
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Vulvar squamous cell carcinoma with a fatal outcome
Carolina T Chavesti*; Catarina de Freitasti; Andreia Sofia Basíliot
Sesaram, EPE. Machico Health Centers Grouping, Machico Health Center, Portugal.
*Corresponding Author : Carolina T Chavest
Sesaram, EPE. Machico Health Centers Grouping,
Machico Health Center, Portugal.
Tel: 961 183 987;
Email: carolina.chaves.2@gmail.com
Received : Jan 31, 2024
Accepted : Feb 16, 2024
Published : Feb 23, 2024
Archived : www.jcimcr.org
Copyright : © Chavesti CT (2024).
Abstract
Vulvar cancer is one of the least common forms of gynecologic malignancies. At least 75 percent of vulvar cancer are squamous cell carcinoma, being mainly associated with human papillomavirus infection. Many patients are asymptomatic at the time of diagnosis. However, some have vulvar pruritus or bleeding. Treatment depends on both the extent of the vulvar lesion and the lymph node evaluation. Prognosis data reports five-year survival ranging from 70 to 93 percent for patients with negative nodes, to 25 to 41 percent for those with positive nodes. We report a case of a 53 years old woman presenting with a vulvar lesion with about one year evolution, worsening in the past three weeks with bleeding and purulent discharge. Biopsy of the lesion confirmed a moderately differentiated squamous cell carcinoma, considered Stage IVB. Was proposed upfront chemotherapy with carboplatin and paclitaxel. The patient died fivedays ager the first session of chemotherapy. The present case highlights the importance of longitudinal and regular follow-up in primary care, as the first point of contact to healthcare services and the manager of the patient’s health.
Keywords: Vulvar squamous cell carcinoma; General and family medicine; Chemotherapy.
Citation: Chavesti CT, Freitasti CD, Basílioti AS. Vulvar squamous cell carcinoma with a fatal outcome. J Clin Images Med Case Rep. 2024; 5(2): 2878.
Case description
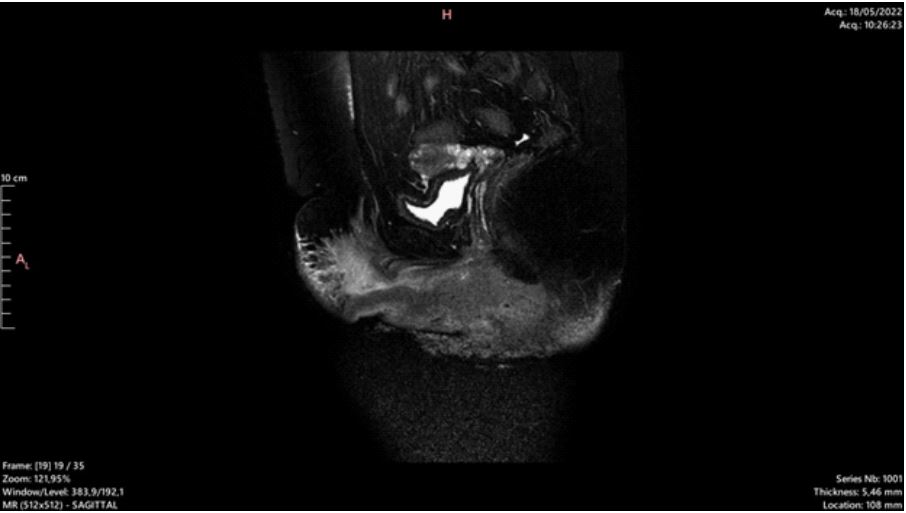
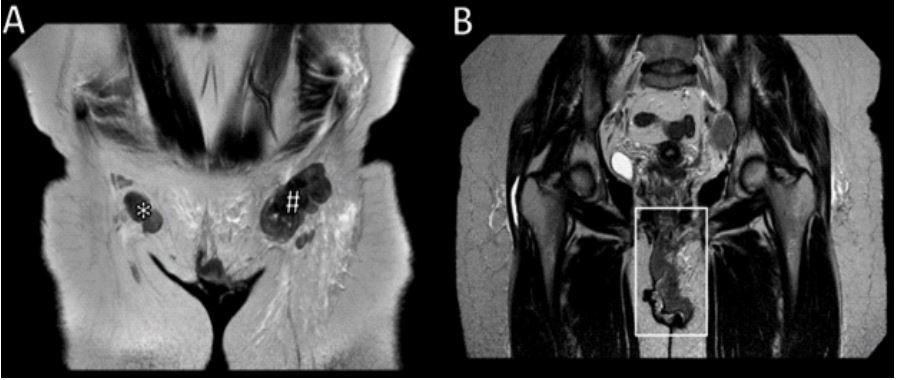
Female, 53 years old, with no relevant personal or family history, no smoking habits nor alcohol or drugs consumption, with out-of-date cervical cancer screening. From a nuclear family, at Duvall’s VI life stage, co-lived with her husband and two children. She went to a General and Family Medicine consultation for vulvar lesion with about one year of evolution, worsening in the past three weeks with bleeding and purulent discharge. Physical examination revealed a large ulcerated and painful lesion (15 cm x 10 cm) involving the leg labia majora and genitocrural sulcus 1,5 cm from the urethra and 1 cm from the anal margin. Hard inguinal adenopathy where palpable bilaterally (Figure 1). The patient was urgently referred to Gynecology. Pelvic magnetic resonance imaging revealed a vulvar tumor with a posterior limit of the lesion immediately anterior to the anus (without involvement of the rectum) and anterior limit at the mons pubis (152 mm x 89 mm x 33 mm) (Figure 2). Likewise revealed invasion of the distal third of the urethra and vagina, and bilateral inguinal adenopathies with necrotic conglomerate on the leg (72 mm transverse axis), external and internal iliac chain on the leg and mesorectum (Figure 3). Imaging showed an enlargement of the leg thigh with edematous infiltration of sog tissues on pubic region and root of the leg thigh. Imaging through Computed Axial Tomography showed no distant metastasis. Biopsy of the lesion confirmed a moderately differentiated squamous cell carcinoma, considered Stage IVB, and proposed upfront chemotherapy. The patient died five days ager the first administration session of carboplatin and paclitaxel.

Discussion
Vulvar cancer is one of the least common forms of gynecologic malignancies. At least 75 percent of vulvar cancer are squamous cell carcinoma with most of them being associated with Human Papillomavirus infection. Risk factors include vulvar or cervical intraepithelial neoplasia, a prior history of cervical cancer, cigareme smoking, vulvar lichen sclerosus, immunodeficiency syndromes, and northern European ancestry [1]. Many patients are asymptomatic at the time of diagnosis. However, some have vulvar pruritus or bleeding. Typically presenting with a vulvar lesion, such as a unifocal vulvar plaque, ulcer, or mass on the labia majora. Usually, lesions are firm, white, red, or skin-colored papules, nodules, or plaques. Varying degrees of erosion or ulceration may occur. The surface is ogen friable. Other presentations could be pain, dysuria, dyschezia, rectal bleeding and enlarged lymph node in the groin or lowerextremity edema, but these are less common and suggest advanced disease. Vulvar cancer is an histologic diagnosis. There are two subtypesti the keratinizing, differentiated, or simplex type, which is more common, especially in older women, and associated with lichen sclerosus but not HPV infection; and the classic, warty or Bowenoid type, predominantly associated with HPV (16,18,33) and found in younger patients [1]. The treatment of vulvar squamous cell carcinoma depends on both the extent of the vulvar lesion and the lymph node evaluation. Vulvar cancer is classified by the 2021 International Federation of Gynecology and Obstetrics (FIGO) staging system. For patients with unresectable, locally advanced disease, it is preferred chemoradiation. For patients who present initially with stage IVB, chemotherapy, generally with the combination of carboplatin and paclitaxel is preferred. Restaging exams with Computed Tomography of the thorax, abdomen, and pelvis every three cycles are performed, and Positron emission tomography is optional. For patients with stage IVB disease limited to the pelvic lymph nodes, definitive chemoradiation with curative intent may be considered. Extension to any of the upper/proximal two-thirds of urethra, upper/proximal two-thirds vagina, bladder mucosa, rectal mucosa, or fixed to pelvic bone are treated with definitive chemoradiation. Ager chemoradiation, many lesions respond completely or there is only a residual tumor, that can be resected surgically [2]. Inguinal and/or femoral node involvement is the most significant prognostic factor for survival. Other prognostic factors include stage (which encompasses size and depth of invasion), capillary lymphatic space invasion, and older age. Reported five-year survival ranges from 70 to 93 percent for patients with negative nodes, to 25 to 41 percent for those with positive nodes. Evidence suggests that patients treated for HPV-associated vulvar cancer have bemer disease outcomes [3]. The present case highlights the importance of longitudinal and regular follow-up in primary care, as the first point of contact to healthcare services and the manager of the patient’s health.
References
- Berek Jonathan S, Karam Amer. Vulvar cancerti Epidemiology, diagnosis, histopathology, and treatment. UpToDate [Internet]. 2023.
- Karam Amer, Berek Jonathan S, Russo Andrea L Russo. Squamous cell carcinoma of the vulvati Medical therapy and prognosis. UpToDate [Internet]. 16 [cited 2024 jan 19]. 2023.
- Karam Amer, Berek Jonathan S, Russo Andrea L Russo. Squamous cell carcinoma of the vulvati Staging and surgical treatment. UpToDate [Internet]. 2024