Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 5
IgG4-related pleuritis mimicking tuberculous pleurisy
José Richard Tenazoa Villalobos1,3*; Edgar Fermín Yan Quiroz2,3
1Hospital Víctor Lazarte Echegaray – Es Salud, Trujillo 13006, Peru.
2Virgen de la Puerta High Complexity Hospital – Es Salud, La Esperanza 13013, Peru.
3Faculty of Medicine, Universidad Privada Antenor Orrego, Trujillo 13008, Peru.
*Corresponding Author : Kohei Yoshimine
Department of Respiratory Medicine, Iizuka Hospital, Japan.
Tel: +81948223800;
Email: k.yoshi.med@gmail.com
Received : Feb 02, 2024
Accepted : Feb 20, 2024
Published : Feb 27, 2024
Archived : www.jcimcr.org
Copyright : © Yoshimine K (2024).
Abstract
Citation: Yoshimine K. IgG4-related pleuritis mimicking tuberculous pleurisy. J Clin Images Med Case Rep. 2024; 5(2): 2882.
Description
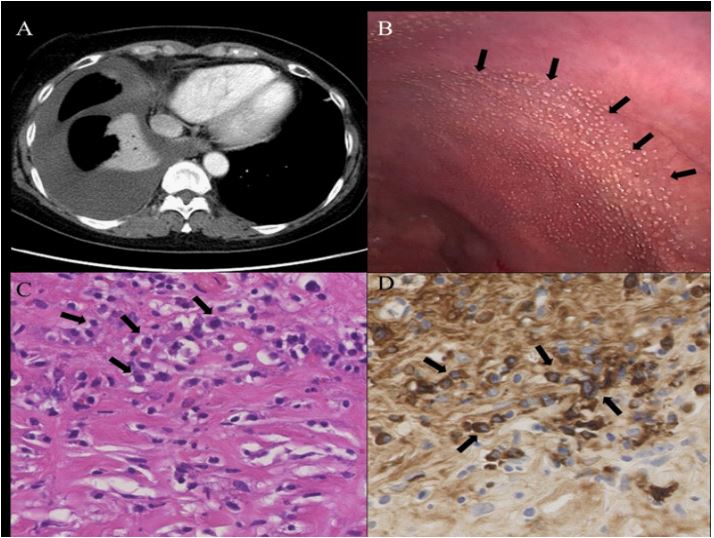
A 55-year-old Japanese woman with a medical history of uterine fibroids presented with dyspnea on exertion for three months. She did not have so-called B symptoms such as weight loss or night sweats. She was a carrier of the hepatitis B virus, and had no medications and smoking history. Chest X-ray and computed tomography demonstrated right-sided pleural effusion (Figure 1A). Serum IgG was slightly elevated (2,038 mg/dL normal, 870-1,700 mg/dL), and serum IgG4 level was markedly elevated (578 mg/dL normal, 4.8-105 mg/dL). Interferon gamma release assay for tuberculosis was negative, and her pleural effusion was a lymphocyte-predominant (40%) exudates with high Adenosine Deaminase (ADA) level (78.2 units/L). The staining of her pleural fluid showed no microorganisms, and cultures grew no microorganisms, including tuberculosis. Thoracoscopy showed multiple white nodules throughout the right parietal pleura (Figure 1B), which were biopsied. Histopathological examination of the lesion revealed lymphoplasmacytic infiltration and fibrosis without malignancy, granuloma, or microorganisms (Figure 1C). Immunohistochemical staining revealed abundant IgG4-positive plasma cells infiltration (Figure 1D). Acid-fast staining of the specimen and polymerase chain reaction for tuberculosis were both negative. Based on these findings, the patient was diagnosed with IgG4-related pleuritis. Other tests showed no lesions in other organs of the body. IgG4-related disease can involve nearly all organs and multiple-organ involvement is common. Lesions of the mediastinum, airways, and lung parenchyma are common in IgG4-related lung disease, and pleural lesions are rare, with only a dozen or so cases reported so far. The thoracoscopic findings of IgG4-related pleurisy that have been reported include normal, milky pleural plaques, diffuse inflammatory thickening of the pleura, and very rarely multiple pleural nodules. Multiple white nodules on gross thoracoscopic appearance and lymphocyte-predominant exudative pleural effusion with high ADA level are highly specific findings for tuberculous pleurisy, but IgG4-related pleurisy should be mentioned as well.