
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Cat scratch disease
Casper bo Poulsen1*; Luit Penninga2; Peter Bjerring3; Carsten Sauer Mikkelsen4
1Department of Dermato-Venereology, Research Lab, Aalborg University Hospital, Denmark.
2Department of Surgery and Transplantation, Specialist in Surgery, Phd, Clinical Associate Professor, Rigshospitalet, Denmark.
3Department of Dermato-Venereology, Clinical Professor, Dr. Med, Specialist in Dermato-Venereology, Aalborg University Hospital, Denmark.
4Department of Dermato-Venereology, Specialist in Dermato-Venereology, Private Practice in Dermato-Venereology, Brønderslev, Denmark; Research Lab, Aalborg University Hospital, Denmark.
*Corresponding Author : Casper bo Poulsen
Department of Dermato-Venereology, Research
Lab, Aalborg University Hospital, Denmark.
Email: CASPPU@rm.dk
Received : Feb 02, 2024
Accepted : Feb 19, 2024
Published : Feb 26, 2024
Archived : www.jcimcr.org
Copyright : © Poulsen CB (2024).
Abstract
Citation: Poulsen CB, Penninga L, Bjerring P, Mikkelsen CS. Cat scratch disease. J Clin Images Med Case Rep. 2024; 5(2): 2879.
Introduction
Cat Scratch Disease (CSD), caused by the Gram-negative bacterium Bartonella henselae, presents a clinical challenge as a zoonotic infection. Named for its typical mode of transmission through scratches or bites from infected felines most commonly by domestic cats or kittens. CSD has diverse clinical manifestations. The clinical presentation of CSD is ranging from self-limiting lymphadenopathy to severe systemic complications that require antibiotic treatment [1]. Most cases of CSD are self-limiting symptoms vary from person to person as well as the severity of the symptoms. Often the primary lesion is seen with small papule or pustule at the site of the scratch or bite, appearing within 3-10 days after exposure to an infected cat. Regional lymphadenopathy CSD is typically observed as a characteristic feature and therefore is one of the hallmark clinical manifestations of the condition. This enlargement of lymph nodes occurs in proximity to the primary lesion, commonly within 1 to 3 weeks after exposure. The affected lymph nodes become tender and swollen [2]. While most cases of CSD follow a benign and self-limiting course, atypical manifestations can occur, especially in immunocompromised individuals. These may include hepatosplenic involvement, neurologic manifestations, and, rarely, bacillary angiomatosis [3]. It’s important to note that the clinical presentation of CSD can mimic other infectious or inflammatory conditions, making diagnosis challenging. Patients can be tested by PCR with swap around the lesions or by plasma antibody test if the clinical presentations require this or is atypical.The antibiotic treatment of CSD is recommended despite the self-limiting nature of the disease to prevent evolvement and severe progression of the disease [4,5]. The bacteria are susceptible to several antibiotics, azithromycin therapy has shown a more rapid effect in the treatment [6].
Case report
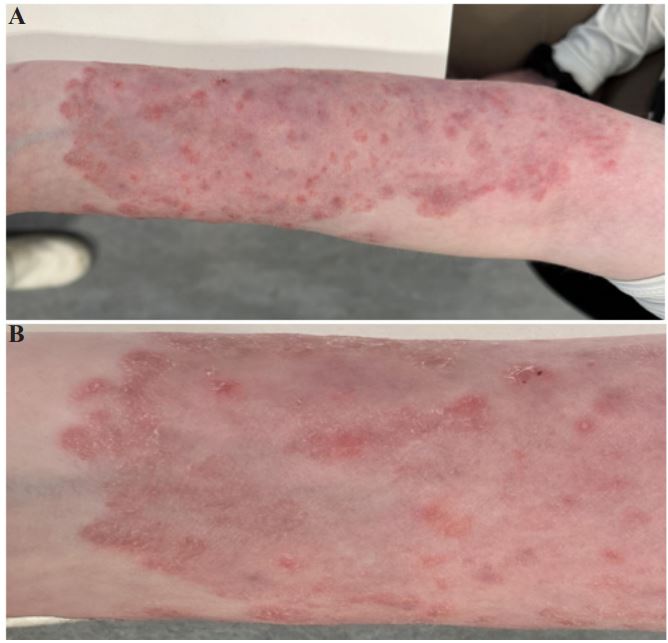
A 26-year-old woman, previously healthy, sought medical attention after being scratched and bitten by a kitten in November 2022 on her left forearm. The kitten was later diagnosed with ringworm. Initial symptoms included 3-5 mm reddish-brown papules at the site of the scratches, evolving into pustules 3-10 days after the incident. Subsequently, a larger rash developed on the left forearm, initially presenting as small erythematous patches, gradually spreading over the course of 2-4 months. Upon consultation with a dermatologist, it was observed that the rash had extended to the entire volar aspect of the forearm (Figure 1). The patient remained without systemic symptoms, such as fever or malaise, even as the rash progressed to involve the entire volar aspect of the forearm, however lymphadenopathy became evident in the left axilla during the dermatological manifestations. Despite attempts at topical treatments, including Dermovat, Brentan, and most recently, Fucicort, the rash persisted. Fucicort however showed limited efficacy, resulting in less itching and reduced redness of the rash. Upon consultation with a dermatologist, the patient was diagnosed with cat scratch disease. Antibiotic treatment was initiated with azithromycin at a dosage of 500 mg daily for 3 days. Following this course, the patient experienced significant improvement in both the skin symptoms and left axillary lymphadenopathy. This case highlights the importance of considering cat scratch disease in patients with atypical dermatological presentations, particularly in the context of exposure to kittens.
References
- Klotz SA, Ianas V, Elliott SP. Cat-scratch Disease. Am Fam Physician. 2011; 83(2): 152-5. PMID: 21243990.
- Smith DL. Cat-scratch disease and related clinical syndromes. Am Fam Physician. 1997; 55(5): 1783-9. 1793-4. PMID: 9105205.
- Chomel BB. Cat-scratch disease. Rev Sci Tech. 2000; 19(1): 136- 50. doi: 10.20506/rst.19.1.1204. PMID: 11189710.
- Bass JW, Freitas BC, Freitas AD, Sisler CL, Chan DS, Vincent JM, Person DA, Claybaugh JR, Wittler RR, Weisse ME, Regnery RL, Slater LN. Prospective randomized double blind placebocontrolled evaluation of azithromycin for treatment of catscratch disease. Pediatr Infect Dis J. 1998; 17(6): 447-52. doi: 10.1097/00006454-199806000-00002. PMID: 9655532.
- Margileth AM. Antibiotic therapy for cat-scratch disease: clinical study of therapeutic outcome in 268 patients and a review of the literature. Pediatr Infect Dis J. 1992; 11(6): 474-8. PMID: 1608685.
- Conrad DA. Treatment of cat-scratch disease. Curr Opin Pediatr. 2001; 13(1): 56-9. doi: 10.1097/00008480-200102000-00010. PMID: 11176245.