
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Series - Open Access, Volume 5
Computed tomography imaging features of hepatic perivascular epithelioid cell tumor: A report of two cases and Review of the Literature
Yi-xiang Li1,2,3,4; Wei-long Lv1,2,3,4; Li-li Wang1,2,3,4; Meng-meng Qu1,2,3,4; Jun-qiang Lei1,2,3,4*
1The First Clinical Medical of Lanzhou University, Lanzhou, China.
2Department of Radiology, The First Hospital of Lanzhou University, Lanzhou, China.
3Gansu Intelligent Imaging Medical Engineering Research Center, Lanzhou, China.
4Precision Image Collaborative Innovation Gansu International Science and Technology Cooperation Base, Lanzhou, China.
*Corresponding Author : Jun-Qiang Lei
The First Clinical Medical of Lanzhou University,
Lanzhou, 730000, China.
Email: leijq1990@163.com
Received : Jan 29, 2024
Accepted : Feb 26, 2024
Published : Mar 04, 2024
Archived : www.jcimcr.org
Copyright : © Jun-Qiang L (2024).
Abstract
Background: Perivascular Epithelioid Cell tumor (PEComa) is an uncommon tumor of mesenchymal origin which can arise at a variety of visceral and soft tissue sites, most frequently in the uterus whereas particularly uncommon in liver,only 8% of PEComa cases. Here, we present two pathologically proven cases of PEComa of the liver, retrospectively discuss the clinical, imaging, histological features and review the literature.
Case presentation: Case 1: A 54-year-old female patient with intermittent epigastric discomfort for 2 years and aggravated for 5 days.The laboratory examinations were normal. Computed Tomography (CT) showed the lesions were located on the right lobe. The discomfort had resolved after surgery and PEComa was diagnosed after pathological examination of the surgical specimen. The patient has been followedup for 5 years without recurrence. Case 2: A 30-year-old woman was found to have a mass of liver incidentally during regular physical examination after breast cancer surgery. On contrast enhancement CT, a well demarcated mass was found. After operation, pathological diagnosis was established as malignant PEComa of the right liver. Neither primary recurrence nor metastasis was found during the 2-year follow-up.
Conclusion: The CT imaging manifestations of liver PEComa have certain characteristics. When the tumor density is not uniform or contains fat, and thickening vascular shadow appears around the lesion, combined with clinical and laboratory examination, suggestive diagnosis can be made.
Keywords: Computed tomography; Hepatic; Imaging; Pecoma; Perivascular epithelioid cell tumor.
Citation: Yi-xiang L, Wei-long L, Li-li W, Meng-meng Q, Jun-qiang L. Computed tomography imaging features of hepatic perivascular epithelioid cell tumor: A report of two cases and Review of the Literature. J Clin Images Med Case Rep. 2024; 5(3): 2896.
Background
PEComa is a rare stromal tissue-derived tumor [1], which show perivascular epithelioid cell differentiation, and the incidence is rising. The World Health Organization defines PEComa as a family of related mesenchymal neoplasms which share a distinctive cell type, the perivascular epithelioid cell or “PEC’ (which was morphologically described first in 1944 by Apitz and it was designated as an “abnormal myoblast” in renal angiomyolipoma, but there is no known normal tissue counter part). In 1996, Zamboni [2], put forward the concept of PEComa for the first time, and four years later, the case report of PEComa of the liver was first reported by Yamasaki [3]. The “family” now includes angiomyolipoma, lymphangiomyomatosis, clear cell “sugar” tumor of the lung, and a group of rare, morphologically and immunophenotypic lesions that are simply termed PEComa [4]. This tumor always composed of nests and sheets of usually epithelioid but occasionally spindled cells with clear to granular eosinophilic cytoplasm and a focal connection with blood vessel walls. In a word, the origin and function of PEComas system still need to be further studied. More and more reports have demonstrated different anatomical sites of these lesions, including vagina [5], kidneys, bladder, prostate, lungs, pancreas and liver [6]. Compared to other liver tumors, these lesions are uncommon and difficult to identify. But due to the development of diagnostic procedures and there are characteristic immunohistochemicall indicators to confirm the diagnosis, we now diagnose PEComa more often. Our cases add to the volume of primary hepatic PEComas, and contribute to increase awareness and understanding of this rare tumor. At the same time, the information we provided is useful for summarizing the CT features of this kind of tumors. It should be included in differential diagnoses from common hypervascular neoplasms of liver.
Case presentations
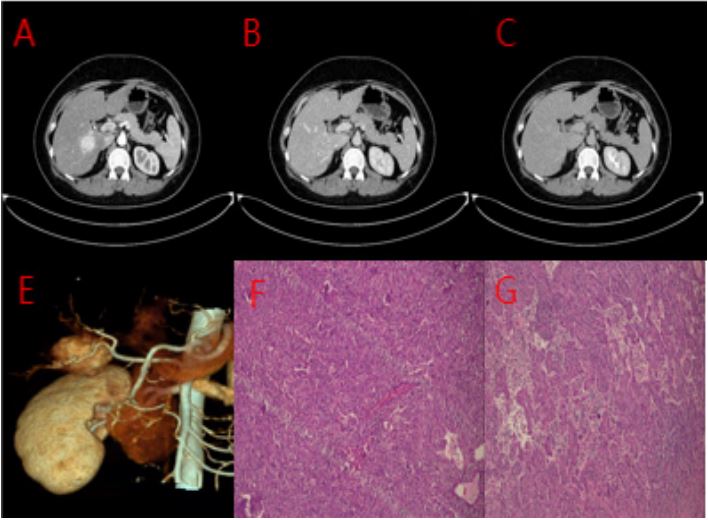
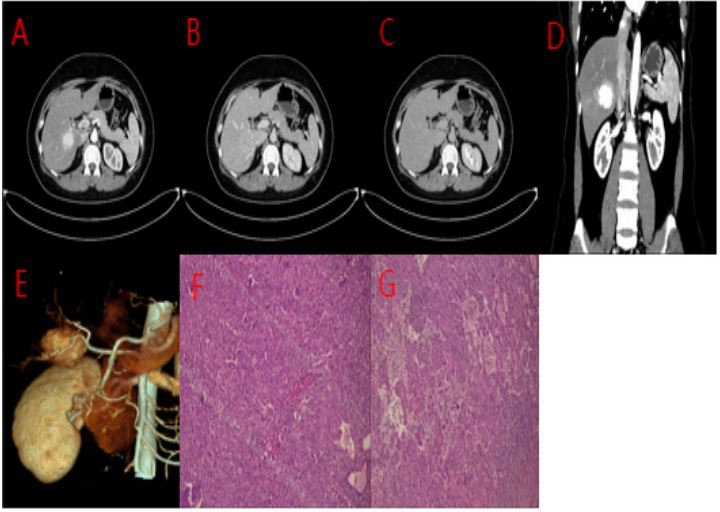
Case 1: A 54-year old previously healthy female was referred to a gastroenterologist for unspecific pain in the lower abdominal region. The physical examination was normal and the levels of laboratory tests were within reference ranges. The patient had a nonsignificant past medical history, no history of recent illness and/or trauma and was not receiving any medication at the time of referral. An abdominal Computed Tomography (CT) scan revealed a circular, space-occupying lesion with a maximum diameter of 6.8×5.0 cm. The lesion was localized primarily in segment 5 of the right lobe that was hypodense on a normal scan with apparent early arterial phase enhancement and delayed-phase washout. No portal vein tumor thrombus and retroperitoneal enlarged lymph nodes were found, and there was no obvious invasion of the surrounding organs. Immunohistochemistry: ki67 (<5%), CD34 (vascular rich), Vimentin (1+), HMB (2+). Pathological diagnosis: perivascular epithelioid cell tumor (PEComa). The patient has been followed-up for 5 years without recurrence.
Case 2: A 30-year-old woman was found to have a mass of liver incidentally during regular physical examination after breast cancer surgery. The patient did not show any symptom-related discomfort or history of hepatitis B or C, cirrhosis background, and alcohol abuse. The laboratory tests including blood routine, liver, and renal function, and tumor biomarkers including AFP, CEA, and CA19–9 were found to be within the normal range. On contrast enhancement CT, a well demarcated mass, sized 2.4 cm × 3.1 cm, was found with significant and uniform enhancement in the Arterial phase. There was no evidence of fatty density, calcification and necrosis in the mass. Liver metastasis of breast cancer was considered before operation. Immunohistochemistry: CD31 (vascular+), CD34 (vascular +), SMA (partial+), Smur100 (adipocyte +), ki67 (>5%), Vimentin (1+), HMB (1+), CD117 (focus+), Melan-A (1+). After operation, pathological diagnosis was established as malignant PEComa of the right liver. Neither primary recurrence nor metastasis was found during the 2-year follow-up.
Table 1: The authors, age, gender, location, size, enhanced CT imaging features, symptom, whether it contains fat, immunohistochemistry and preoperative diagnosis of 37 cases of hepatic perivascular epithelioid cell tumor.
| Authors | Age | M/F | Location | Size (cm) |
Enhanced CT imaging features |
Symptom | Fat ingredients |
HMB-45 | SAM | Melan-A | PD |
|---|---|---|---|---|---|---|---|---|---|---|---|
|
Yi-xiang Li [our case] |
54 | F | S5 | 6.8 | Washout pattern |
Intermittent epigastric discomfort |
Yes | + | + | + | AML |
| 30 | F | S6 | 3.1 | Washout pattern |
Asymptomatic | No | + | + | + |
Metastatic carcinoma |
|
| Fang He [8] | 30 | F | S6 | 3.5 | UN | Asymptomatic | No | + | + | + | Hemangioma |
| Abigail Attard [9] | 69 | M | S6 | 4.5 | Washout pattern |
Non-specific abdominal discomfort |
No | + | + | + | HAML |
| Galera López [10] |
29 | F | S2 | 1.3 | UN | Asymptomatic | No | + | − | + | Hepatic adenoma |
| 27 | M | S6 | 3 | UN | Asymptomatic | No | + | + | + | UN | |
|
Naotake Funamizu [11] |
50 | F | S2 | 2 | Washout pattern |
Abdominal discomfort | No | + | − | + | HCC |
| Rok Dežman [12] | 24 | F | S4 | 2.5 |
Persistent enhancement |
Unspecific pain in the lower Abdominal region |
No | + | − | + | FNH |
| Xu Han [13] | 36 | F | S8 | 3.7 | Washout pattern |
Abdominal distention, cramps, and low-grade fever |
No | + | + | + | Metastasis |
| Yin Zhi Lan [14] | 40 | F | S4 | 9.4 |
Persistent enhancement |
Asymptomatic | Yes | + | − | − | UN |
| S5 | 5 | UN | − | − | + | − | − | UN | |||
| S6 | 2.5 | UN | − | − | + | − | + | UN | |||
| Daren Liu [15] | 25 | F | S7 | 1.8 | Washout pattern |
An abdominal mass | No | + | + | + | UN |
|
Toshiya Mae- bayashi [16] |
58 | M | S3 | 4.5 | Washout pattern |
Abdominal bloating | No | + | + | + | Inflammatory |
|
Hassania Ameurtesse [17] |
63 | F | S4 | 8 | UN |
Atypical pain in the right upper Abdominal quadrant |
No | + | + | + | UN |
| Dongmei Yu [18] | 41 | F | S6 | 1.9 | Washout pattern |
Fever, nausea, and slight upper abdomen pain |
No | + | − | + | HCC |
| Wenying Chen [19] |
44 | F | RL | 2.9 | Unenhance- ment |
Abdominal discomfort | Yes | + | + | + | Cyst |
| 37 | F | LL | 1.7 | Washout pattern |
Emaciation | Yes | + | + | + | HCC | |
| 43 | M | LL | 5 | Washout pattern |
Asymptomatic | No | + | + | + | HCH | |
| 57 | F | S1 | 5 | Washout pattern |
Asymptomatic | No | + | + | + | HCC | |
|
Banerjee Abhirup [20] |
72 | F | S8 | 10 | UN |
Constant dull aching epigastric pain |
No | + | + | + | UN |
|
Federico Selvaggi [21] |
42 | M | between S5 and S8 |
7 | UN |
Dyspnea, temperature, Abdominal discomfort and weight loss. |
No | + | + | + | UN |
|
Jeremy R Parfitt [22] |
60 | F | RL | 14 | UN |
Right upper quadrant pain and tenderness |
No | + | − | + | HCC |
|
Carlos Eduardo Paiva [23] |
51 | F | RL | 0.8 | UN |
Pain in the left hypochondrium |
No | + | − | − | UN |
| Da Tang [24] | 32 | F | S5 | 6.5 |
Persistent enhancement |
Intermittent right upper quadrant pain |
No | + | + | − | HCC |
| Bao-Bin Hao [25] | 51 | F | S6 | 8 | Washout pattern |
Asymptomatic | Yes | + | + | + | FNH |
| 30 | F | S8 | 2.5 | Washout pattern |
Asymptomatic | Yes | + | + | + | HCC | |
| 25 | M | S6 | 8 | Washout pattern |
Asymptomatic | Yes | + | + | + | HCH | |
| Zu-Sen Wang [26] |
29 | F | S5 | 19 |
Persistent enhancement |
Liver cancer rupture | Yes | + | + | + | HCA |
|
Hadi Mohammad Khan [27] |
61 | M | S7 | 4.5 | Washout pattern |
Asymptomatic | No | + | − | − | UN |
|
Xiaogang Zhang [28] |
63 | F | RL | 3.5 | Washout pattern |
Asymptomatic | No | + | + | − | HCC |
| Faseeh Khaja [29] |
51 | F | RL | UN | Washout pattern |
Asymptomatic | No | + | − | + | UN |
| L-J Zhao [30] | 58 | M | RL | 6 | Washout pattern |
Abdominal distention | Yes | + | + | − | UN |
|
AdriaNo Mas- similiaNo Priola [31] |
36 | F | LL | UN |
Persistent enhancement |
Abdominal discomfort and progressive growth of an epigastric bulk |
No | + | + | + | UN |
|
Carlos Eduardo Paiva [32] |
51 | F | LL | 0.8 | UN |
Pain in the left hypo- chondrium |
No | + | − | − | Metastasis |
| Haitao Guan [33] | 40 | F | S8 | 7.5 | Washout pattern |
Asymptomatic | No | + | + | − | HCA |
| Hyun-Jin Son [34] |
56 | F | S5 | 4.5 | Washout pattern |
Asymptomatic | Yes | + | + | + | HCC |
| Sh Y Tay [35] | 51 | F | Between S2 and S3 |
9 | Washout pattern |
Asymptomatic | No | + | + | − | HCC |
| Tan To Cheung [36] |
51 | F | RL | 10 | Washout pattern |
Dull Abdominal pain in the right upper quadrant |
No | + | − | + | UN |
Discussion and conclusions
PEComas are rare mesenchymal tumors with unpredictable behavior, the etiology remains uncertain. They are characterized by epithelioid cells, which stain with melanocytic markers, associated with spindle cells reactive for smooth muscle markers, nearly all PEComas show immunoreactivity for both melanocytic (HMB-45 and/or melan-A) and smooth muscle (actin and/or desmin) markers [7], which is the key point of the final diagnosis. More specifically, these cells are immune to melanocytic markers, have an epithelioid appearance and a transparent eosinophilic cytoplasm, and show a perivascular distribution. This heterogeneity makes it difficult to diagnose by imaging, biopsy and other techniques before operation. Because of low morbidity, there is a lack of comprehensive understanding of this hepatic lesion.
We summarize literature published in English after researching PubMed online database and inclusion terms are “hepatic” and “PEComa.” Thirty-seven cases (39 lesions) were found with primary hepatic PEComas, including our present patient, from 30 articles (Table 1).
The patients’ median age is 44 years (range 24-72 years). The maximum diameter of the tumors ranged from 0.8 to 19 cm (mean 5.15 cm). PEComas show a marked female predominance, with a male-to-female ratio of 29:8. Twelve lesions are arising from the left lobe of the liver while rest lesions are from the right lobe (12/39). Usually, the vast majority of PEComas are solitary lesions (36/37), and only 1 case reported to have 3 lesions at initial diagnosis. In the past, it was considered to be a benign disease, generally exhibits an inert biological behavior. However, multifocality is also reported more frequently in cases involving malignant lesions. Since 2000, some studies have shown that PEComas can display characteristics of both benign and malignant tumors. What’s more, PEComas have a wide variety of presentations and behavior, recurrences or metastases can be observed in patients with tumors exceeding 5-7 cm in size in some studies [37,38]. Malignant PEComas originating from the liver can affect many abdominal organs simultaneously, including the omentum, resulting in massive bleeding into the peritoneal cavity. According to some histologic features such as growth pattern, size of the lesion, mitotic activity, necrosis, nuclear grade, and vascular invasion, PEComas have been divided into 3 prognostic categories—benign, uncertain malignancy potential, and malignant. But Criteria to define the biological behavior of these rare lesions have not been clearly defined. Currently, the most useful features to predict poor outcome are tumor size >5 cm, high nuclear grades, infiltrative growth patterns and cellularity, mitotic rate >1/50 High-Power Fields (HPF), necrosis, and vascular invasion, as proposed by Folpe in 2005 [39]. Therefore, clear diagnosis and early intervention is extremely important for the prognosis of patients, but diagnose them preoperative is difficult. First of all, PEComas are commonly asymptomatic [16/37], the symptoms (such as abdominal pain, increased tension of the abdominal wall, constipation, or signs of ileus) are always caused by other diseases or occur in cases involving very large PEComa lesions. For the hepatic PEComa, it is difficult to differentiate a benign tumor from malignant variant only in clinical manifestations. Secondly, the disease is not significantly associated with hepatitis and liver cirrhosis. Laboratory examinations in patients with PEComa don’t reveal any specific abnormalities, Serum AFP, carcinoembryonic antigen, and Ca19-9 concentrations are also within the normal ranges. The most important thing is that PEComas mimic features of other hepatic neoplasms. At present, there are no characteristic imaging findings. Tumors typically had welldefined borders and show uniform or uneven enhancement on arterial phases. Some of the lesions contain fat and malformed blood vessels. These imaging features are non-specific, similar to many other liver tumors, including Hepatocellular Carcinoma (HCC) and Focal Nodular Hyperplasia (FNH) among others, but the histological evaluation might provide valuable diagnostic information. The unique feature of PEComas is the coexpression of at least one smooth muscle and melanocytic markers. That is to say, these are identified immunohistochemically by the expression of Human Melanin Black-45 (HMB-45), Melan-A and Smooth Muscle Antigen (SMA) which are seen in the majority of tumors. Among them, HMB45 is the most sensitive indicator, because there is no expression in primary liver tumors except hepatoblastoma in children, but it is positive in almost all PEComas [40]. In our study, immunohistochemical staining results show that all lesions are positive for human melanoma black 45 (HMB45) stain. Other positive immunostains are also reported including smooth muscle actin (SMA) (26/37) and melan-A (29/37). The final diagnosis is established on histopathological and immunohistochemical studies that are the “gold standard.”
The differential diagnoses of PEComas at imaging are wide; therefore, it is difficult to reach definite diagnosis preoperatively. Many cases had mentioned imaging diagnosis was misleading to other diseases. Hence radiologists should promote cognition. If we focus on the CT imaging performances, PEComas with high arterial vascularization as a consequence of rich vascularization from the branches of the hepatic artery have been described. In diagnostic studies,for most patients, the lesions exhibited mass with heterogeneous low density in plain CT; at the same time, the tumor can be well-demarcated or ill-defined. Contrast-enhanced CT shows almost all hepatic PEComas were hyperenhanced in the arterial phase. In the portal venous phase, the lesions can present as a hyperenhanced, isoenhanced, or hypoenhanced tumor. In the delayed phase, the density of the neoplasms returned to an hypoenhanced or isoenhanced state. Although the presence of adipose tissue, which is easier to detect, is typical only for some PEComas [10/37]. According to previous diagnoses, when PEComa is blood-rich and contains adipose tissue, it should be differentiated from liposarcoma, steatosis of hepatocellular carcinoma and liver adenoma: (1) Primary liposarcoma of the liver is rare but more common in male patients, its imaging findings are difficult to distinguish from PEComa of the liver, but the fibrous septum within the tumor and a small amount of local fat components are helpful for the definite diagnosis. (2) The content of steatosis in HCC is very few, and the patient always has a history of hepatitis and liver cirrhosis. AFP increases generally, and it is easy to be complicated with necrosis, portal vein tumor thrombus, enlarged peripheral lymph nodes, which can be distinguished by clinical diagnosis. Typical manifestation of HCC on contrast-enhanced CT is a hypodense tumor which is markedly enhanced in the arterial phase with the contrast reagent drain out in the portal and equilibrium phases. Pseudocapsule can also be seen in most cases. (3) Hepatic adenomas contain true capsule and are prone to fatty necrosis, but they often occur in special populations and are common in young women with a long history of oral contraceptives. Typical imaging findings suggest homogeneous enhancement in arterial phase and prolonged mild enhancement with well-defined margin. Moreover, rupture and bleeding may occur for a larger HCA. When there is no fat density inside the mass, it is difficult to distinguish from a variety of liver diseases, so it needs to be considered according to clinical and laboratory information: (1) when PEComa did not show contrast “washout”, which overlap with features of benign, well vascularized tumors such as Focal Nodular Hyperplasias (FNH) and hemangiomas. These, however, should not be mistaken, as FNHs show very homogenous enhancement and in turn, hemangiomas have a typical blood pooling appearance, which both differ significantly from heterogenous enhancement of PEComas. CT imaging shows an ill-delineated, heterogeneously enhanced mass with a central star-like scar. The tumor has an early mild enhancement in arterial phase whereas marked enhancement in portal and equilibrium phases. The central scar appears hypodense in noncontrast CT and slightly delayed enhancement in equilibrium phase. (2) when the enhanced lesion showed “fast in and out”, it is often misdiagnosed as primary hepatocellular carcinoma which one’s some laboratory and clinical characteristics have been described before. However, the AFP value of PEComa of liver is generally not high, and the expression of HMB-45 is positive. But HCC is generally supplied by small hepatic artery, and the proportion of blood supply artery in the focus is relatively low, while PEComa is rich in twisted abnormally dilated thick-walled vessels, and strips and punctate vessels can be seen in the mass. This sign is of high value in differentiating the two neoplasms.
Hepatic PEComas are rare but increasingly recognized tumors. Still, there is a curiosity, and the diagnostic approach, treatment modalities, and the follow-up are faced with challenge. Due to the rarity and atypical symptoms of primary hepatic PEComa, it is easy to delay the timing of treatment, thus we presented two pathologically proven cases of PEComa of the liver and inspected the importance of thoughtful examination in the diagnosis of this lesion, and the necessity of a more sensible approach and broad investigation for the stratification of the biologic behavior of PEComas. In our study, the patients are females with no background of liver cirrhosis, the focuses were located in the right liver and had no typical clinical symptoms, which are in accordance with the epidemiological report. Above all, the natural history of primary hepatic PEComas is quite varied and not yet well established or predictable. Presentation ranged from a palpable abdominal mass to acute abdomen. Usual treatment is surgery for benign tumors and chemotherapy including mTOR inhibitors for malignant tumors. In short, for liver space-occupying lesions with no history of substantial liver disease, thickened and twisted blood vessels and negative tumor markers, the possibility of PEComa should be considered in addition to common diseases, but the identification of benign and malignant tumors should also be combined with pathological and immunohistochemical results. In view of the fact that the biological behavior of liver PEComa is not entirely known at present, long-term follow-up of postoperative patients is a necessary clinical management measure. Hopefully, further research will allow accurate prediction of the behavior of this lesion and establish firm criteria for discrimination between malignant and benign tumors. At the same time, further research into the etiology of PEComa may yield new drug targets for treating this distinctive tumor.
Declarations
Acknowledgements: We are grateful for surgery support Jun Wang and the personnel of the nursing department. This work was supported by grants from the The First Hospital of Lanzhou University, (Grant No. Ldyyyn2020-14).
Authors’ contributions: Yi-xiang Li, Wei-long Lv,Li-li Wang and Meng-meng Qu collected the data. Yi-xiang Li, Wei-long Lv and Jun-qiang Lei did the analysis and interpretation of data; Yi-xiang Li and Wei-long Lv conceptualized and wrote the manuscript. Grant to Clinical Foundation of the First Hospital of Lanzhou University financed this study. All the authors approved the version to be published.
Funding: Funding from the Clinical Foundation of The First Hospital of Lanzhou University, (No. Ldyyyn2020-14) is gratefully acknowledged.
Availability of data and materials: Data are available on request from the authors.
Ethics approval and consent to participate: This case was approved by the institutional ethical review board of The First Hospital of Lanzhou University of Science and Technology. Written informed consent for the present study was obtained from the patient.
Consent for publication: The manuscript has not been and will not be a podium or poster meeting presentation.
Competing interests: No potential conflict of interest relevant to this article was reported.
References
- Folpe AL, Kwiatkowski DJ. Perivascular epithelioid cell neoplasms: pathology and pathogenesis. Hum Pathol. 2010; 41(1): 1-15. doi: 10.1016/j.humpath.2009.05.011. Epub 2009 Jul 15. PMID: 19604538.
- Fletcher CDM, Bridge JA, Hogendoorn PCW, Mertens F. World Health Organization Classification of Tumours of Soft Tissue and Bone, 4th ed.; IARC Press: Lyon, France. 2013; 230-231.
- Zamboni G, Pea M, Martignoni G. Clear cell “sugar” tumor of the pancreas. A novel member of the family of lesions characterized by the presence of perivascular epithelioid cells. Am J Surg Pathol. 1996; 20(6): 722-30. doi: 10.1097/00000478-199606000-00010. PMID: 8651352.
- Yamasaki S, Tanaka S, Fujii H. Monotypic epithelioid angiomyolipoma of the liver. Histopathology. 2000; 36(5): 451-6. doi: 10.1046/j.1365-2559.2000.00848.x. PMID: 10792487.
- Gupta R, Hariprasad R, Dhanasekaran K, Gupta S. Malignant perivascular epithelioid tumor of the vagina: Report of a rare case with brief review of literature. Diagn Cytopathol. 2020; 48(5): 483-488. doi: 10.1002/dc.24402. Epub 2020 Mar 5. PMID: 32134210.
- Martignoni G, Pea M, Reghellin D, Zamboni G, Bonetti F. PEComas: The past, the present and the future.Virchows Arch. 2008; 452: 119-132.
- Dickson MA, Schwartz GK, Antonescu CR. Extrarenal perivascular epithelioid cell tumors (PEComas) respond to mTOR inhibition: clinical and molecular correlates. Int J Cancer. 2013; 132(7): 1711-7. doi: 10.1002/ijc.27800. Epub 2012 Sep 21. PMID: 22927055; PMCID: PMC3558545.
- He F, Xia Y, Ling X. Diagnosis and Individualized Treatment of Three Primary Malignant Tumors: A Case Report. Breast Cancer (Dove Med Press). 2021; 13: 519-527. doi: 10.2147/BCTT.S321390. PMID: 34526817; PMCID: PMC8437380.
- Attard A, Piscopo N, Schembri J, et al. A Rare Case of PEComa of the Liver. GE Port J Gastroenterol. 2021; 28(3): 217-221. doi: 10.1159/000509192. Epub 2020 Oct 5. PMID: 34056048; PMCID: PMC8138188.
- Galera López MDM, Márquez Rodas I et al. Simultaneous diagnosis of liver PEComa in a family with known Li-Fraumeni syndrome: a case report. Clin Sarcoma Res. 2020; 10(1): 24. doi: 10.1186/s13569-020-00143-7. PMID: 33292569; PMCID: PMC7684891.
- Funamizu N, Omura K, Osada H, etal. [Laparoscopic Hepatic Resection for a Hepatic Perivascular Epithelioid Cell Tumor-A Case Report]. Gan To Kagaku Ryoho. 2020; 47(8): 1229-1231. Japanese. PMID: 32829361.
- Dežman R, Mašulović D, Popovič P. Hepatic perivascular epithelioid cell tumor: A case report. Eur J Radiol Open. 2018; 5: 121-125. doi: 10.1016/j.ejro.2018.08.004. PMID: 30140716; PMCID: PMC6104347.
- Han X, Sun MY, Liu JH, et al. Computed tomography imaging features of hepatic perivascular epithelioid cell tumor: a case report and literature review. Medicine (Baltimore) 2017; 96: 9046.
- Lan YZ, Hua XE. Hepatic multiple perivascular epithelioid cell neoplasm: A case report and literature review. Mol Clin Oncol. 2016; 4(4): 619-621. doi: 10.3892/mco.2016.735. Epub 2016 Jan 22. PMID: 27073677; PMCID: PMC4812225.
- Liu D, Shi D, Xu Y, Cao L. Management of perivascular epithelioid cell tumor of the liver: A case report and review of the literature. Oncol Lett. 2014; 7(1): 148-152. doi: 10.3892/ol.2013.1689. Epub 2013 Nov 19. PMID: 24348838; PMCID: PMC3861588.
- Maebayashi T, Abe K, Aizawa T,et al. Improving recognition of hepatic perivascular epithelioid cell tumor: Case report and literature review. World J Gastroenterol. 2015; 21(17): 5432-41. doi: 10.3748/wjg.v21.i17.5432. PMID: 25954119; PMCID: PMC4419086.
- Ameurtesse H, Chbani L, Bennani A,et al. Primary perivascular epithelioid cell tumor of the liver: new case report and literature review. Diagn Pathol. 2014; 9: 149. doi: 10.1186/1746-1596-9-149. PMID: 25034830; PMCID: PMC4223599.
- Yu D, Tang S. Hepatic perivascular epithelioid cell tumor: a case report and review of the literature. Intern Med. 2013; 52(12): 1333-6. doi: 10.2169/internalmedicine.52.0144. PMID: 23774542.
- Chen W, Liu Y, Zhuang Y,et al.Hepatic perivascular epithelioid cell neoplasm: A clinical and pathological experience in diagnosis and treatment. Mol Clin Oncol. 2017; 6(4): 487-493. doi: 10.3892/mco.2017.1168. Epub 2017 Feb 16. PMID: 28413654; PMCID: PMC5374935.
- Abhirup B, Kaushal K, Sanket M,et al. Malignant hepatic perivascular epithelioid cell tumor (PEComa) - Case report and a brief review. J Egypt Natl Canc Inst. 2015; 27(4): 239-42. doi: 10.1016/j.jnci.2015.05.004. Epub 2015 Jun 10. PMID: 26071321.
- Selvaggi F, Risio D, Claudi R,et al.Malignant PEComa: a case report with emphasis on clinical and morphological criteria. BMC Surg. 2011; 11: 3. doi: 10.1186/1471-2482-11-3. PMID: 21272348; PMCID: PMC3042371.
- Parfitt JR, Bella AJ, Izawa JI,et al. Malignant neoplasm of perivascular epithelioid cells of the liver. Arch Pathol Lab Med. 2006; 130(8): 1219-22. doi: 10.5858/2006-130-1219-MNOPEC. PMID: 16879028.
- Paiva CE, Moraes Neto FA, Agaimy A,et al.Perivascular epithelioid cell tumor of the liver coexisting with a gastrointestinal stromal tumor. World J Gastroenterol. 2008; 14(5): 800-2. doi: 10.3748/wjg.14.800. PMID: 18205275; PMCID: PMC2684012.
- Tang D, Wang J, Tian Y,et al. Hepatic perivascular epithelioid cell tumor: Case report and brief literature review. Medicine (Baltimore). 2016; 95(51): 5572. doi: 10.1097/MD.0000000000005572. PMID: 28002331; PMCID: PMC5181815.
- Hao BB, Rao JH, Fan Y, et al. Hepatic perivascular epithelioid cell tumor in three patients. Hepatobiliary Pancreat Dis Int. 2016; 15(6): 660-664. doi: 10.1016/s1499-3872(16)60077-2. PMID: 27919857.
- Wang ZS, Xu L, Ma L,et al. Hepatic falciform ligament clear cell myomelanocytic tumor: A case report and a comprehensive review of the literature on perivascular epithelioid cell tumors. BMC Cancer. 2015; 15: 1004. doi: 10.1186/s12885-015-1992-4. PMID: 26698563; PMCID: PMC4690247.
- Khan HM, Katz SC, Libbey NP,et al. Hepatic PEComa: a potential pitfall in the evaluation of hepatic neoplasms. BMJ Case Rep. 2014; 2014: bcr2014204122. doi: 10.1136/bcr-2014-204122. PMID: 24907216; PMCID: PMC4054585.
- Zhang X, Wang L, Jiang Y, et al. Hepatic perivascular epithelioid cell tumors-not otherwise specified: a case report. Nan Fang Yi Ke Da Xue Xue Bao. 2014 Jan;34(1):1-4. PMID: 24463106.
- Khaja F, Carilli A, Baidas S, et al. PEComa: A Perivascular Epithelioid Cell Tumor in the Liver-A Case Report and Review of the Literature. Case Rep Med. 2013; 2013: 904126. doi: 10.1155/2013/904126. Epub 2013 Dec 29. PMID: 24489554; PMCID: PMC3891746.
- Zhao LJ, Yang YJ, Wu H, et al. Perivascular epithelioid cell tumor of the liver: a case report and literature review. Eur Rev Med Pharmacol Sci. 2013; 17(12): 1665-8. PMID: 23832736.
- Priola AM, Priola SM, Cataldi A, et al. Acute abdomen as an unusual presentation of hepatic PEComa. A case report. Tumori. 2009; 95(1): 123-8. PMID: 19366072.
- Paiva CE, Moraes Neto FA, Agaimy A, et al. Perivascular epithelioid cell tumor of the liver coexisting with a gastrointestinal stromal tumor. World J Gastroenterol. 2008; 14(5): 800-2. doi: 10.3748/wjg.14.800. PMID: 18205275; PMCID: PMC2684012.
- Guan H, Zou Y, Lv Y, et al. Hepatic perivascular epithelioid cell tumor treated by transarterial embolization plus radiofrequency ablation: A case report and literature review. Medicine (Baltimore). 2017; 96(22): e6969. doi: 10.1097/MD.0000000000006969. PMID: 28562547; PMCID: PMC5459712.
- Son HJ, Kang DW, Kim JH, et al. Hepatic perivascular epithelioid cell tumor (PEComa): a case report with a review of literatures. Clin Mol Hepatol. 2017; 23(1): 80-86. doi: 10.3350/cmh.2016.0034. Epub 2017 Mar 14. PMID: 28288506; PMCID: PMC5381835.
- Tay ShY, Lao WT, Chen ChL, et al. Contrast-enhanced ct and angiographic findings in hepatic perivascular epithelioid cell tumor. JBR-BTR. 2013; 96(5): 308-10. doi: 10.5334/jbr-btr.428. PMID: 24479295.
- Cheung TT, Trendell-Smith N, Poon RT. Primary perivascular epithelioid cell tumour (PEComa) of the liver. BMJ Case Rep. 2013; 2013: 013008706. doi: 10.1136/bcr-2013-008706. PMID: 23845671; PMCID: PMC3736252.
- Doyle LA, Argani P, Hornick JL. PEComa. InWorld Health Organization Classification of Tumours of Soft Tissue and Bone, 5th ed.;IARC Press: Lyon, France. 2020; 312-314.
- Martignoni G, Pea M, Reghellin D, Zamboni G, Bonetti F. PEComas: The past, the present and the future.Virchows Arch. 2008; 452: 119-132. [CrossRef]
- Folpe AL, Mentzel T, Lehr HA. Perivascular epithelioid cell neoplasms of soft tissue and gynecologic origin: a clinicopathologic study of 26 cases and review of the literature. Am J Surg Pathol. 2005; 29(12): 1558-75. doi: 10.1097/01.pas.0000173232.22117.37. PMID: 16327428.
- Hornick JL, Fletcher CD. PEComa: what do we know so far? Histopathology. 2006; 48(1): 75-82. doi: 10.1111/j.1365-2559.2005.02316.x. PMID: 16359539.