
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Mounier-Kuhn syndrome: A case report of a 64-year-old male followed up after 8 years of the first diagnosis
Dil Afrose1; Pradeesh Sivapalan2,3*; Shailesh Balasaheb Kolekar1,3
1Department of Internal Medicine, Unit of Respiratory Medicine, Zealand University Hospital, Roskilde, Vestermarks Road 9, 4000 Roskilde, Denmark.
2Department of Medicine, Section of Respiratory Medicine, Herlev & Gentofte Hospital, Gentofte Hospital Road 1, 2900 Hellerup, Denmark.
3Department of Clinical Medicine, Faculty of Health and Medical Sciences, University of Copenhagen, Denmark.
*Corresponding Author : Pradeesh Sivapalan
Department of Medicine, Section of Respiratory
Medicine, Herlev & Gentofte Hospital, Gentofte
Hospital Road 1, 2900 Hellerup, Denmark.
Tel: +45 29 88 06 01,
Email: pradeesh.sivapalan.02@regionh.dka
Received : Jan 28, 2024
Accepted : Feb 26, 2024
Published : Mar 04, 2024
Archived : www.jcimcr.org
Copyright : © Sivapalan P (2024).
Abstract
Mounier-Kuhn Syndrome (MKS) is a rare congenital disorder characterized by the abnormal dilatation of the major airways, namely trachea and stem bronchi. It can be presented as the recurrent lower respiratory tract infection. Symptoms may vary from being asymptomatic to a wide range of infections which may lead to severe respiratory failure. Diagnosis can be performed by the means of computed tomography and bronchoscopy. The treatment is primarily symptomatic and supportive. Herein, we have presented a case of a 64-years old man, ex-smoker, who was referred after 4 episodes of antibiotic treated pulmonary infection. He was previously diagnosed with tracheobronchomegaly through CT scan in 2015. We have compared the lung function test and the radiological features between two time slots being 8 years apart (2015-2023), that showed insignificant change.
Keywords: Mounier-Kuhn syndrome; Tracheobronchomegaly; Computed tomography; Lung function test; Chest X-ray; Rare lung disease.
Abbreviations: MKS: Mounier-Kuhn Syndrome; Bpm: Beat Per Minute; CT: Computed Tomography; HRCT: High Resolution Computed Tomography; FEV1: Forced Expiratory Volume in 1st Second; FVC: Forced Vital Capacity; PFT: Pulmonary Function Test.
Citation: Afrose D, Sivapalan P, Kolekar SB. Mounier-Kuhn syndrome: A case report of a 64-year-old male followed up after 8 years of the first diagnosis. J Clin Images Med Case Rep. 2024; 5(3): 2895.
Introduction
Mounier-Kuhn syndrome was named after Mounier Kuhn P, who described the disease first in 1937 [1]. The MKS was first visualized in computed tomography in 1987. The MKS has been significantly higher prevalent in men with an 8:1 male to female ratio [2]. The average diagnosis age of patients between 30 to 60 years [3]. While the exact cause of MKS is still to be revealed, smoking and pollutants may be deemed as the aggravating factors which cause airway inflammation [3]. MKS is a rare congenital disorder, characterized by the thinning of smooth muscle layer and atrophy or absence of elastic fibres in the trachea and main bronchi [3]. Chronic cough with sputum production in the form of recurrent lower respiratory tract infections trademark the clinical picture [4]. Patients often being asymptomatic to MKS, are diagnosed incidentally with other diseases. Progression is variable, from bronchiectasis, emphysema to severe respiratory failure. The confirmatory diagnosis is made by radiological imaging. As an irreversible disease, there is no curative treatment [5].
Case presentations
A 64-year-old male, with BMI 24 Kg/m2 , presented to the lung medicine outpatient as a referral from a general practitioner. He had smoked 23 pack years and stopped smoking at the age of 36. He has no significant occupational history of exposure to hazardous chemicals, dusts, and fibers. He presented with a history of recurrent productive cough from childhood but no family history of congenital, lung or infectious diseases. He has a history of recurrent respiratory tract infection (2-3 times per year) until the age of 57, when he was admitted to hospital with respiratory infection for 1 month in 2015. There he was diagnosed with tracheobronchomegaly together with cystic bronchiectasis radiologically, with good ventilation capacity. He was followed up until after 3 years with no significant pulmonary event, and Bronchodilator and prophylactic antibiotics were not advised. After 8 years, in 2023, he was referred to us after 4 episodes of antibiotic treated pulmonary infection and 2 episodes of hospitalization due to pneumonia, in the last 2 years. Upon presentation, he had complained of progressive cough with mucoid sputum that became purulent during infectious exacerbations, respiratory distress MRC-2 with physical stress and in winter. There was no history of haemoptysis, nasal blockage, loss of sense of smell, voice change, dysphagia, fever, chest pain, weight loss or night sweats. Patient reported no history of loud snoring, he had no episodes of gasping for air during sleep and no history of somnolence.
The clinical examination reveals respiratory rate under 16, pulse 74 bpm, oxygen saturation 96%. There was no evidence of clubbing, jaundice, anaemia, dehydration, dependent oedema or lymphadenopathy. There were no rashes or evidence of peripheral stigmata of connective tissue disease. Patient presented with good oral hygiene and there was no sign of oral candida or mouth ulcer. On auscultation, his chest was clear with good bilateral air entry, and no evidence of wheeze or crackles. Heart sounds were normal.
Full blood cell count, electrolytes, C-reactive protein, liver and renal function tests and immunoglobulin levels (IgA, IgG, IgM, IgG-subclasses) were all within normal ranges with no clinically significant abnormalities. Bacteriological and virological tests of the sputum showed no growth. Table 1 shows a comparison spirometry parameter between 2015 and 2023.
Table 1: Comparison of the spirometry between 2015 and 2023. *LLN (lower Limit of Normal range).
| Parameters | 2015 | 2023 | |||||||
|---|---|---|---|---|---|---|---|---|---|
| % of expected | LLN (Best) | Before Salbutamo |
% of expected | LLN (Best) | After Salbutamol |
% of expected |
Change in % of expected |
||
| FEV1 (L) | 4.85 | 151 | 3.4 | 4.26 | 139 | 2.26 | 4.23 | 138 | -1 |
| FVC (L) | 5.5 | 137 | 4.28 | 5.27 | 132 | 2.99 | 5.09 | 128 | -3 |
| FEV1/FVC (%) | 88% | 115 | 79 | 80.88 | 105 | 64.42 | 83.02 | 108 | -3 |
| FEF50 (L/s) | 5.61 | 137 | 1.91 | 5.8 | 142 | -3 | |||
| PEF (L/s) | 11.02 | 141 | 5.8 | 10.59 | 136 | -4 | |||
| VC MAX (L) | 5.27 | 135 | 2.98 | 5.09 | 130 | -3 | |||
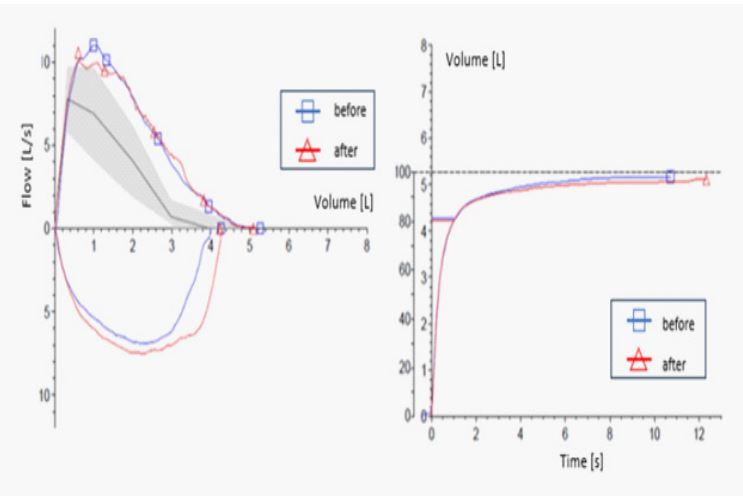
Pulmonary Function Test (PFT) in 2015 showed that, the patient had a good ventilation capacity with Forced Expiratory Volume (FEV1), Forced Vital Capacity (FVC) and the ratio FEV1/ FVC of 151%, 137% and 115% of the expected values respectively. Whereas the measured value in 2023, showed no notable changes of the PFT parameters as recorded before and after the administration of Salbutamol. Therefore, body plethysmography was not conducted. Other PFT values: total lung capacity and residual volume in 2015 were 8.16 and 2.56 which are 124% and 113% of the respective expected values. These values were not recorded in 2023. Figure 1 shows spirometry and bronchodilator reversibility test with Salbutamol in 2023. No obstructive changes and good ventilation capacity even after bronchodilator inhalation is seen.
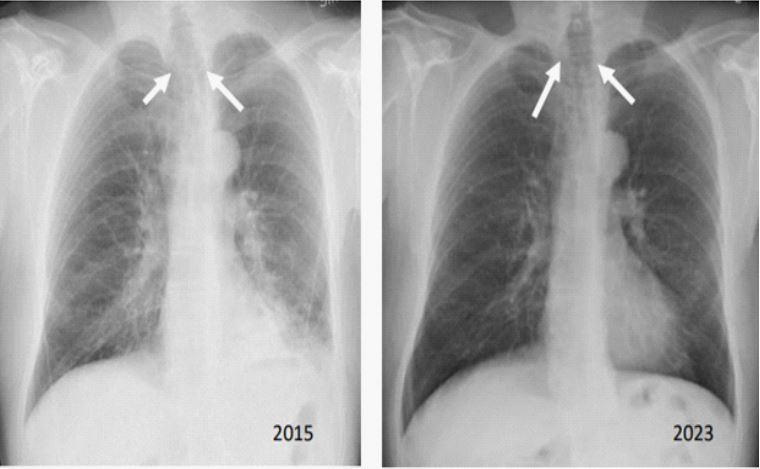
Chest X ray shows tracheobronchomegaly with discrete reticular and small nodular thickenings laterally pericardially in the left lung, there is thickening of the bronchial walls basally on the left side and suspected bronchiectasis. There is no widening of the cardiac shadow, neither signs of pulmonary stasis nor pleural effusion. Compared to the corresponding previous chest X-ray, it remained unchanged for eight years, shown in Figure 2.
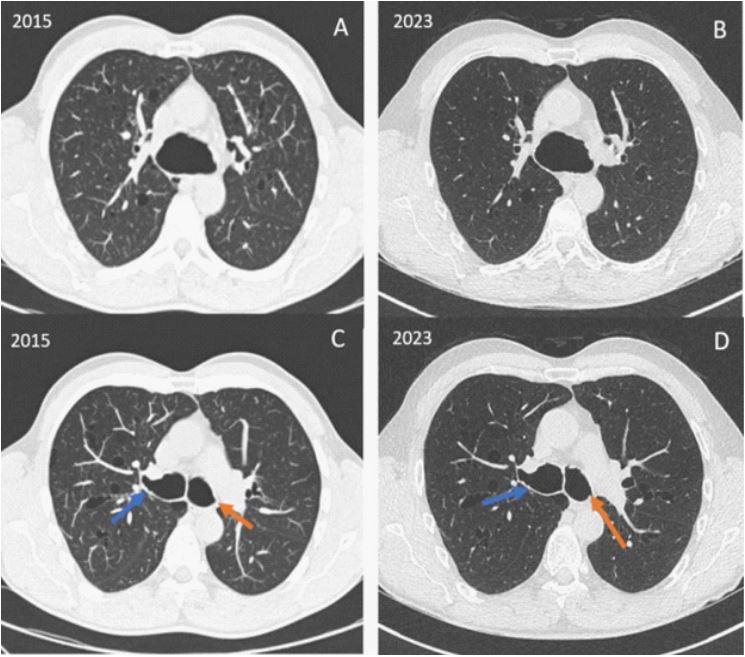
High-Resolution Computed Tomography (HRCT)shows,
• Moderately ectasia of trachea and main bronchi, diameter of trachea measuring approx. 5 cm, left main bronchus approx. 2.3 cm and right main bronchus approx. 3 cm - remain unchanged from 2015 to 2023. As shown in Figure 3 - this corresponds to the primary feature of Mounier-Kuhn syndrome.
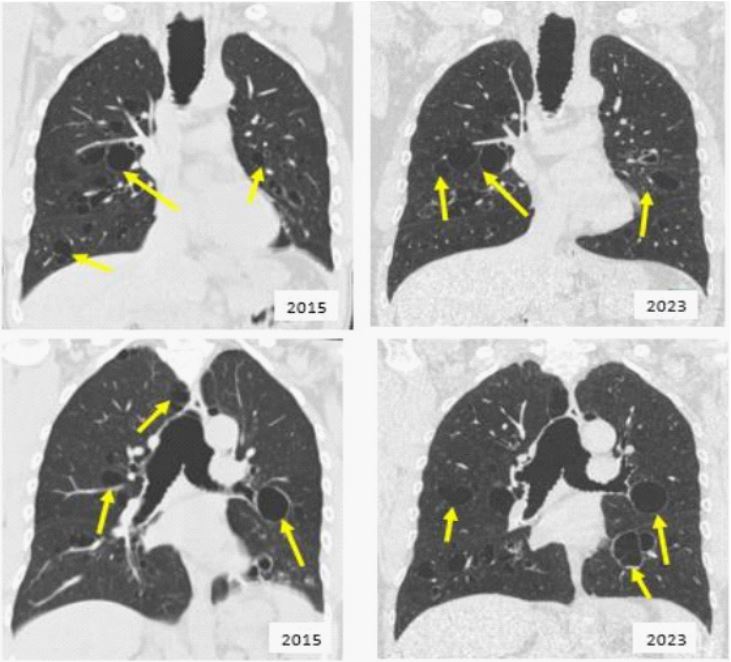
• Numerous cystic bronchiectasis, which hang as thinwalled bags from bronchial branches and have diameters up to approx. 40 mm -remain unchanged.
• Mild apical para-septal emphysema – remain unchanged, as shown in Figure 4.
• There is good air exchange without air trapping.
• No pleural change or accumulation.
• No pathologically enlarged lymph node.
He is a father of 4 children, none of them have a history of recurrent respiratory infection. All of them have normal Monoclonal B Lymphocytosis (MBL) amounts and genetic analysis for genetic cystic disease is without evidence and HRCT of the children showed no sign of tracheobronchomegaly. The patient shows no progression of disease both clinically and radiologically over 8 years, except for the episodes of acute exacerbation in the form of infection, which is one of the common clinical features of MKS.
As an outpatient, the patient was treated with tiotropium bromide inhalation, a Long-acting anticholinergic drug to prevent further deterioration of respiratory distress and azithromycin 250 mg 3 times a week as prophylaxis to prevent further infection and use the PEP (Positive Expiratory Pressure) device that helps to move the mucus into the larger airway. The effect of azithromycin will be evaluated and adjusted during the next visit scheduled after 6 months. The patient was contacted after two months of the last visit. The patient reported no further progression or any episode of exacerbation. Patient further reported that he has been leading his habitual lifestyle. The patient was requested to follow -up after 6 months or any progression of symptoms e.g., dyspnoea, sign of infection.
Discussion
Mounier-Kuhn Syndrome (MKS) is a rare clinical and radiological entity characterized by markedly dilated trachea and bronchi associated with diverticula. Histological hallmark of MKS is atrophy of longitudinal muscle and elastic fibers and thinning of muscularis mucosa by trachea and main bronchi [6]. Numerous saccular diverticula between cartilages and pooling of secretion in it along with abnormal airway dynamics predispose to development of chronic pulmonary infection, bronchiectasis, emphysema and pulmonary fibrosis [2]. Aetiology of the tracheobronchomegaly is not well known. Congenital as well as autosomal recessive disorder of MKS has been reported [2]. Mechanical ventilation especially for preterm neonates, pulmonary fibrosis, and radiotherapy are the acquired causes of tracheobronchomegaly. Exposure to certain irritants of the bronchial membrane, tobacco as well as industrial and occupational pollution are possible factors in the development of this disease [7,8].
MKS has been reported to be associated with Ehlers-Danlos syndrome, cystic fibrosis, Marfan’s syndromes and cutis laxa [8], Kenny-Caffey syndrome, and Brachmann-de Lange syndrome as well as rheumatologic disorders – ankylosing spondylitis and rheumatoid arthritis [3]. The genetic analysis for cystic fibrosis of the patient and his children showed no evidence for this disease. Symptomatology is non-specific and primarily related to the infectious complications of the disease. Clinical features vary from asymptomatic with preserved lung functions to severe consequences of respiratory infections to death [9]. Patients may have a history of respiratory infection since childhood with infective exacerbations 2 to 3 per year. The cough may be dry or productive with purulent sputum, often associated with haemoptysis [3]. Finger clubbing is common, and wheezing can be heard upon auscultation during exacerbation of MKS. MounierKuhn syndrome may also include sino-nasal polyposis, bilateral ptosis, epicanthus, micrognathism and excess skin of the upper lip [10]. Fever with cough and excessive purulent sputum, tachypnoea and tachycardia indicate acute exacerbation, while recurrent infection, exertional dyspnoea and respiratory failure indicate progression of disease. The reported patient has a history of frequent childhood pulmonary infection and presented to us with productive cough but no sign of infection. There was no sign of acute exacerbation or progression of disease at presentation.A wide range of pulmonary and nonpulmonary clinical consequences associated with MKS. The frequent pulmonary complications are bronchiectasis, bullous emphysema [11], recurrent pneumonia, tracheobronchomalacia and aspergillosis and infection with atypical organisms, including tuberculous and non-tuberculous mycobacteria [3]. Pneumothorax is caused by bullous emphysema in MKS [3]. GERD is the most common non-pulmonary complication of MKS. Patients mainly die of progressing respiratory failure or acute respiratory failure due to pulmonary embolism and subsequent nosocomial pneumonia [12].
The diagnosis of MKS is made by an image examination. Diagnosis is confirmed by measurement of the trachea, can be made by a chest x-ray but High-Resolution Computer Tomography (HRCT) is the gold standard [13]. Chest radiographs show dilatation of the trachea and bronchi; irregularly corrugated or scalloped appearance of the air columns with associated complications of diverticula, bronchiectasis as well as infections [14]. Measurement of trachea and main bronchi can be made by CT. MKS in adults, the CT diagnostic criteria are the diameter of the trachea increases beyond 30 mm and/or the diameter of the right and left main bronchus increases beyond 18 and 21 mm respectively [13]. In presenting case, the diameter of the trachea measuring approx. 5 cm, left main bronchus approx. 2.3 cm and right main bronchus approx. 3 cm, thus fulfilling primary features of tracheobronchomegaly in MKS (Figure 3). Bronchoscopy shows proximal airway dilation, the expiratory collapse due to tracheomalacia, tracheal and bronchial diverticula, extent of the lesion and retained secretion [14]. Retention of secretion may cause chronic infection, bronchiectasis and pulmonary fibrosis.
Lung function tests using spirometry supplements the diagnosis. The reversibility test with a bronchodilator is often done to reveal a range of obstructiveness. Result of lung function test may range from normal to varying degree of obstructive ventilation defect [15]. Spirometry results in presenting case shows good ventilation capacity with no obstructive features. This finding corroborates the case report by Mostafa et al. who also reported normal PFTs [16]. The differential diagnosis are mainly laryngocele, pharyngocele, Zencker’s diverticulum, pulmonary hernia, bullous emphysema and Williams-Campbell syndrome [17]. In laryngocele, pharyngocele, Zencker’s diverticulum, there is no tracheal diverticula [17]. In apical pulmonary hernia and bullous emphysema, the trachea and bronchi are intact [11]. Williams-Campbell syndrome is characterized by congenital bronchiectasis cysts resulting from a deficiency of cartilage in the fourth and sixth order bronchi. In this syndrome, the trachea and the main bronchi are of normal diameter [6,17].
MKS has no specific treatment guideline. Asymptomatic patients required no specific treatment. Cessation of smoking and minimizing exposure to industrial or occupational pollutants is proved conducive [14]. The pneumococcal polysaccharide and influenza vaccines are recommended regardless of age or symptoms at diagnosis [3]. Choosing antibiotics in acute exacerbations of MKS should be according to guidelines for non-cystic fibrosis bronchiectatic disease and lower respiratory tract infections [3]. Pulmonary physiotherapy including massage and postural drainage for clearing secretion and using of mucolytic agents are proved to be helpful [3]. long-term continuous positive airway pressure, airway stenting [1], surgical tracheoplasty and laser treatment [18] seem to be beneficial in some cases [5]. A double lung transplant was performed for the first time in 2005 in a patient of MKS [19], though there is no documented benefit.
Conclusion
• Munier-Kuhn syndrome is a rare respiratory condition. Symptoms can be mistaken with other chronic pulmonary conditions, e.g., chronic bronchitis, bronchiectasis- until imaging more precisely computed tomography is used to diagnose it.
• Though there is no definitive treatment, control and prevention of recurrent infections will prevent further deterioration. Patients should be followed up in a regular interval regardless of symptom to reduce morbidity.
• As shown in the present case, the pulmonary parameters and chest CT have not been changed over the period of 8 years, this attest to the fact that MKS can be kept stable with chest physiotherapy, prevention of infection and periodical followups.
Declarations
Acknowledgements: The patient in this case report was informed for the publishing of case details and accompanying images.
Funding: None.
Conflict of interest: None.
References
- MKP. Dilatation de la trachee; constatations radiographiqueset bronchoscopiques. Lyon Med. 1932; 150: 106.
- R F Johnston, RA Green. Tracheobronchiomegaly. Report Of Five Cases and Demonstration of Familial Occurrence. Am Rev Respir Dis. 1965; 91: 35-50, Jan. doi: 10.1164/arrd.1965.91.1.35.
- E Krustins, Z Kravale, and A Buls. Mounier-Kuhn syndrome or congenital tracheobronchomegaly: a literature review. Respir Med. 2013; 107(12): 1822-1828. doi: 10.1016/j.rmed.2013.08.042.
- SH S1 and K Utpat2. Rare Association of Mounier-Kuhn Syndrome With Panlobular Emphysema,” Journal of Evidence based Medicine and Healthcare. 2017; 4(6): 1-3.
- M Rjimati, M Serraj, M Elbiaze, MC Benjelloun, and B Amara. Mounier-Kuhn syndrome (Tracheobronchomegaly): Radiological diagnosis, Radiol Case Rep. 2021; 16(9): 2546-2550. doi: 10.1016/j.radcr.2021.06.021.
- I Katz, M Levine, and P Herman. Tracheobronchiomegaly. The Mounier-Kuhn syndrome. Am J Roentgenol Radium Ther Nucl Med. 2021; 88: 1084-1094.
- Mounier-Kuhn Syndrome: Report of 8 Cases of Tracheobronchomegaly with Associated Complications. Accessed. 2023. [Online]. Available: https://sma.org/article/.
- AA Wanderer, EF Ellis, RW Goltz, and EK Cotton. Tracheobronchiomegaly and acquired cutis laxa in a child. Physiologic and immunologic studies. Pediatrics. 2021; 44(5): 709-715.
- DD Odell et al., Airway stenting and tracheobronchoplasty improve respiratory symptoms in Mounier-Kuhn syndrome. Chest. 2011; 140(4): 867-873. doi: 10.1378/chest.10-2010.
- JH Woodring, RS Howard, and SR Rehm. Congenital tracheobronchomegaly (Mounier-Kuhn syndrome): a report of 10 cases and review of the literature. J Thorac Imaging. 1991; 6(2): 1-10.
- SF Boushy, R Kohen, DM Billig, and MJ Heiman. Bullous Emphysema: Clinical, Roentgenologic and Physiologic Study of 49 Patients. Diseases of the Chest. 1968; 54(4): 327-334. doi: 10.1378/chest.54.4.327.
- JA Ker and H Prinsloo. Tracheobronchomegaly associated with recurrent pneumonia,” Trop Doct. 2000; 30(4); 242-243. doi: 10.1177/004947550003000423.
- MG Dunne and B Reiner. CT features of tracheobronchomegaly,” J Comput Assist Tomogr. 1988; 12(3): 388-391. doi: 10.1097/00004728-198805010-00004.
- D Babirye, J Walubembe, JA Babirye, JB Baluku, P Byakika-Kibwika, and E Nabawanuka. Tracheobronchomegaly (Mounier-Kuhn Syndrome) in a 43-Year-Old Male: A Case Report. IMCRJ. 2022; 15: 631-637. doi: 10.2147/IMCRJ.S386083.
- E Krustins. Mounier-Kuhn syndrome: a systematic analysis of 128 cases published within last 25 years. Clin Respir J. 2016; 10(1): 3-10. doi: 10.1111/crj.12192.
- M Ghanei, M Peyman, J Aslani, and N Zamel. Mounier-Kuhn syndrome: a rare cause of severe bronchial dilatation with normal pulmonary function test: a case report. Respir Med. 2007; 101(8): 1836-1839. doi: 10.1016/j.rmed.2007.02.005.
- L Loued, et al. Mounier-Kuhn syndrome: A variable course disease. Respiratory Medicine Case Reports. 2020; 31: 101238. doi: 10.1016/j.rmcr.2020.101238.
- H Dutau, F Maldonado, DP Breen, and A Colchen. Endoscopic successful management of tracheobronchomalacia with laser: apropos of a Mounier-Kuhn syndrome. European Journal of Cardio-Thoracic Surgery. 2011; 39(6): 186.
- AJ Drain, et al. Double lung transplantation in a patient with tracheobronchomegaly (MounierKuhn syndrome). J Heart Lung Transplant. 2006; 25(1): 134-136, Jan. doi: 10.1016/j.healun.2005.06.018.