
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Report - Open Access, Volume 5
Bullous skin disease occurring due to bedbug bite: Case report
Büşra Nur Yilmaz¹*; Sema Can²; Eda Yaman³; Abdurrahman Yılmaz⁴
1Department of Medical Biology, Istanbul University Cerrahpasa Medical Faculty, Istanbul, Turkey.
2Department of Public Health, Uşak Health Directorate, Uşak, Turkey
3Department of Emergency Medicine, Uşak Research and Training Hospital, Uşak, Turkey.
4Clinic of Chest Diseases, University of Heath Sciences Süreyyapaşa Chest Diseases and Thoracic Surgery Training and Research Hospital, İstanbul, Turkey.
*Corresponding Author : Büşra Nur Yilmaz
Department of Medical Biology, Istanbul University
Cerrahpasa Medical Faculty, Istanbul, Turkey.
Email: busranurb.kaya@gmail.com
Received : Feb 10, 2024
Accepted : Feb 27, 2024
Published : Mar 05, 2024
Archived : www.jcimcr.org
Copyright : © Yılmaz BN (2024).
Abstract
Bedbug bites are arthropod bites which are mostly seen in especially developing countries and in countries which have low socio-economical status. If allergic reaction occurs due to these bites; urticarial skin rashes, macules, papular lesions can be observed. Its aetiology is not known clearly. Aim of this case example is to present the skin reactions occurring in a 40 year old male patient, who has come to our emergency service, due to bedbug bite.
Keywords: Bullous pemphigoid; Bedbug; Outo-immune disease.
Citation: Yilmaz BN, Can S, Yaman E, Yılmaz A. Bullous skin disease occurring due to bedbug bite: Case report. J Clin Images Med Case Rep. 2024; 5(3): 2899.
Introduction
Cimex Lectularis popularly known as bedbug belongs to Cimicidae insect family [1]. They feed on bleeding humans and animals [1]. This family consists of two species as Cimex Lectularis and Cimex Hemipterus which live in mild climates [1]. An adult bedbug feeds three or five times a day [1]. Bedbug bites mainly resemble other arthropod bites; but, they tend to be dense on the skin that is not covered during the sleep [2]. Single symptom of bedbug bites can be itchy erythematous macules for individuals who have not been bitten before whereas more severe local lesions such as vesicles and bullous can be observed for individuals who have been bitten before [2]. This case report presents the skin reactions occurring in the patient who has been bitten by bedbug before and who has the same complaint again; and management of this by corticosteroid treatment.
Case report
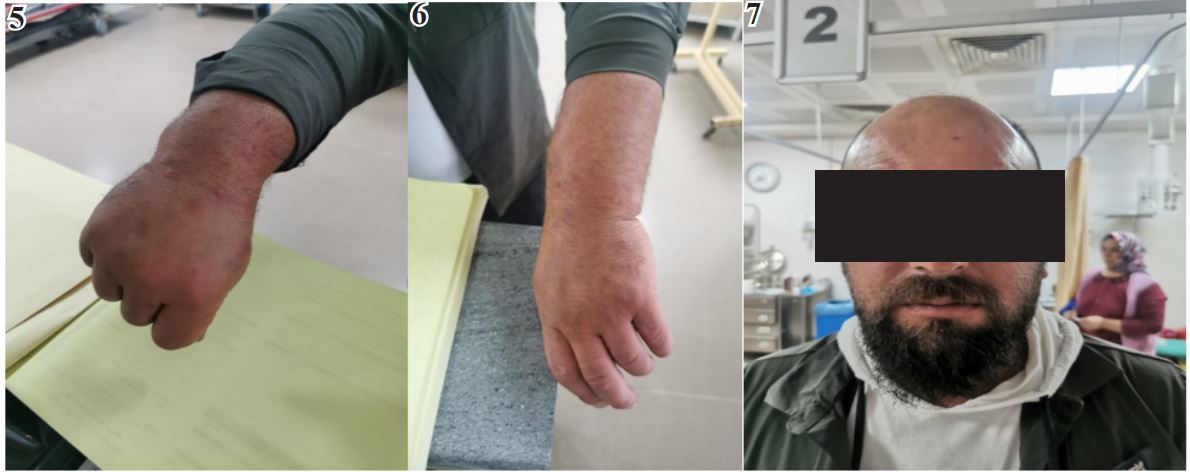
A 40 year old male patient came to our emergency service complaining about bullous and papular lesions on skin continuing nearly 1 week. It was seen in the physical examination of the patient that there were healed ülsere lesions and fluid retention around his left eye. The patient said that his complaints of these were occurred after his contact with “Cimex Lectularis” which is popularly known as bedbug. Vitals of the patient when he came were as TA: 125/82 mmHg, Pulse: 95 beat/per minute oxygen Saturation: 98% Fever: 36.3⁰C. Patient’s lesions are as the following. Patient permission was obtained for using these photographs in the report (Figures 1-4).
We have learnt that the patient does not have any chronic diseases, use any drugs regularly and is not sensitive to any allergen he knows. Other system examinations of the patient were normal and any additional pathologies were not encountered. The result of hemogram analysis of the patient was as the following: WBC: 7120 µL, HGB: 14.6 g/dL, HCT: % 42.4 and PLT: 298.000 µL. The result of biochemistry analysis of the patient was as the following: Glucose: 100 mg/dl, Creatinine: 0,83 mg/dl, GGT: 38 IU/L, ALT: 19 U/L, AST: 24 U/L, LDH: Haemolysis, Calcium: 9.5 mg/dl, Sodium: 136 mmol/L, Potassium: 4.4 mmol/L, Chlorine: 106 mmol/L, CRP: 5.3 mg/L. The result of coagulation analysis of the patient was as the following: aPTT: 22.5 seconds, PTZ: 11.5 seconds, INR: 1.0. 40 mg prednol, 40 mg pantoprazole, 45.5 mg pheniramine hydrogene maleate were applied to the patient in a 1000 cc physiological saline solution at the emergency service and this treatment continued for 3 days. At the same time the patient was prescribed 15 mg mepyramine maleate, 15 mg lidocaine hydrochloride and 50 mg gel consisting of dexpanthenol and antihistamine. The changes in the lesions of the patient when he came in the second day are as the following:
We recommended our patient whose complaints were decreased with the treatment to see the dermatology clinic.

Discussion
Bedbug causes allergic reactions. We studied diagnosis and treatment process of the patient who came to the emergency service complaining about itchy bullous papular lesions in this case report. The patient did not have any known dermatological diseases. Patient’s lesions occurred as a result of bedbug bite. The patient was discharged from the hospital after he recovered with our treatment. Richard D; DeShazo et al. took the photographs of bedbug bites at the 6th, 12th, 24th, 36th and 72th hours; even for 4 weeks in the article they published in May 2012 [3]. They scanned the medical literature for finding patients who developed bullous reaction due to these bites and found out that bedbug bites were only seen in the 6% of the patients [3]. Antigens in the bedbug’s saliva were held liable for this hypersensivity reaction [5]. Robyn S; Fallen et al. emphasized in the study they carried out that bedbug bites must be taken into consideration during differential diagnosis, these lesions causing various skin lesions and psychological disorders can even cause anaphylaxis [2]. They also asserted that corticosteroids, symptomatic drugs can be used against this bedbug invasion which does not have an exact treatment protocol; however actual treatment is the eradication of this living creature [2]. Alexandra Wieczorek et al. reported in their study that bedbug bites can imitate bullous diseases such as Pemphigoid or Duhring disease; and that differential diagnosis of the auto-immune diseases can be accurately made with immunofluorescence examinations [1]. As a result; disease situation related to bedbug must be questioned in the medical history of the patients who came to emergency service complaining about erythematous, bullous or papular lesions and this situation must not be ignored.
Conflicts of interest and financial position: Our study was not financed by an institution or organization. There are not conflicts of interest upon any issues among these authors.
References
- Wieczorek A, Szepietowski J, Łoza K, Bizoń A, Lanckorońska J, Rutkowska K et al. Bed bug bites mimicking bullous pemphigoid: a report of two cases. Przegl Dermatol. 2016; 103(4): 281-284. DOI: 10.5114/dr.2016.61775.
- Fallen R, Gooderham M et al. Bedbugs: An Uptodate on Recognition and Management Fallen RS, Gooderham M. Bedbugs: an update on recognition and management. Skin Therapy Lett. 2011; 16(6): 5-7. PMID: 21833462.
- DeShazo R, Feldlaufer M, Mihm Jr M, et al. Bullous Reactions to Bedbug Bites Reflect Cutaneous Vasculitis. 2012; 125(7): 688- 694. DOI: 10.1016/j.amjmed.2011.11.020.
- Leverkus M, Jochim R C, Schäd S, Bröcker E B, Andersen J F, Valenzuela J G & Trautmann A. Bullous allergic hypersensitivity to bed bug bites mediated by IgE against salivary nitrophorin. Journal of Investigative Dermatology. 2006; 126(1): 91-96