cardioembolic stroke: an update. Lancet Neurol. 2003; 2: 177-188.
- Segura T, Serena J, Teruel J & Dávalos A. (2000). Cerebral embolism in a patient with polycythemia rubra vera. European Journal of Neurology. 2000; 7(1): 8790.
- H Poppert, S Sadikovic, K Sander, O Wolf, D Sander. Embolic signals in unselected stroke patients. Stroke. 2006; 37: 2039-2043.
- RG Hart, L Catanese, KS Perera, G Ntaios, SJ Connolly. Embolic stroke of undetermined source: a systematic review and clinical update. Stroke. 2017; 48: 867-872.