
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Subcutaneous panniculitis like T - cell lymphoma: Case series report
Hieu CC1; Hang VT*; Hoang TN1; Quan HVH2; Tien DT3; Lam DTT3; Linh NT4; Tuyen PV1; Chuong TV1; Tien LQ2; Nguyet NN1
1Bach Mai Hospital, Vietnam.
2Ha Noi Medical University, Vietnam.
3Duc Giang Hospital, Vietnam.
4Vinmec International Hospital, Vietnam.
*Corresponding Author : Hang VT
Bach Mai Hospital, Vietnam.
Tel: (+84) 988-600-115;
Email: Vuhangbc92@gmail.com
Received : Jan 31, 2024
Accepted : Feb 23, 2024
Published : Mar 01, 2024
Archived : www.jcimcr.org
Copyright : © Hang VT (2024).
Abstract
Subcutaneous Panniculitis-like T-cell lymphoma (SPTCL) is characterized by malignant lymphoid cell infiltration within the lobules of panniculitis. Diagnosis of SPTCL requires distinguish from primary cutaneous c/d T-cell lymphoma, peripheral T-cell lymphoma, and lupus panniculitis. We reported 4 cases with the diagnosis of SPTCL. Five patients were admitted to the hospital with skin lesions (erythema nodosum, skin thickening, skin ulcers) accompanied by persistent fever. Skin biopsies of them have infiltrative images of septal adipose tissue inflammation, immunohistochemical staining were positive for CD3, CD4, CD8, high Ki index. SPTCL is mainly based on biopsy. If SPTCL is diagnosed early, the prognosis is good.
Keywords: Panniculitis; T-cell lymphoma; Hemophagocytic; Lymphohistiocytosis.
Citation: Hieu CC, Hang VT, Hoang TN, Quan HVH, Tien DT, et al. Subcutaneous panniculitis like T - cell lymphoma: Case series report. J Clin Images Med Case Rep. 2024; 5(3): 2892.
Introduction
Subcutaneous panniculitis-like T cell lymphoma (SPTCL) is a type of lymphoma that affects the subcutaneous tissue and is characterized by the expression of a cytotoxic T cell immunophenotype. This lymphoma primarily affects the skin and is caused by T cells that attack the subcutaneous tissue [1]. Less than 1% of T cell lymphomas are SPTCL, which can manifest at any age, with 20% of patients being under 20 years old. SPTCL can be diagnosed by evaluating clinical and pathological features. This type of lymphoma is identified by the presence of nodules or subcutaneous plaques on the trunk and extremities, ranging in size from 0.5 to 2.0 cm. Patients may experience B symptoms, including fever, fatigue, and weight loss. Additionally, HLH can occur in 14% to 27% of cases of SPTCL [2]. In SPTCL, the typical histopathological appearance is the presence of atypical lymphocytes infiltrating the subcutaneous tissue in a lobular pattern, with adipocytes rimming in a lace-like manner. Patients diagnosed with subcutaneous panniculitis-like T cell lymphoma had a three-year survival rate of 85.2%, which was comparable to the results of the EORTC study [1]. Our report included four patients with erythema nodosum, with/without ulceration. All 4 patients had a confirmed diagnosis of SPTCL after biopsy, and all 4 patients are now alive.
Case presentations
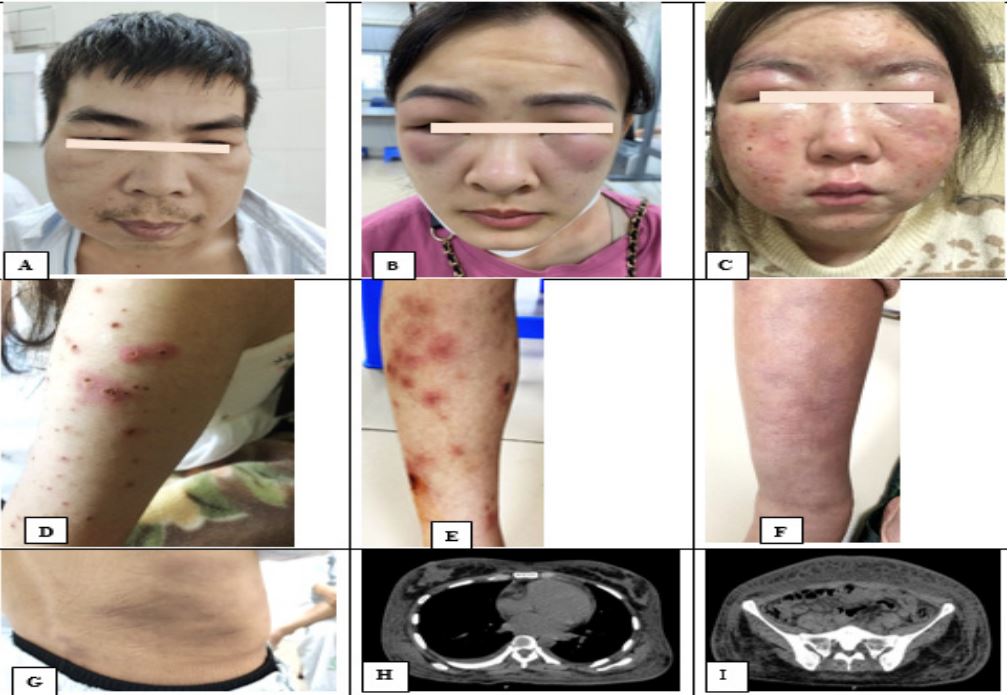
Patient No.1: A 43-year-old man had history with fever for the past 8 months. The patient had fever accompanied by the appearance of infiltrative, hard and hyperpigmented skin lesions, and painful when pressed. In addition, the jaw angle and neck were edematous, painless, and without pruritus. The examination have spenlomegaly, and cervical and inguinal lympho nodes. Tests to ruled out autoimmune disease, tuberculosis and virus were also normal. The patient was treated by experience based antibiotic therapy but unimprovement.
Patient No.2: A 29-year-old woman, with a stable history of Basedow has received radioactive I131 3 years ago. Before admission 5 months, she developed febrile, 3-4 fevers per day with Tmax 39,5o C, and in the evening, loose stools. She was diagnosed with peritoneal tuberculosis based on the result of the peritoneal biopsy. Results of the biopsy of the bone marrow showed no hematologic malignancy. She ended up receiving RHZE with levofloxacin for 41 days after, but without any significant improvement. In addition, the abdomen and left forearm had nodular lesions the size of 3x4 cm, no skin ulcers. Computed Tomography (CT) of the abdomen showed diffuse soft-tissue edema in the abdomen, chest, pelvis, and hips on both sides and no abscess.
Patient No.3: A 23-year-old woman, a month before admission, the patient appeared scattered subcutaneous, erythematous papules on both lower extremities, the largest papule size was 3*4 cm. The biggest nodule had an ulcer on the right leg measuring 0.5*0.5 cm, black scales, no pain, and no itching. In addition, the patient had no fever, no joint pain, and normal cardiovascular and respiratory examination. The tissue from the biopsied skin confirmed diagnosis with subcutaneous panniculitis-like T-cell lymphoma. The patient was treated with methylprednisolone 64 mg per day. After two months, the patient’s skin lesion had almost completely subsided. However, the fat around the eye sockets and the cheeks were atrophied.
Patient No.4: A 23-year-old female patient with 3 years history with a red rash appeared on the face. The lesion was on nasolabial folds, neck, arms, forearms, thighs, and legs on both sides. The patient was diagnosed with discoid lupus, treated with oral corticosteroids Dexamethasone 2 mg/day with topical hydrocortisone Acetate 15 g and tacrolimus 0.03% applied in batches. 1 week before hospitalize, the patient had facial redness, infiltrative papules, painful pressure, a few ulcers 1x1 cm in size with yellow exudate. Dot-type ulcers, nodules in the arms on both sides, eyelids are mildly swollen, painless, and not itchy. No cervical, supraclavicular, subclavian, axillary, or inguinal lymph nodes were palpable.
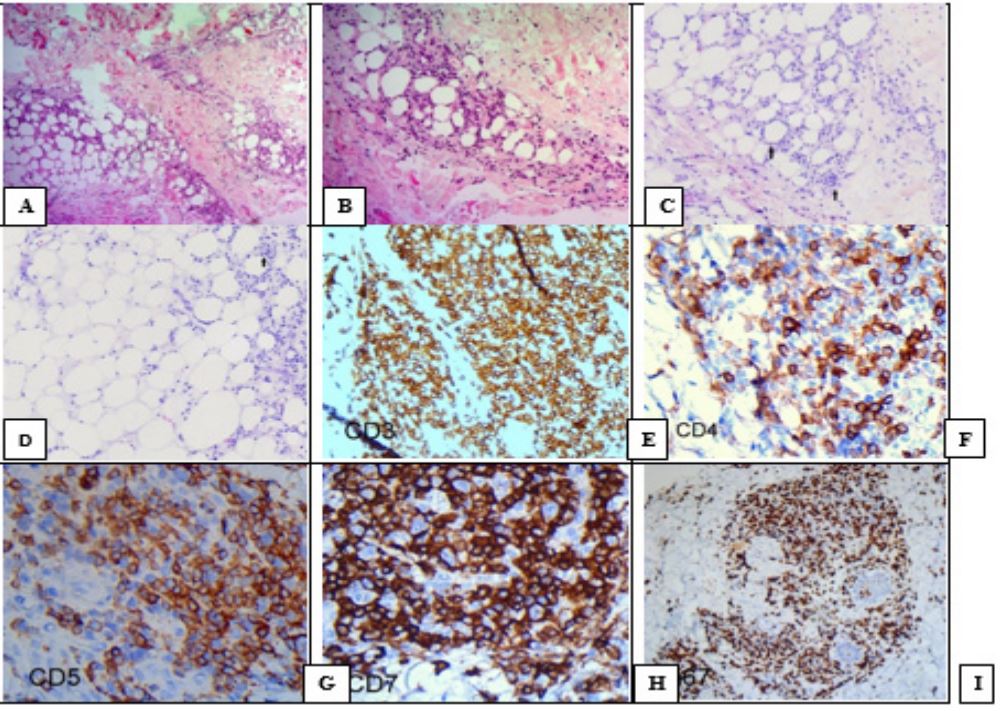
All 4 patients had deep skin biopsies and histopathological showed lobular fatty tissue infiltration. Immunohistochemical staining positive for CD43, CD8, granzymb, high Ki67 index. They were diagnosed SPTCL (Figure 2).
Discussion
The initial documentation of subcutaneous panniculitis-like T cell lymphoma was by Gonzalez et al. in 1991 [3], which is a type of panniculitis that involves the infiltration of neoplastic cytotoxic T cells into the subcutaneous tissue, mimicking the symptoms of panniculitis. Subcutaneous panniculitis-like T cell lymphoma makes up a small proportion of peripheral T cell lymphomas, accounting for less than 1% [1]. Panniculitis is characterized by unique attributes such as subcutaneous nodules that vary in shape, number, and location, mainly on the legs (71%), arms (62%), torso (56%), and/or face (25%). These nodules tend to ulcerate and secrete fluid [1,4]. Subsequent assessments are essential to determine if nodules tend to develop ulcers and to examine their characteristics, including color, texture, and location. SPTCL is also crucial to identify any possible systemic symptoms or abnormalities in blood tests to achieve an accurate diagnosis. Symptoms such as fever, night sweats, and weight loss are indicators of systemic symptoms, also known as B symptoms. In a study conducted by Ohtsuka et al. in Japan, 16 cases of SPTCL were reviewed, and their clinical features were compared with European and Chinese patients. Japanese cases had a higher prevalence of B symptoms, while autoimmune disorders were more common in European cases [4]. Four patients in our report were also screened for autoimmune disease, however no autoimmune disease was confirmed. All 4 patients had B symptoms and erythema nodosa on admission.
An algorithmic approach to histopathological diagnosis of panniculitides can be employed, relying primarily on the inflammation type and location to aid in identifying a specific panniculitis diagnosis in most cases [5]. The initial stage of the process involves determining whether the inflammatory infiltrate is more concentrated in the septa or lobule. If the lobules are unaffected or only have minor peripheral lobular involvement, then it is likely that the panniculitis is primarily septal. Conversely, if both the lobules and septa are affected, then it is mostly lobular. The subsequent step is to assess whether vasculitis is present. Steps three and four are usually evaluated concurrently since they entail a thorough examination of the inflammatory infiltrate composition and identification of additional characteristics such as the type of adipocyte necrosis, presence of sclerosis, foreign bodies, crystals, microorganisms, or calcium deposits. It is recommended that the biopsy is performed at a deep level beneath the subcutaneous fat and that an elliptical shape is preferred over a punch biopsy.
SPTCL is identified by the infiltration of cancerous lymphoid cells within the lobules of panniculitis, with no effect on the interlobular septum, epidermis, or dermis. The neoplastic lymphoid cells usually have angulated, hyperchromatic nuclei, indistinct cell borders, and limited cytoplasm. Other usual observations entail dispersed histiocytes, plasma cells, neutrophils, mitoses, apoptotic bodies, karyorrhectic debris, and areas of fat necrosis. Moreover, the abnormal cells frequently surround individual fat cells [6]. The histological features of SPTCL are defined by the occurrence of cancerous T-cells that are pleomorphic and infiltrate the adipose tissue beneath the skin. This infiltration is accompanied by macrophages and does not involve the epidermis or dermis. The infiltration is identified by the presence of atypical T-cells enveloping fat cells, which often have necrosis and karyorrhexis. The lobular area is the main site of impact, with only a small amount of involvement of the septa. CD2, CD3, CD7, CD8, beta F1, and activated cytotoxic proteins (T-cell intracellular antigen [TIA-1], granzyme B [GzB], and/or perforin) are typically expressed by the atypical lymphoid cells, as identified through immunohistochemical analysis. However, CD4, CD56, and CD30 are not present. Additionally, a high Ki-67 proliferation index is commonly observed [7]. The differential diagnosis with lupus adipose tissue is very important in terms of prognosis and treatment orientation. LeBlanc et al. found that “hotspot” areas with increased Ki-67 staining were useful in differentiating between SPTCL and LEP [2].
The objectives of treatment SPTCL involve halting the proliferation of atypical T cells, preventing excessive cytokine release, and maintaining a balanced immune environment. There is no universally recognized method for treating SPTCL. In France, David Michonneau et al. performed a clinical study that demonstrated that immunosuppressive drugs are more effective in treating SPTCL than polychemotherapy with complete remission rates of 81.2% and 28.5%, respectively [8]. If patients develop HLH, aggressive management may be necessary. Singleagent corticosteroids are a current treatment option for SPTCL. In 20 cases reported by Go and Wester, initial treatment with steroids resulted in complete and partial remissions in six (30%) and four (20%) cases, respectively [9]. Our patient had two cases of hematologic lesions, assigned a combination chemotherapy regimen (CHOP and CVE-P), the remaining two patients had no hematologic lesions, one received methylprednisolone, the other received CHOP due to lung injury on PET-CT. And all 4 patients are alive after treatment.
Conclusion
SPTCL is an uncommon clinical presentation of ulcerating panniculitis. Clinical symptoms of panniculitis are nonspecific, leading to being diagnosed late. The diagnosis of SPTCL is majorly based on biopsies and immunohistochemistry.
References
- Willemze R, Jansen PM, Cerroni L, et al. Subcutaneous panniculitis-like T-cell lymphoma: definition, classification, and prognostic factors: an EORTC Cutaneous Lymphoma Group Study of 83 cases. Blood J Am Soc Hematol. 2008; 111(2): 838-845.
- LeBlanc RE, Tavallaee M, Kim YH, Kim J. Useful parameters for distinguishing subcutaneous panniculitis-like T-cell lymphoma from lupus erythematosus panniculitis. Am J Surg Pathol. 2016; 40(6): 745-754.
- Gonzalez CL, Medeiros LJ, Braziel RM, Jaffe ES. T-cell lymphoma involving subcutaneous tissue: a clinicopathologic entity commonly associated with hemophagocytic syndrome. Am J Surg Pathol. 1991; 15(1): 17-27.
- Ohtsuka M, Miura T, Yamamoto T. Clinical characteristics, differential diagnosis, and treatment outcome of subcutaneous panniculitis-like T-cell lymphoma: a literature review of published Japanese cases. Eur J Dermatol. 2017; 27: 34-41.
- Llamas-Velasco M, Fernández-Figueras MT. A practical approach to the clinico-pathological diagnosis of panniculitis. Diagn Histopathol. 2021; 27(1): 34-41.
- Gupta P, Saikia UN, Arora S, De D, Radotra BD. Panniculitis: A dermatopathologist’s perspective and approach to diagnosis. Indian J Dermatopathol Diagn Dermatol. 2016; 3(2): 29.
- Lin EC, Liao JB, Fang YH, Hong CH. The pathophysiology and current treatments for the subcutaneous panniculitis‐like T cell lymphoma: An updated review. Asia‐Pacific J Clin Oncol. 2023; 19(1): 27-34.
- Michonneau D, Petrella T, Ortonne N, et al. Subcutaneous panniculitis-like T-cell lymphoma: immunosuppressive drugs induce better response than polychemotherapy. Acta Derm Venereol. 2017; 97(3): 358-364.
- Go RS, Wester SM. Immunophenotypic and molecular features, clinical outcomes, treatments, and prognostic factors associated with subcutaneous panniculitis‐like T‐cell lymphoma: a systematic analysis of 156 patients reported in the literature. Cancer Interdiscip Int J Am Cancer Soc. 2004; 101(6): 1404-1413.