Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 5
Idiopathic hepatic vein calcification
Aditya Garg1,2; Bela Kis1*
1Diagnostic and Interventional Radiology, H. Lee Moffitt Cancer Center and Research Institute Tampa, Florida, USA.
2University of South Florida Health Morsani, College of Medicine Tampa, Florida, USA.
*Corresponding Author : Bela Kis
Diagnostic and Interventional Radiology, H. Lee
Moffitt Cancer Center and Research Institute
Tampa, Florida, USA.
Tel: 813-745-8425;
Email: bela.kis@moffitt.org
Received : Jan 31, 2024
Accepted : Feb 23, 2024
Published : Mar 01, 2024
Archived : www.jcimcr.org
Copyright : © Kis B (2024).
Abstract
This case represents the first reported patient with idiopathic hepatic vein calcification.
Citation: Garg A, Kis B. Idiopathic hepatic vein calcification. J Clin Images Med Case Rep. 2024; 5(3): 2891.
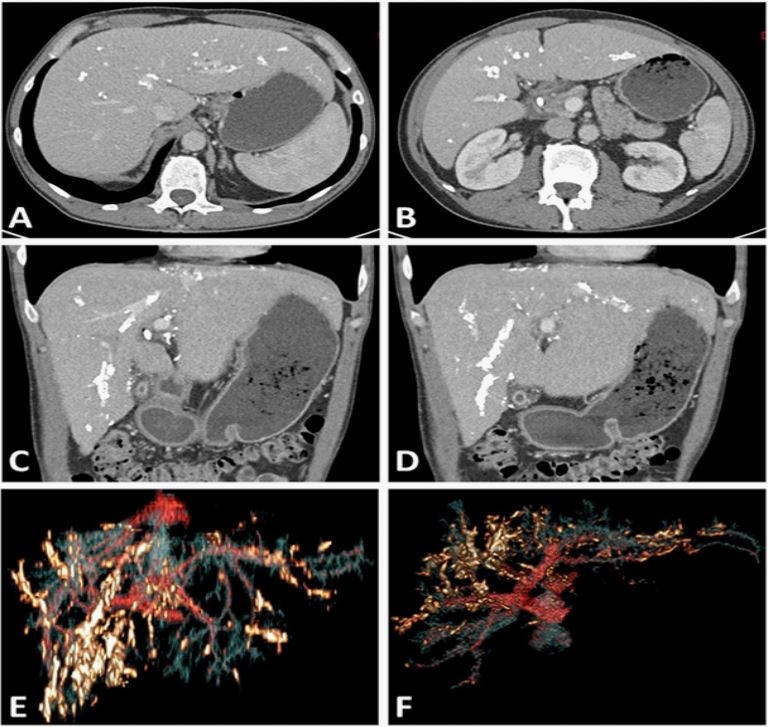
Description
A 51-year-old male with a history of seizure disorder presented with jaundice. He was diagnosed with primary sclerosing cholangitis and unresectable metastatic hilar cholangiocarcinoma (Klatskin’s tumor). Axial (A,B) and coronal (C,D) contrast-enhanced CT scan showed prominent hepatic vein calcification with minimal calcification in few peripheral portal vein branches and no calcification in the hepatic artery and its branches. His hepatic vein was patent with no history of BuddChiari syndrome. There was no prior imaging available, and it was unknown when the calcification occurred. The patient did not have history of calcium/phosphorous homeostasis disorders, parasitic disease, tuberculosis, diabetes, kidney disease, portal hypertension, or atherosclerosis which are known potential risk factors of hepatic vascular calcifications. The patient died 32 months after the diagnosis of cholangiocarcinoma. The cause of his hepatic vein calcification is unknown. According to our knowledge this is the first reported case of idiopathic hepatic vein calcification with patent hepatic veins in a patient without history of prior Budd-Chiari syndrome.