
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Review Article - Open Access, Volume 5
A detailed review of critical illness related to pregnancy
Misbahuddin Khaja1*; Abeer Qasim2; Kinnera Sahithi Urlapu3; Zaheer Ahmad Qureshi4
1Division of Pulmonary and Critical Care Medicine Bronx Care Health System, Attending Physician, Affiliated with Icahn School of Medicine at Mount Sinai1650 Grand Concourse Bronx, NY10457, USA.
2Department of Medicine Bronx Care Health System, Third year Internal Medicine Resident, Affiliated with Icahn School of Medicine at Mount Sinai 1650 Grand Concourse Bronx, NY 10457, USA.
3Department of Medicine Bronx Care Health System, Pulmonary Fellow, Affiliated with Icahn School of Medicine at Mount Sinai 1650 Grand Concourse Bronx, NY 10457, USA.
4Department of Medicine Bronx Care Health System, Attending Physician, Affiliated with Icahn School of Medicine at Mount Sinai 1650 Grand Concourse Bronx, NY 10457, USA.
*Corresponding Author : Misbahuddin Khaja
Division of Pulmonary and Critical Care Medicine,
Attending Physician, Bronx Care Health System.
Affiliated with Icahn School of Medicine at Mount
Sinai1650 Grand Concourse Bronx, NY10457, USA.
Tel: 347-967-7074, Fax: (718) 466-8184,
Email: drkhaja@yahoo.com
Received : Feb 12, 2024
Accepted : Feb 27, 2024
Published : Mar 05, 2024
Archived : www.jcimcr.org
Copyright : © Khaja M (2024).
Abstract
Critical illness during pregnancy refers to severe medical conditions that can endanger the health and life of the pregnant woman and the developing fetus. Using critical illness during pregnancy as a topic for a review article can provide valuable insights into the challenges, management strategies, and outcomes associated with high-risk pregnancies. Pregnancy is a unique and complex physiological state that can challenge obstetricians and intensivists. Despite the advances in prenatal care, certain critical pregnancy illnesses are associated with significant feto-maternal morbidity and mortality. Maternal complications arise from abnormalities in physiological changes of pregnancy. This section highlights the common yet severe pregnancy complexities, pathophysiology, clinical manifestations, diagnosis, and management in critical care settings to optimize maternal and fetal outcomes. Some of the frequently encountered critical pregnancy illnesses are preeclampsia, eclampsia, HELLP syndrome, amniotic fluid embolism, peripartum cardiomyopathy, placental abruption, postpartum hemorrhage, and ectopic pregnancy. Each condition is discussed separately, further insinuating the need for timely diagnosis and treatment. This article also reviews the current treatment strategies, including blood pressure management, supportive care, and surgical intervention in obstetric hemorrhage and rupture. Critical care in pregnancy warrants profound vigilance and an adept, intensive, multidisciplinary approach, as prompt recognition and intervention decrease mortality and carry lifelong implications for both the mother and child.
Keywords: Pregnancy; Critical illness; Preeclampsia; Eclampsia; Postpartum hemorrhage; Cardiac arrest.
Abbreviations: HEELP: Hemolysis Elevated Liver Enzyme Low Platelets; ICU: Intensive Care Unit; CO: Cardiac Output.
Citation: Khaja M, Qasim A, Urlapu KS, Qureshi ZA. A detailed review of critical illness related to pregnancy. J Clin Images Med Case Rep. 2024; 5(3): 2897.
Introduction & background
Critical illness is a rare yet severe risk associated with pregnancy. Intensive Care Unit (ICU) admission incidence rate is about 0.7 to 13.5 per 1000 deliveries, with most cases admitted after the mother has given birth [1]. The prevalence rate of critical care illness in ICU is between 100 to 900 per 100,000 gestations. However, the mortality rate ranges from 6 to 24 deaths per 100,000 live births in developed regions, most seen in developing countries, leading to 55-920 deaths per 100,000 live births [2]. Pregnant patients who are critically ill can also exacerbate preexisting illnesses, including Myasthenia gravis, valvar heart disease, e.g. Mitral stenosis, and many other diseases. Pregnancy can also lead to severe complications, including Acute Respiratory Distress Syndrome (ARDS), septic shock, and Pulmonary embolism requiring ICU admission [3]. Common illnesses that require ICU admission include Preeclampsia, Eclampsia, HELLP, Acute fatty liver, Peripartum cardiomyopathy, Peripartum hemorrhage, Amniotic fluid embolism, ectopic pregnancy, and Sheehan syndrome. Below is a brief discussion of each of the conditions. Critically ill obstetric patients appear to have a significant risk of dying of their critical illness and high infant mortality. With an increase in the birth rate, the challenge of caring for critically ill obstetric patients requires urgent attention. ICU management should be directed at optimizing maternal well-being, which will benefit the fetus by assessing maternal and fetal risk from continuing pregnancy and deciding if delivery/termination of pregnancy will improve outcomes.
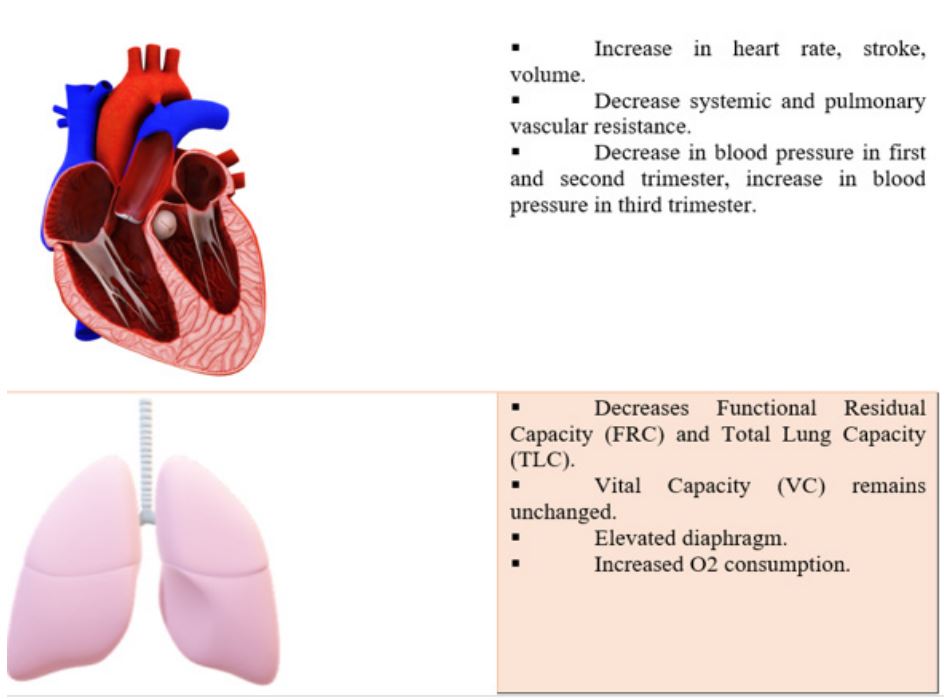
Normal physiology in pregnancy: Pregnancy causes physiologic changes in all maternal organ systems that return to normal after delivery. The cardiovascular changes include the heart rate and SV that increase to 30-50% from 4 to 6 l/min; during the first trimester, the Cardiac Output (CO) increases to 75% and maintains a plateau between 28- and 32 weeks’ gestation and remains same until the end of the pregnancy. As CO increases, it decreases systemic and pulmonary vascular resistance due to vasodilator effects [4]. During labor, CO increases another 30%. After delivery, the uterus contracts, and CO drops rapidly to about 15 to 25% above average, then gradually decreases (mainly over the next 3 to 4 weeks) until it reaches the pre-pregnancy level at about six weeks postpartum (Figure 1). Blood pressure will typically fall in the first trimester (down 10%) and second trimester (down 5%), with a slight 5% increase in the third trimester. During pregnancy, there are several respiratory changes. The Functional Residual Capacity (FRC) decreases by 10-15%, and the Total Lung Capacity (TLC) also reduces by about 5% due to the elevation of the diaphragm caused by the growing uterus. However, the Vital Capacity (VC) remains unchanged. Pregnant women are more susceptible to experiencing hypoxia, hyperventilation, and dyspnea than nonpregnant women. Gastrointestinal effects during pregnancy involve morning sickness, the most common symptom caused by elevated estrogen levels, progesterone, and human Chorionic Gonadotropin (hCG), resulting in nausea and vomiting. Typically, this symptom resolves within 14-16 weeks. Additionally, pregnancy increases gastric emptying time due to smooth muscle relaxation caused by higher progesterone secretion. Furthermore, progesterone induces dilation of the ureters, reducing ureteral tone. Also, the Renin-Angiotensin System (RAS) is activated during pregnancy, leading to increased Glomerular Filtration Rate (GFR) and renal plasma flow. GFR rises by 50% and remains elevated until delivery. The hematological effects of pregnancy result in an increase in both plasma and red blood cell volume, leading to dilution anemia. While the concentration of platelets decreases, the count remains the same. Moreover, levels of fibrinogen and factors VII-X are elevated, which increases the risk of thromboembolic events during pregnancy due to factors like venous stasis and endothelial dysfunctions. In terms of endocrinological manifestations, pregnancy leads to elevated levels of T3 and T4, mainly due to an increase in Thyroxine-Binding Globulin (TBG) caused by estrogen. ACTH, aldosterone, Corticosteroid-Binding Globulin (CBG), prolactin, and oxytocin levels also increase during pregnancy. Conversely, FSH and LH levels decrease due to the increased secretion of estrogen, progesterone, and inhibin. During pregnancy, several musculoskeletal and dermatologic changes occur. The growing uterus exerts mechanical stress on the body, leading to the development of joint laxity due to hormonal fluctuations. This can result in symptoms like lower back pain, pelvic pain, sacroiliac joint pain, and hip pain. Additionally, increased fluid retention can lead to carpal tunnel syndrome. Pregnancy can cause various pigmentation changes. These include darkening of the areola and the Linea nigra, as well as increased facial pigmentation. The stretching of the skin may also lead to the formation of striae gravidarum, commonly known as stretch marks, which can result in scarring [5].
Preeclampsia: Preeclampsia is characterized by new-onset hypertension, proteinuria, or hypertension with end-organ damage without proteinuria at >20 weeks’ gestation or postpartum in previously normotensive women. It occurs in 4.6% of pregnancies worldwide and 5% in the United States, with 0.3% before 34 weeks gestation and 2.7% after 34 weeks gestation [6]. Pathogenesis is thought to occur because of placental abnormalities. Spiral artery remodeling occurs when the tortuous vessels narrow, leading to hypo perfusion, hypoxia, and ischemia-trophoblast invasion due to defective differentiation results in the release of immunological factors that cause systemic endothelial dysfunction. Hypertension is related to abnormal vascular tone, proteinuria/edema relates to increased vascular permeability, and coagulopathy results from procoagulant expression (Figure 2). Preeclampsia commonly presents with headaches, blurry vision, nausea, vomiting, shortness of breath, decreased urinary output, and altered mental status. The significant risk factors for preeclampsia include nulliparity, chronic renal disease, obesity, maternal age <18 years or >40 years, prior preeclampsia, chronic hypertension, autoimmune disease, vascular disease, multiple gestations, and pregestational/gestational diabetes [7]. The diagnostic criteria for preeclampsia are: Woman after 20 weeks gestation with systolic blood pressure >140 or diastolic blood pressure >90 on at least two occasions taken 4 hours apart in a previously normotensive patient AND onset of one of the following: Proteinuria >0.3 g in 24-hour urine specimen or urinary protein/creatinine ratio >0.3 mg/mg or dipstick >2+, Platelet count <100,000/microL, Serum creatinine >1.1 mg/dL or doubling of creatinine in the absence of other renal disease, Liver transaminases at least 2x the upper limit of normal, Pulmonary edema, New-onset, and persistent headache in the absence of other causes and not responding to analgesics, visual disturbances. To classify preeclampsia with severe features, one or more must be present: severe blood pressure elevation, new-onset visual disturbances or severe/persistent headache, hepatic abnormalities, thrombocytopenia, renal abnormality, or pulmonary edema [8]. The key to managing pre-eclampsia patients is preventing seizures, prompt delivery, and treating severe hypertension. Magnesium sulfate is recommended for seizure prophylaxis if extreme features are present. The definitive treatment is prompt delivery after maternal stabilization, depending on gestational age and severity of the disease. Antihypertensive therapy such as labetalol, hydralazine, nicardipine, and nifedipine is given for patients with systolic blood pressure >160 or diastolic blood pressure >110 [9].
Eclampsia: Eclampsia is characterized by seizures during pregnancy and postpartum in preeclampsia patients. It occurs in antepartum in 50% of pregnancies, intrapartum in 20%, and postpartum in 30%. Postpartum eclampsia usually occurs 48 hours post-delivery but can be as late as four weeks post-delivery. The incidence of eclampsia is 1.45-10 per 10,000 deliveries, with a peak incidence in adolescents and early twenties with an increased risk in patients >35 years old [10]. The exact cause of eclampsia is unknown, with two models focusing on the role of hypertension. One model proposes that hypertension causes endothelial dysfunction and vasogenic/cytotoxic edema via the breakdown of circulatory autoregulation. The second model suggests that hypertension causes the activation of circulatory autoregulation, leading to vasoconstriction, ischemia, endothelial dysfunction, and vasogenic/cytotoxic edema of the cerebral vessels (Figure 2). Eclampsia most commonly presents with hypertension, headaches, shortness of breath, edema, right upper quadrant or epigastric pain, nausea/vomiting, mental status changes, and visual disturbances. Most patients’ clinical diagnosis is based on a hypertensive disorder in pregnancy and newonset tonic-clonic seizures with recovery within 10-20 minutes and no focal neurological deficits. Other conditions, such as epilepsy, cerebral arterial infarction, intracranial hemorrhage, or drug use, must be ruled out. Neuroimaging via CT or MRI is indicated in patients with focal neurological deficits, prolonged coma, or seizures at <20 weeks’ gestation. Classic imaging findings in 90% of eclampsia patients are similar to Posterior Reversible Encephalopathy Syndrome (PRES), with cerebral edema evident [11]. Hypertension contributes to approximately 15-20% of deaths in eclampsia patients, highlighting the urgency of prompt treatment to avoid maternal hypoxia and stroke. Antihypertensive therapy for eclampsia is like preeclampsia and includes medications like labetalol, hydralazine, nicardipine, or nifedipine. These drugs are administered at specific intervals for patients with systolic blood pressure above 160 or diastolic blood pressure above 110 until the target blood pressure is achieved. During a witnessed seizure, maintaining airway patency and preventing aspiration are crucial. Hypoxemia resulting from seizure is treated with supplemental oxygen provided via a non-rebreather mask at a rate of 8-10 mL/min. To prevent seizure recurrence, magnesium sulfate is the primary treatment and is continued for 24-48 hours post-delivery. In prolonged seizures, Diazepam or Lorazepam can be used. At the same time, Phenytoin may be considered if contraindications for magnesium sulfate are present, such as myasthenia gravis, pulmonary edema, and cardiac conduction defects. The definitive treatment for eclampsia involves prompt delivery of the baby once the mother’s condition has stabilized [12].
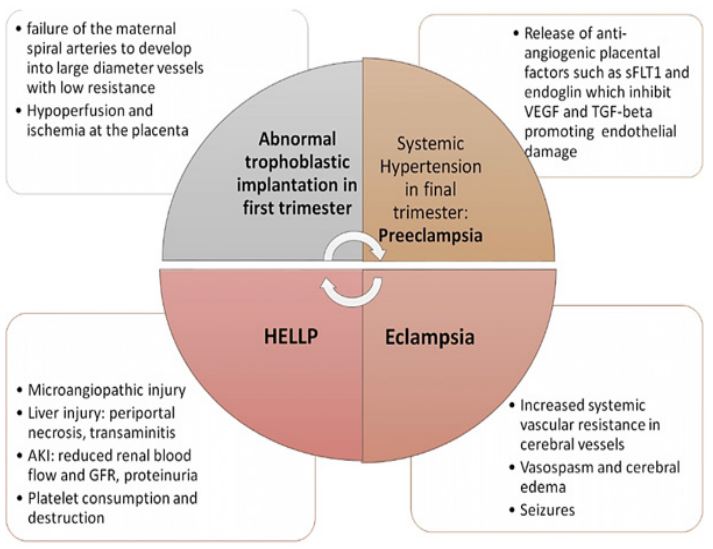
sFLT1: soluble Fms-Like Tyrosine Kinase-1; VEGF: Vascular Endothelial Growth Factor; TGF-beta: Tumor Growth Factor.
HELLP syndrome: HELLP syndrome (hemolysis with microangiopathic blood smear, elevated liver enzymes, and low platelet count) occurs in 0.1-1% of pregnancies, typically in the third trimester. 1-2% of patients with severe pre-eclampsia and eclampsia have microangiopathic hemolysis and, therefore, HELLP syndrome. While the pathogenesis remains unclear, it is thought that HELLP syndrome develops from microangiopathic hemolysis and endothelial cell damage with subsequent platelet consumption and fibrin deposits. The liver is the primary organ involved in HELLP syndrome, and in severe cases, it can lead to subcapsular hematomas contributing to hepatic necrosis. The most common clinical manifestations of HELLP syndrome are epigastric/right upper quadrant abdominal pain, nausea, jaundice, visual disturbances, headaches, and vomiting. In 85% of cases, hypertension >140/90 and proteinuria occur. Most patients are diagnosed at 28-36 weeks gestation, but symptoms can be present up to a week postpartum [13,14].
The Tennessee classification is used to diagnose HELLP and requires the following: Hemolysis with at least two of the following: schistocytes and burr cells on peripheral blood, serum bilirubin >1.2 mg/dL, low serum haptoglobin or LDH (Lactate Dehydrogenase) >2x upper limit of normal or severe anemia not related to blood loss, Elevated liver enzymes with AST or ALT >2x upper limit of normal, Low platelets <100,000 cells/µL. Severe hypertension should be treated with antihypertensive therapy such as IV labetalol, hydralazine, nicardipine, or nifedipine to reduce stroke risk. Magnesium sulfate IV is administered to prevent seizures between 24-32 weeks gestation. Antenatal corticosteroids can be given to protect fetuses if they are <34 weeks gestation. Prompt delivery is necessary if the patient is hemodynamically stable and anemia or coagulopathy is corrected. If patients have DIC (Disseminated Intravascular Coagulopathy), pulmonary edema, or renal failure, prompt delivery is warranted once the patient is stabilized. If the patient presents with acute abdomen, shock, or severe right upper quadrant pain, rupture of subcapsular hematoma is suspected, and surgical intervention is recommended. Hepatic bleeding is controlled with volume replacement and transfusion of blood products as necessary [15].
Acute fatty liver: AFLP is a rare yet fatal condition most commonly associated with the third trimester of pregnancy, characterized by liver failure and multiorgan dysfunction. Pathogenesis is linked to the defective handling of fatty acid oxidation by the fetal/placental unit, leading to the buildup of intermediate metabolites in the maternal liver. These metabolites, in combination with reactive oxygen species, cause inflammation and hepatocellular necrosis. Abnormal laboratory findings include elevated bilirubin, liver enzymes, ammonia, uric acid, leukocyte count, hypoglycemia, and coagulation disorders [16]. Patients are presented with nausea, vomiting, epigastric abdominal pain, anorexia, jaundice, and encephalopathy. The incidence of AFLP ranges from 1:7,000 to 1:20,000 pregnancies [17]. Imaging modalities that can be helpful in the diagnosis include ultrasound, CT scan, MRI, and liver biopsy. Management includes symptomatic stabilization in the intensive care unit with prompt delivery of the fetus. Biochemical, hematological, and coagulation disorders should be corrected alongside diligent monitoring for 24-48 hours.
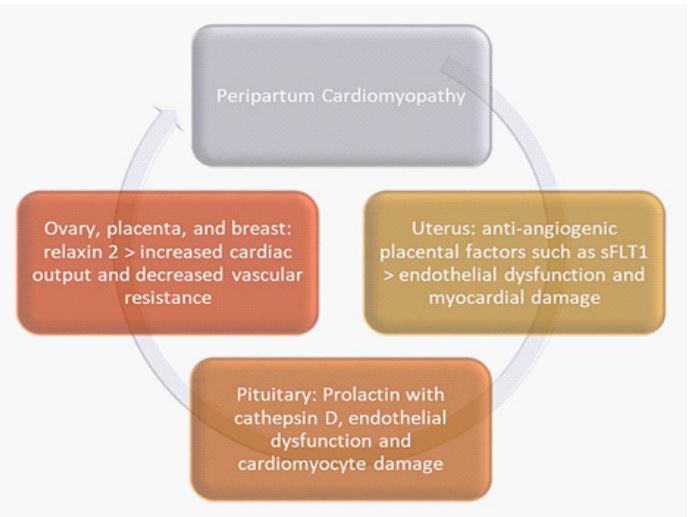
Peripartum/postpartum cardiomayopathy: Peripartum Cardiomyopathy (PPCM) is defined as nonischemic heart failure due to left ventricular dysfunction (LVEF<45%) presenting in the last few months of gestation or the initial postpartum months, for which no other cause can be identified. Presenting complaints include exertional dyspnea, orthopnea, and peripheral edema. The incidence of PPCM in the United States varies according to incidence reports from 1:1,000 to 1:3,200 live births [18]. PCCM results from vascular damage caused by the cleavage products of certain hormones, especially prolactin [1,5]. Other suggested mechanisms are linked to gene variants encoding sarcomere proteins, nutritional deficiencies, myocarditis, autoimmune processes, etc [18]. Pathogenesis of peripartum cardiomyopathy may result from vascular dysfunction, including endothelial injury and inflammation, leading to impaired blood flow to the heart muscle. Pregnancy-related changes in the vascular system, such as increased oxidative stress, endothelial dysfunction, and altered immune responses, may contribute to this process. Pregnancy is associated with significant hormonal changes, including elevated levels of estrogen, progesterone, and prolactin. These hormones may directly or indirectly affect the heart, including alterations in cardiac remodeling, contractility, and vascular function. Prolactin, in particular, has been implicated in PPCM pathogenesis due to its role in promoting cardiac hypertrophy and impairing cardiac function. The autoimmune mechanism includes autoantibodies against cardiac proteins, such as beta-adrenergic receptors or sarcomeric proteins, which have been detected in PPCM patients, suggesting a possible autoimmune component to the disease (Figure 3). Investigative findings in PCCM include tachycardia in ECG, enlarged heart in chest radiography, and LV dilatation, among others. Lab values may reveal elevated troponin and BNP. Management of PCCM is control of fluid status (approached with caution during gestation), neurohumoral mechanism with ACEI or ARB (in the postpartum period) or nitrates and hydralazine (gestational period), beta-blockade, and anticoagulation. Other management modalities include bromocriptine and cessation of breastfeeding due to the role of prolactin. Recovery of LV function is usually achieved in the first six months. Cardiac transplantation is the last resort [19].
Postpartum hemorrhage: Postpartum Hemorrhage (PPH) is defined as a blood loss greater than or equal to 1,000 ml or blood loss accompanied by signs or symptoms of hypovolemia within 24 hours after the birth process, regardless of the delivery route. PPH initially presents tachycardia and hypotension. It is the leading cause of maternal mortality worldwide, accounting for 8% of maternal deaths in developed countries and 20% in developing countries. A comprehensive physical examination, along with the utilization of a sonogram, aids in determining the underlying cause of Postpartum Hemorrhage (PPH). Atonic uterus, coagulopathies, placental abnormalities, retained products of conception, infection, and trauma to the genital tract are the most common causes of peripartum hemorrhage [20]. Secondary postpartum hemorrhage refers to excessive bleeding more than 24 hours after delivery up to 12 weeks postpartum. Secondary PPH is often attributed to uterine atony due to retained products with or without infection. Initial management aims to hemodynamically stabilize the patient with crystalloids and blood products, constantly needing the initiation of a massive transfusion protocol. 1g of Tranexamic Acid can also be used to prevent further hemorrhaging. Hysterectomy is the definitive management when pharmacological, resuscitative, mechanical, and fertility-preserving surgical interventions have been futile [21].
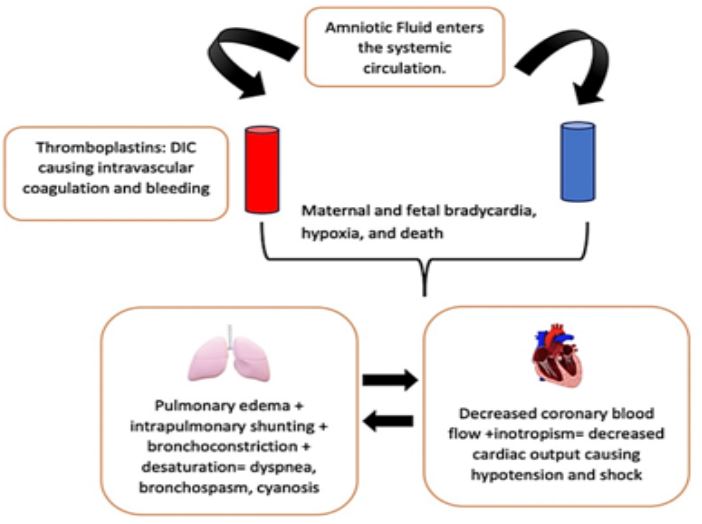
Amniotic fluid embolism: Amniotic Fluid Embolism (AFE) is a rare and often fatal obstetric condition characterized by sudden cardiovascular collapse, altered mental status, and Disseminated Intravascular Coagulation (DIC). Despite being a devastating condition, it is relatively rare. The incidence reported for AFE ranges from 1.9 to 6.1 cases per 100,000 deliveries [22]. The pathogenesis of AFE needs to be clarified. It is hypothesized that entry of amniotic fluid (which contains fetal cells and other antigenic material) into the maternal systemic circulation via a breach in the maternal/fetal interface leads to abnormal activation of humoral and immunological processes and release of vasoactive and procoagulant substances (Figure 4). As a result, pulmonary pressures usually become acutely elevated, the Right Ventricle (RV) pressure increases, and the RV begins to fail. Mechanical obstruction of pulmonary arteries from cellular components and debris in amniotic fluid plays no role in this RV failure. RV failure may subsequently lead to Left Ventricle (LV) failure and systemic hypotension. In most cases, AFE occurs during labor and delivery or within 30 minutes postpartum. AFE can also occur following a first or second-trimester abortion (medical or surgical), miscarriage, amniocentesis, or abdominal/uterine trauma. However, this is rare and typically only described in case reports. However, in most patients, the clinical presentation of AFE is abrupt, catastrophic, and rapidly progressive. Classically, patients present with cardiorespiratory compromise or sudden hypoxia and hypotension, often accompanied by noncardiogenic pulmonary edema and hemorrhage due to Disseminated Intravascular Coagulopathy (DIC). Diagnosis for AFE is purely clinical. The diagnosis should be suspected in pregnant or recently postpartum women who experience sudden cardiovascular collapse, severe respiratory difficulty and hypoxia, and seizures, particularly when followed by Disseminated Intravascular Coagulopathy (DIC). A working group of the Society for Maternal-Fetal Medicine (SMFM) and the Amniotic Fluid Embolism Foundation proposed a definition of AFE based on the presence of four diagnostic criteria, all of which must be present [23].
Criteria for AFE (all must be present): Sudden onset of cardiorespiratory arrest OR hypotension with evidence of respiratory compromise, Documentation of overt DIC using the scoring system of the Scientific and Standardization Committee on DIC of the International Society on Thrombosis and Hemostasis (ISTH), modified for pregnancy [24], Clinical onset during labor or within 30 minutes of placental delivery, Absence of fever (≥38°C) during labor. In unstable patients, a multidisciplinary, team-based approach involving maternal-fetal medicine, anesthesia, critical care, respiratory, and nursing is desirable to increase the chances of stabilization and avoid further deterioration, given that most patients present with acute cardiorespiratory compromise, hypoxemia, and hemorrhage from Disseminated Intravascular Coagulation (DIC). The initial goal is to perform Cardiopulmonary Resuscitation (CPR) as per ACLS protocol. Control of hemorrhage and the reversal of coagulopathy comes next, using tranexamic acid and a massive transfusion protocol. Delivery of the fetus comes next in aiding maternal resuscitation. For patients who are hemodynamically stable at presentation, once patients are delivered and stabilized, they should be transferred to the intensive care unit for further care. Management is supportive and focused on maintaining a secure airway [25], hemodynamic stability, and preventing bleeding.
Ectopic pregnancy: Ectopic pregnancy is a life-threatening condition and the most common cause of maternal death in the first trimester of pregnancy. Ectopic pregnancy can present as abdomen pain and first-trimester vaginal bleeding. The most common site is in the fallopian tubes, but the other sites that can be involved are cesarean scar, tubal salpingitis, ovarian, abdominal, corneal, intramural, and cervical. Its incidence ranges from 4.5-16 per 1000, with maternal mortality up to 5% in most developed countries [26]. The common risk factors are the age of over 40, infertility, previous tubal pregnancy, previous ectopic pregnancy, tubal abnormality or pathology, intrauterine device, use of oral contraceptive pills, smoking, pelvic inflammatory disease, medically induced abortions, and vaginal douching. The functional impairment secondary to damaged ciliary activity and anatomic distortion can be the physiology behind ectopic pregnancy. Pelvic infection with ordinary organisms like gonorrhea and chlamydia alters tubal function, leading to obstruction and adhesions. The chlamydia infection Produces a protein (PROKR2), causing pregnancy to implant in the tubes. The biggest concern of an ectopic pregnancy is rupture. Patients become hemodynamically unstable if ectopic pregnancy ruptures with hemorrhage. Physical signs may include orthostatic hypotension, feeling faint, tachycardia, and hypotension leading to shock. The Patients may also have abdomen pain and shoulder pain due to diaphragm irritation by blood in the peritoneal cavity. Protocol for hemorrhage and immediate surgery is usually required [27]. The diagnosis of ectopic pregnancy is by history of abdomen pain and abnormal vaginal bleeding in the first trimester. Abnormal transvaginal ultrasound findings and rising hCG products with no evidence of conception in the uterine cavity can further assist in the diagnosis. The rise in hCG of less than 35 percent every two days by three different measurements is consistent with abnormal, likely ectopic pregnancy. Medical management of ectopic pregnancy includes methotrexate. It is used if the patient is hemodynamically stable with serum hCG less than 5000 milli-international units/ml, no fetal cardiac activity on ultrasound, and a size less than 3 to 4 cm. It cannot be used in hemodynamically unstable patients or if there is a ruptured ectopic pregnancy. Surgery is still an option in hemodynamically stable patients if transvaginal ultrasound shows tubal pregnancy or adnexal mass, which favors ectopic pregnancy. Emergency surgery is required in hemodynamically unstable patients, rupture of ectopic, and intraperitoneal hemorrhage [28].
Sheehan’s syndrome: Sheehan’s syndrome is the ischemic necrosis of the pituitary gland secondary to severe hemorrhagic shock occurring secondary to peripartum hemorrhage. The incidence of this condition is relatively low in developed countries, mainly due to advanced obstetrical care. However, in resource-limited countries, postpartum pituitary infarction remains a common cause of hypopituitarism. During pregnancy, an increase in pituitary volume and cell count is appreciated. The prolactin-producing cells (lactotrophs) and other cells are hyperplasia, requiring increased nutritional and metabolic demands. However, there is no increase in the corresponding blood supply. A relatively low-pressure vascular system supplies the anterior pituitary gland. This mechanism is suspected of making the pituitary cells more susceptible to ischemia [29]. Sheehan can present acutely or chronically. In its acute form, Sheehan’s syndrome is usually evident when the newborn mother has difficulty breastfeeding or cannot produce milk (agalactorrhea). Women may report problems with menstruation after childbirth, and some may never have menses until Sheehan’s syndrome is diagnosed and treated. Chronic Sheehan’s syndrome, which occurs months to years after the initial vascular insult to the pituitary gland, is diagnosed due to symptoms of hypopituitarism. These include fatigue, asthenia or weakness, hair loss, constipation, weight gain, problems with focusing or with their attention span, and cold intolerance. Patients may also have hypotension and bradycardia and exhibit secondary adrenal insufficiency, which could cause fatigue and weight loss symptoms. Diagnostic evaluation can be based on ordering a Complete Blood Count (CBC) with differential count, basic metabolic profile, thyroid function tests (TSH, FT3, FT4), FSH, LH, prolactin, estrogen, cortisol, and growth hormone. Due to the nature of necrosis in the pituitary gland, GH is usually affected first, followed by PRL, FSH, LH, ACTH, and then TSH last. A magnetic resonance imaging (MRI) evaluation of the pituitary can be done to confirm the diagnosis. An empty Sella is present in about 70% of patients; a partially empty Sella is present in about 30% of patients on a later MRI [30]. The basis for treating Sheehan’s syndrome is the lifelong replacement of deficient hormones. Hypothyroidism can be treated with levothyroxine or liothyronine replacement. Cortisol deficiency can be treated by replacement with prednisone or hydrocortisone. Gonadotropin deficiency should be treated with estrogen if the uterus has been removed and with a combination of estrogen and progesterone if a uterus is present. The growth hormone is probably the most common hormone that needs replacing, and the dosage must be individualized to the patient’s needs. For patients who develop diabetes insipidus, desmopressin (DDAVP) is the recommended treatment of choice [31].
Pregnancy-associated spontaneous coronary artery dissection (scad): Spontaneous coronary artery dissection in pregnancy is the most frequent cause of pregnancy-related myocardial infarction. It is coronary atherosclerosis, but hemodynamic and hormonal changes are due to a high level of progesterone, which affects the arterial media by altering the elastic fiber and impairing collagen synthesis. Increased blood volume and cardiac output increase wall shear stress, leading to dissection. The arteries heal spontaneously with a conservative approach rather than revascularization in stable pregnant women with no ongoing ischemia. If the left main is involved in dissection, then emergency CABG is considered, also in patients in whom PCI failed. Consider low-dose aspirin. The addition of clopidogrel to aspirin may increase the risk of bleeding. The risk of recurrence of spontaneous dissection is high in pregnant women, so they need to be counseled regarding future pregnancy [32].
Cardiac arrest in pregnancy: Cardiac arrest in pregnancy is uncommon, with incidence as low as one in every 12,000 hospital deliveries. The causes of cardiac arrest in pregnancy are divided into non-obstetric and obstetric causes. The non-obstetric reasons included are pulmonary embolism, myocardial infarction, stroke, trauma, and sepsis, and obstetrical causes are anesthesia-related (general, epidural) hemorrhage, peripartum cardiomyopathy, amniotic fluid embolism, ventricular tachyarrhythmia, and pregnancy-induced hypertension. The interdisciplinary team should be alerted immediately, which comprises a resuscitation team, obstetrician, critical care physician, nurse, neonatologist, and anesthesiologist. High-quality CPR should be provided to pregnant women by placing them in left lateral uterus displacement to prevent compression of the aorta and inferior vena cava. To prevent hypoxemia, 100% oxygen via the face mask is initiated, establish intravenous access, and early intubation to protect the airway. Apply defibrillating pads; the protocol is the same as for nonpregnant women. If no spontaneous circulation ROSC is returned in five minutes, we should consider a cesarean section [33,34].
Conclusions
In conclusion, critical illness during pregnancy presents a complex and challenging scenario that demands careful management and consideration. The health and well-being of both the mother and the unborn child are at stake, making it essential for healthcare professionals to approach these cases with the utmost expertise, sensitivity, and empathy. The presence of a critically ill pregnant patient poses a formidable challenge for critical care physicians because of the distinct physiological aspects and specific medical conditions. Comprehensive and well-coordinated care for critical pregnant patients necessitates a multidisciplinary strategy incorporating obstetricians, maternal-fetal medicine specialists, intensivists, neonatologists, and other pertinent healthcare experts. Effective communication and collaboration among these teams guarantee that medical decisions are thoughtfully evaluated, considering the potential risks and benefits involved. Moreover, it is crucial to constantly monitor the mother and baby throughout the pregnancy and during the critical illness period. Consistent fetal assessments, judicious utilization of diagnostic procedures, and vigilant observation of the mother’s condition are pivotal in promptly detecting any alterations or complications that may arise. Providing support and counseling to the pregnant woman and her family can help alleviate anxiety and stress, ultimately contributing to better overall outcomes.
Declarations
Authors acknowledgments: M Khaja and M Qureshi searched the literature and wrote the manuscript. M Khaja conceived and edited the manuscript. M Khaja supervised the paper, and treatment, and critically revised and edited the manuscript. A Qasim and K Urlapu were involved in the manuscript along with M Khaja. All authors have made significant contributions to the manuscript and have reviewed it before submission. All authors have confirmed that the manuscript is not under consideration for review at any other Journal. All authors have read and approved the final manuscript.
Conflict of interest: None of the authors has a conflict of interest or financial relationship with a commercial entity that has an interest in the subject of the manuscript.
Funding: No financial support was used for this case series.
References
- Pollock W, Rose L, and Dennis CL: A systematic review of pregnant and postpartum admissions to the intensive care. Intensive Care Medicine. 2010; 36: 1465-2010. 10.1007/s00134-010-1951-0.
- Soubra SH, Guntupalli KK: Critical illness in pregnancy: an overview. Critical care medicine. 2005; 33: 248-55. 10.1097/01.CCM.0000183159.31378.6A.
- Neligan PJ, Laffey JG: Clinical review: Special populations-critical illness and pregnancy. Critical care. 2011; 15: 1-0. 10.1186/cc10256.
- Costantine MM: Physiologic and pharmacokinetic changes in pregnancy. Frontiers in pharmacology. 2014; 3: 65. 10.3389/fphar.2014.00065.
- Pascual ZN, Langaker MD: Physiology, pregnancy. 20228.
- Epidemiology of pre-eclampsia and the other hypertensive disorders of pregnancy. Hutcheon JA, Lisonkova S, Joseph KS. Best Pract Res Clin Obstet Gynaecol. 2011; 25: 391-403. 10.1016/j.bpobgyn.2011.01.006.
- Risk factors for pre-eclampsia at antenatal booking: systematic review of controlled studies. Duckitt K, Harrington D. BMJ. 2005; 565: 2005. 10.1136/bmj.38380.674340.E0.
- American College of Obstetricians and Gynecologists (ACOG) Practice Bulletin No. 222: Gestational Hypertension and Preeclampsia. Obstet Gynecol. 2020; 135: 237. 10.1097/AOG.0000000000003891.
- National Collaborating Centre for Women’s and Children’s Health: Hypertension in Pregnancy: The Management of Hypertensive Disorders During Pregnancy, RCOG. Press, London. 2010.
- Incidence, risk factors, and associated complications of eclampsia. Liu S, Joseph KS, Liston RM, Bartholomew S, Walker M, León JA, Kirby RS, Sauve R, Kramer MS, Maternal Health Study Group of Canadian Perinatal Surveillance System (Public Health Agency of Canada). Obstet Gynecol. 2011; 118: 987. 10.1097/AOG.0b013e31823311c1.
- Posterior reversible encephalopathy syndrome in 46 of 47 patients with eclampsia. Brewer J, Owens MY, Wallace K, Reeves AA, Morris R, Khan M, Lamarca B, Martin JN Jr. Am J Obstet Gynecol. 2013; 208: 468-1. 10.1016/j.ajog.2013.02.015.
- The Parkland Memorial Hospital protocol for treatment of eclampsia: evaluation of 245 cases. Pritchard JA, Cunningham FG, Pritchard SA. Am J Obstet Gynecol. 1984; 148: 951. 10.1016/0002-9378(84)90538-6.
- Diagnosis, controversies, and management of the syndrome of hemolysis, elevated liver enzymes, and low platelet count. Sibai BM. Obstet Gynecol. 2004; 103: 981. 10.1097/01.AOG.0000126245.35811.2a.
- Hypertension in pregnancy. Report of the American College of. Obstetricians and Gynecologists’ Task Force on Hypertension in Pregnancy. American College of Obstetricians and Gynecologists, Task Force on Hypertension in Pregnancy. Obstet Gynecol. 2013; 122: 1122. 10.1097/01.AOG.0000437382.03963.88.
- Messina V, Dondossola D, Paleari MC: Liver Bleeding Due to HELLP Syndrome Treated With Embolization and Liver Transplantation: A Case Report and Review of the Literature. Front Surg. 2021; 22: 774702. 10.3389/fsurg.2021.774702.
- Strauss AW, Bennett MJ, Rinaldo P: Inherited long-chain 3-hydroxyacyl-CoA dehydrogenase deficiency and a fetal-maternal interaction cause maternal liver disease and other pregnancy complications. Semin Perinatol. 1999; 23: 100-12. 10.1016/s0146-0005(99)80044-5.
- Knight M, Nelson-Piercy C, Kurinczuk JJ, Spark P, Brocklehurst P; UK Obstetric Surveillance System: A prospective national study of acute fatty liver of pregnancy in the UK. Gut. 2008; 57: 951-6. 10.1136/gut.2008.148676.
- Gunderson EP, Croen LA, Chiang V, Yoshida CK, Walton D, Go AS: Epidemiology of peripartum cardiomyopathy: incidence, predictors, and outcomes. Obstet Gynecol. 2011; 118: 583-591. 10.1097/AOG.0b013e318229e6de.
- Arany Z, Elkayam U: Peripartum Cardiomyopathy. Circulation. 2016; 5: 1397-409. 10.1161/CIRCULATIONAHA.115.020491.
- Baird EJ: Identification and Management of Obstetric Hemorrhage. Anesthesiol Clin. 2017; 35: 15-34. 10.1097/AOG.0000000000002351.
- Bienstock JL, Eke AC, Hueppchen NA: Postpartum Hemorrhage. Obstet Gynecol. 2017; 130: 168-186. 10.1056/NEJMra1513247.
- Mazza GR, Youssefzadeh AC, Klar M: Association of Pregnancy Characteristics and Maternal Mortality With Amniotic Fluid Embolism. JAMA Netw Open. 2022; 5: 2242842-20. 10.1001/jamanetworkopen.2022.42842.
- Matsuda T: Clinical aspects of DIC--disseminated intravascular coagulation. Pol J Pharmacol. 1996; 48: 73-75.
- Grimes DA, Cates W Jr: Fatal amniotic fluid embolism during induced abortion, 1972-1975. South Med J. 1977; 70: 1325-6. 10.1097/00007611-197711000-00025.
- Hasaart TH, Essed GG: Amniotic fluid embolism after transabdominal amniocentesis. Eur J Obstet Gynecol Reprod Biol. 1983; 16: 25-30. 10.1016/0028-2243(83)90216-2.
- Alkatout I, Honemeyer U, Strauss A: Clinical diagnosis and treatment of ectopic pregnancy. Obstet Gynecol Surv. 2013; 68: 571-81. 10.1097/OGX.0b013e31829cdbeb.
- Madani Y: The use of ultrasonography in the diagnosis of ectopic pregnancy: a case report and review of the literature. Medscape J Med. 2008; 12: 35-18382705.
- Hajenius PJ, Mol F, Mol BW, Bossuyt PM, Ankum WM, van der Veen F: Interventions for tubal ectopic pregnancy. Cochrane Database Syst Rev. 2007; 24: 000324. 10.1002/14651858.CD000324.
- Woodmansee WW: Pituitary Disorders in Pregnancy. Neurol Clin. 2019; 37: 63-83. 10.1016/j.ncl.2018.09.009.
- Kanekar S, Bennett S: Imaging of Neurologic Conditions in Pregnant Patients. Radiographics. 2016; 36: 2102-2122. 10.1148/rg.2016150187.
- Matsuzaki S, Endo M, Ueda Y, et al. A case of acute Sheehan’s syndrome and literature review: a rare but life-threatening complication of postpartum hemorrhage. BMC Pregnancy Childbirth. 2017; 171: 188-2017. 10.1186/s12884-017-1380-y.
- Elkayam U, Jalnapurkar S, Barakkat MN, Khatri N, Kealey AJ, Mehra A, Roth A: Pregnancy-associated acute myocardial infarction: a review of contemporary experience in 150 cases. between. 20062011. 2014; 22: 1695-702. 10.1161/CIRCULATIONAHA.113.002054.
- Enomoto N, Yamashita T, Furuta M, Sakurai A: Japan Resuscitation Council Maternal task force. Effect of maternal positioning during cardiopulmonary resuscitation: a systematic review and meta-analyses. BMC Pregnancy Childbirth. 2022; 25: 159. 10.1186/s12884-021-04334-y.
- Jeejeebhoy FM, Zelop CM, Lipman S, Callaway CW; American Heart Association Emergency Cardiovascular Care Committee: Council on Cardiopulmonary: Critical Care, Perioperative and Resuscitation, Council on Cardiovascular Diseases in the Young, and Council on Clinical Cardiology. Cardiac Arrest in Pregnancy: A Scientific Statement From the American Heart Association. Circulation. 2015; 3: 1747-73. 10.1161/CIR.0000000000000300.