
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
A case report on CT guided percutaneous NBCA glue injection at probable leak site as a bailout in a postoperative refractory chyloperitoneum without exact demonstrable leak site on lymphangiogram
Devara Anil Kashi Vishnuvardhan1*; Sandeep Botcha2; Chodisetti Subba Rao3; Sujatha Naidu4; Balaji Patel Kola5; Ajit Yadav6; Payala Vijayalakshmi7
1Lead Consultant, Radiology and Interventional Radiology, Medicover Hospitals, MVP, Visakhapatnam, Andhra Pradesh, India.
2Consultant Interventional Radiologist, Medicover Hospitals, MVP, Visakhapatnam, Andhra Pradesh, India.
3Head of Urology, Medicover Hospitals, MVP, Visakhapatnam, Andhra Pradesh, India.
4Head of Radiology, Pinnacle Hospital, Visakhapatnam, Andhra Pradesh, India.
5Professor, Interventional Radiologist, Apollo College of Medical Sciences and Research, Hyderabad, Telangana, India.
6Consultant Interventional Radiologist, Sri Gangaram Hospital, Rajendra Nagar, Delhi, India.
7Department of Microbiology, Associate Professor, GITAM Institute of Medical Sciences and Research, GITAM Deemed to be University, Visakhapatnam, India.
*Corresponding Author : Vishnuvardhan DAK
Lead Consultant, Radiology and Interventional Radiology, Medicover Hospitals, MVP, Visakhapatnam,
Andhra Pradesh, India.
Email: vpayala@gitam.edu
Received : Jan 27, 2024
Accepted : Feb 26, 2024
Published : Mar 04, 2024
Archived : www.jcimcr.org
Copyright : © Vishnuvardhan DAK (2024).
Abstract
The main goal of the present case report is to propose a minimally invasive percutaneous approach in managing postoperative complication of severe chyloperitoneum. A 41-year-old female underwent laparoscopic donor left nephrectomy and developed chyloperitoneum after six weeks. Because of no response to medical management, no demonstrable chyle leak site on conventional lymphangiogram, no response to lymphatic maceration and glue injection at left L4/L5 level, and continuing persistent severe chyloperitoneum, we performed direct percutaneous Computed Tomography (CT) guided glue injection at probable leak site based on operative details and nonenhanced CT of the abdomen. Complete resolution of chyloperitoneum was achieved at two weeks. We believe that prompt utilization of these percutaneous techniques can achieve timely resolution and should be considered in managing such patients. To our knowledge, this novel approach hasn’t been described in any of the earlier studies.
Keywords: Refractory chyloperitoneum; Probable leak site; CTGuided percutaneous glue injection.
Citation: Vishnuvardhan DAK, Botcha S, Rao SC, Naidu S, Kola BP, et al. A case report on CT guided percutaneous NBCA glue injection at probable leak site as a bailout in a postoperative refractory chyloperitoneum without exact demonstrable leak site on lymphangiogram. J Clin Images Med Case Rep. 2024; 5(3): 2894.
Introduction
Postoperative chyloperitoneum was first reported by Clayman et al. in the use of laparoscopic nephrectomy in 1991 and is more common after radical or donor nephrectomy. Chyloperitoneum causes local complications, such as delayed wound healing, infections, severe malnutrition, and immunodeficiency [1,2]. In the failure of traditional modes of medical management of postoperative refractory chyloperitoneum, conventional trans pedal or intranodal lymphangiography is a valuable tool in diagnostic and therapeutic approaches with an efficacy rate of about 70% [1-3]. Alternatively, peritoneovenous shunting and percutaneous transabdominal embolization can be performed, especially in patients with poor performance status [2]. Herein, we present a post-operative complication of severe refractory chyloperitoneum following laparoscopic donor nephrectomy not responding to medical management, conventional lymphangiogram, lymphatic maceration, and glue embolization (below the level of the operative site), which was successfully managed by a novel minimally invasive percutaneous technique that can achieve timely resolution and should be considered in the management of such patients as a viable option.
Case presentations
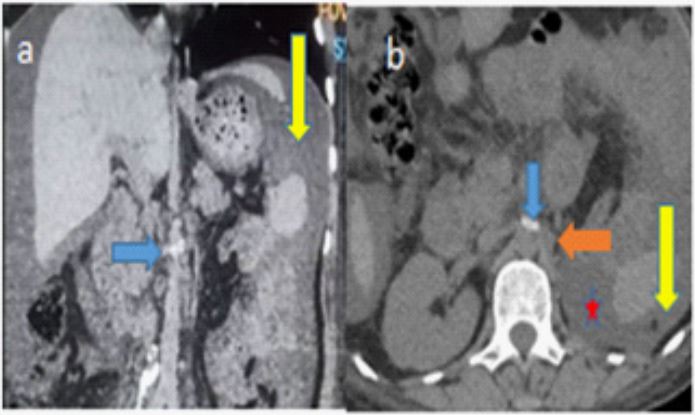
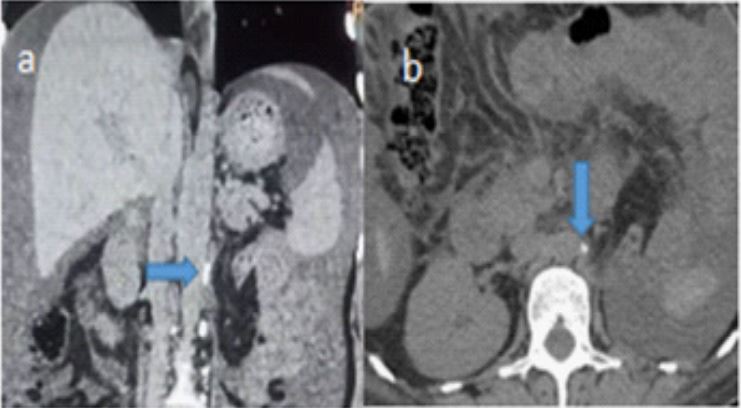
A 41-year-old female underwent laparoscopic donor left nephrectomy and developed significant abdominal pain, distension, and bilateral mild limb swelling approximately six weeks postoperative. Her vitals, complete blood picture, and liver and renal function tests were normal. The chest radiograph was normal. A Computed Tomography (CT) abdomen scan showed gross ascites and an absent left donor kidney with adjacent midline surgical clips. Ascitic fluid tap revealed milky white fluid with triglyceride content (chylomicrons) of 126 mg/dl, confirming chyloperitoneum. Conservative management consists of a high protein-fat-free diet, subcutaneous octreotide injections (150 mcg/ml thrice daily), and peritoneal catheter drain for ascites. The patient continued high-output (4 to 8 liters per day) chylous fluid drainage for over a month. Because of no response to conservative management, she underwent an image-guided lipiodol lymphangiogram from bilateral inguinal lymph nodes, which couldn’t demonstrate the exact site of the chyle leak. Hence, lymphatic maceration and glue embolization of lymphatics at the left L4/L5 level below the level of the operative site was done. However, a large volume of chyloperitoneum persisted even after 20 days.
Considering operative details of simple donor nephrectomy, her current clinical status, reviewing the CT abdominal imaging of the operative site and prior lymphangiogram, our plan of action was:
1. Repeat the lymphangiogram with the guide of the prior lipiodol lymphangiogram.
2. Direct puncture of cisterna chylli or thoracic duct lymphangiogram and embolization of leak.
3. Left subclavian vein angiogram, thoracic duct cannulation, lymphangiogram, and embolization of leak.
4. Percutaneous direct glue injection of probable leak site under CT guidance – which we could identify considering operative details and plain CT abdomen images. We counselled the patient and family regarding plan 4, its risks involved, and benefits, for which they consented after the failed attempts of plans 1 and 2. The patient didn’t agree to plan 3.
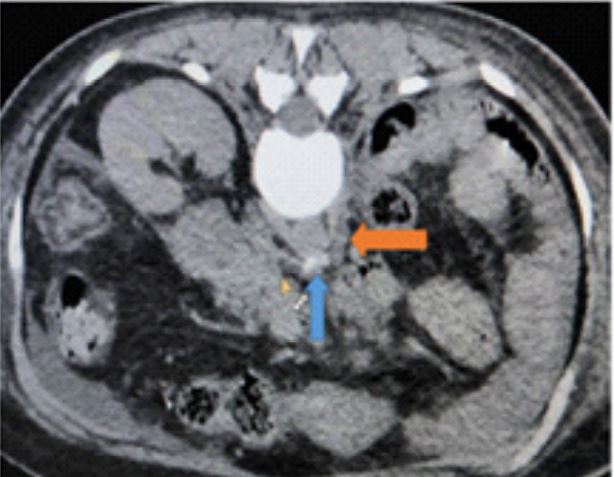
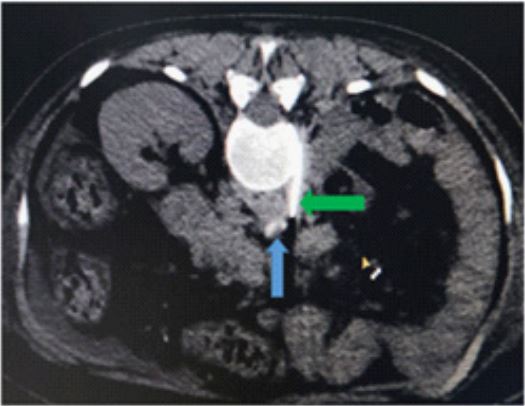
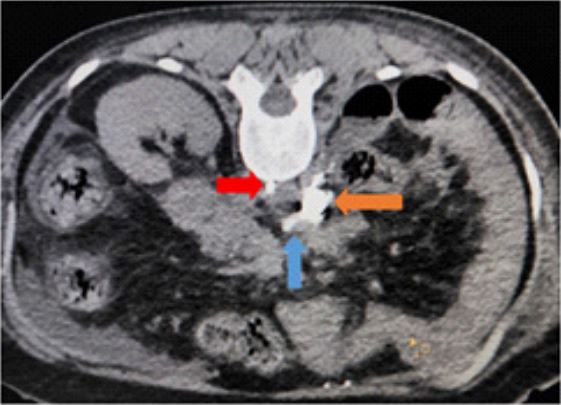
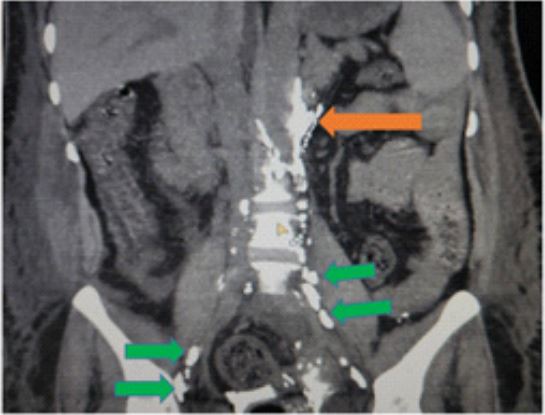
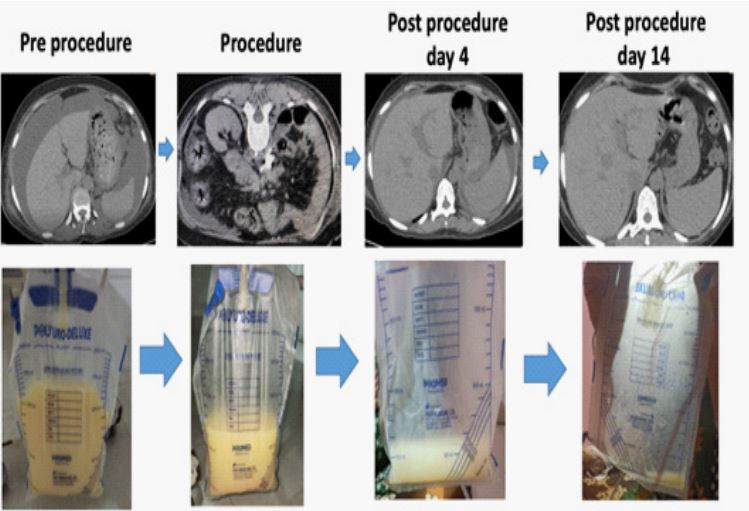
Pre-procedural basic blood investigations were done, and anesthetic clearance was obtained. We were able to localize probable leak site in between the horizontal and vertical surgical clips on plain CT abdomen (Figures 1-3). With the patient in a prone position, under local anesthesia (LOX 2%), a 22 G LP needle (Figure 4) was targeted at the probable leak site under CT guidance, following which 2.5cc of 1:1; Glue: Lipiodol was injected (Figures 5 and 6) embolising the lymphatics, thoracic duct above and below the injected site. The embolised lymphatics were in line with the lipiodol-stained lymphatic channels due to prior lymphangiogram, further confirming the precise intralymphatic spread of glue injection. Post-procedure serial ultrasound, CT abdomen, and urobag drain output (Figure 7) demonstrated gradual and complete resolution of ascites, abdominal distension, and bilateral pedal edema 14 days postprocedure
Discussion
Chyloperitoneum is a less frequently encountered complication of laparoscopic renal surgery [1,2,4]. It is due to routine non-ligation of lymphatics, even though they are usually burned with sealing devices like electrocautery and ultrasonic shears [2]. Usually, a chyle leak due to minor lymphatic channel disruption improves spontaneously without any medical intervention. Conservative medical management as the first line consists of dietary modifications with a high protein, low fat, medium chain triglyceride diet with or without total parenteral nutrition and high-dose Octreotide, which aims to decrease mesenteric lymphatic flow. A surgical option is recommended, wherein 4 to 12 weeks of conservative management fails in treating refractory chyloperitoneum [2,4]. Lymphangiography, transabdominal catheterization of the cisterna chyli or thoracic duct, percutaneous thoracic duct embolization, an established alternative to surgical ligation of the thoracic duct, especially in refractory chyloperitoneum with poor performance status, where no typical dominant lymph ducts can be targeted to control the leak [2,4]. There are few cases of percutaneous embolization technique in literature with limited data [2,4]. To our knowledge, CT-guided glue injection into a chyle leak following a simple donor nephrectomy has not been previously described. A similar glue embolization case of chyle leak following nephrectomy with lymphadenectomy for renal malignancy was described by Paige Ashley Hargis et al. in the recent past (2021), performed within the 1st week of post-operative chyle leak complication where the site of leak was known on lymphangiography [4]. In our case, the period of percutaneous treatment was post-four weeks of conservative management, and a conventional lymphangiogram couldn’t demonstrate the active chyle leak site. Based on operative details of a relatively simple donor nephrectomy, CT abdominal imaging of the operative site, we could localize the probable chyle leak site, which was targeted and embolised with complete resolution of chyloperitoneum within two weeks.
In our observation, special care must be taken during procedure planning and execution. Drainage of ascites before the procedure can provide an optimal environment in preventing glue dispersion and dilution at the targeted area. Limitations of failure to seal the lymphatic leak site, iatrogenic injury, and nontarget embolization of adjacent vascular (aorta, inferior vena cava), neural structures, and bowel loops should be considered while performing such procedures.
Conclusion
A postoperative serious complication of large volume refractory chyloperitoneum, where conventional lymphangiogram may not demonstrate the site of the active leak, operative details, and cross-sectional imaging may play an essential role in providing a clue to probable leak site, which can be targeted and embolised with glue percutaneously under CT guidance resulting in gradual and complete resolution. Prompt utilization of minimally invasive image-guided percutaneous techniques can achieve timely resolution and should be considered in managing such patients. After the literature survey, this was the first study to describe this novel approach.
Declarations
Conflict of interest: The authors declared no conflict of interest.
Data availability: The authors confirm that the data supporting the findings of this study are available within the article.
References
- Lee EW, Shin JH, Ko HK, Park J, Kim SH, Sung KB. Lymphangiography to treat postoperative lymphatic leakage: a technical review. Korean J Radiol. 2014; 15(6): 724-32. doi: 10.3348/ kjr.2014.15.6.724. Epub 2014 Nov 7. PMID: 25469083; PMCID: PMC4248627.
- Kim Bum S, Kwon Tae G. Chylous ascites in laparoscopic renal surgery: Where do we stand. World Journal of Clinical Urology. 2016; 5(1): 37-44.
- Pan F, Loos M, Do TD, Richter GM, Kauczor HU, Hackert T, Sommer CM. Percutaneous afferent lymphatic vessel sclerotherapy for postoperative lymphatic leakage after previous ineffective therapeutic transpedal lym-phangiography. Eur Radiol Exp. 2020; 4(1): 60. doi: 10.1186/s41747-020-00188-9. PMID: 33135104; PMCID: PMC7604276.
- Hargis PA, Henslee B, Pokala N, Bhat A. Percutaneous Lymphatic Maceration and Glue Embolization for High-output Chylous Ascites after Robot-assisted Laparoscopic Nephrectomy and Lymphadenectomy. J Clin Imaging Sci. 2021; 11: 56. doi: 10.25259/ JCIS_100_2021. PMID: 34754596; PMCID: PMC8571355.