
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Weeping blisters – Clinical presentation in an uncommon site
Devi D; Rajesh R*; V Mohankumar V; Revathi K
Department of Dermatology, Venereology and Leprology, Government Erode Medical College and Hospital, India.
*Corresponding Author : Rajesh Rajagopalan
Department of Dermatology, Venereology and
Leprology, Government Erode Medical College and
Hospital, India.
Email: rajeshderma@gmail.com
Received : Jan 30, 2024
Accepted : Feb 27, 2024
Published : Mar 05, 2024
Archived : www.jcimcr.org
Copyright : © Rajesh R (2024).
Abstract
Lymphangioma Circumscriptum (LC), a microcystic hamartomatous lymphatic malformation is a rare benign condition characterized by the proliferation of dilated lymphatic vessels in the skin. Usually, it is congenital, but some may become clinically apparent later in life. They account for 4% of all vascular malformations. Usually seen in and around the shoulder and pelvic girdle. This case report discusses LC in a teenage girl with a 13-year-old history of painless, grouped fluid filled blisters on the right side of her chest, an uncommon site presenting after several years seeking intervention. The diagnosis was established through clinical examination and skin biopsy. With normal basic laboratory investigations, we initiated her with lesional cryotherapy as the primary efficacious intervention before planning for surgical excision. Cryotherapy is cheap, safe and easily available option.
Keywords: Microcystic lymphatic malformation; Right chest wall; Cryotherapy.
Citation: Devi D, Rajesh R, Mohankumar VV, Revathi K. Weeping blisters – Clinical presentation in an uncommon site. J Clin Images Med Case Rep. 2024; 5(3): 2901.
Introduction
Lymphangioma Circumscriptum (LC) is a rare benign lymphatic malformation characterized by the proliferation of dilated lymphatic vessels in the skin. While typically congenital, cases clinically present late in life. This report emphasizes the unusual late presentation of LC in an adolescent girl in a not-socommon location and discusses the clinical approach and management. Therapeutic safety and outcome were reasonably good with liquid nitrogen application in this case.
Case report
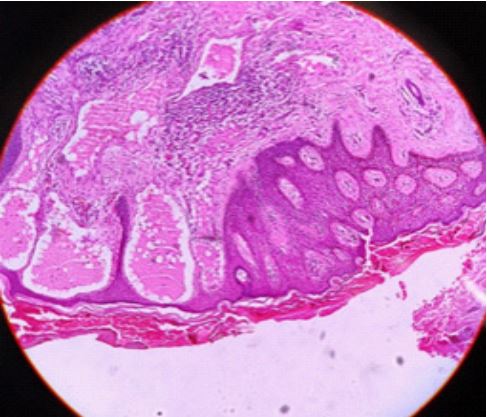
A 16-year-old female school student presented to our skin OPD with a 13-year-old history of painless, grouped vesicles on the right side of her chest, associated with mild itching and intermittent watery discharge. On examination, multiple clear translucent vesicles were observed, covering a 4x5 cm area over the right lateral chest wall along the mid-axillary line (Figure 1). A few ruptured vesicles showed clear fluid discharge. The clinical diagnosis of microcystic lymphatic malformation (lymphangioma circumscriptum) was established, with no involvement of other sites. Nail, hair, and mucosa were unremarkable. Basic laboratory investigations were within normal ranges histopathology of lesional skin revealed acanthosis and hyperkeratosis of epidermis. Within the papillary and reticular dermis, dilated lymphatic channels with eosinophilic proteinaceous material inside were observed (Figure 2). MRI was done to rule out deeper lymphatic system involvement. Cryotherapy with liquid nitrogen was performed as the primary intervention due to its superficial nature. The patient is currently under follow-up to monitor treatment response and we are assessing the need for surgical excision as future further intervention. Lesions are reducing in size and no new lesions were observed.
Discussion
Normal skin has no lymphatic channels in the papillary dermis. However, in LC, dilated channels are noted in the dermis, which at few times protrude above the skin surface. LC is an uncommon hamartomatous malformation first described by Fox and Fox in 1879 under the name of “lymphangiectodes” and the present term was given by Morris in 1889. It is a microcystic lymphatic malformation and is a rare condition characterized by translucent vesicles resembling “frogspawn or tapioca pudding” [1]. It accounts for 4% of all vascular malformations, it manifests as a dermal vesicular component and a non-obvious subcutaneous cisternal component. Acquired form is commonly associated with lymphadenectomy, radiotherapy and postsurgical/radiation complications (called lymphangiectasis) [2], it can also arise due to inflammatory diseases such as filariasis, Crohn’s disease, Hidradenitis Suppurative (HS), chronic cutaneous tuberculosis etc. Vulval lesions are seen as late complication of Lymphogranuloma venereum. Onset occur either at birth or around 5 years of age, presenting in two groups, classical and localized. Affected sites include the neck, oral cavity, axilla, breast, chest, perianal region, buttock, and vulva & scrotum. Vesicles may contain fluid or blood, with colours ranging from red to blue-black. Pain, pruritus, and exudation may occur, and complications like bleeding and malignant change, though rare can occur. The main pathology is muscular lymphatic cisterns in the deep dermis and subcutaneous tissue is not aberrant and not in continuity with normal lymph conduction systems. Hence retrograde transmission of pressure from these lymph vessels causes dilatation of superficial lymphatics leading to blister formation. Clinically present as asymptomatic, red flat, indurated, or atrophic plaques at later life. It has a typical histopathology pattern. These cutaneous lymphatic malformations show dilated, thin-walled, irregular vascular channels with lymphocytes, histiocytes, or RBCs [3]. Microcystic malformations mimic angiokeratomas but with fewer RBCs. Macrocystic malformations exhibit larger channels with thick vessel walls due to fibrous tissue and myofibroblasts. In dermis fibrosis, broadening of subcutaneous fibrous septae, and lymphoid aggregates may be present. The malformed vessels stain positively with lymphatic markers – Prox1, D2- 40, VEGFR-3, and LYVE-1(lymphatic vessel endothelial hyaluronan receptor-1), also biopsy reveals angulated channels staining positive for CD31. Dermoscopically, yellow lacunae surrounded by pale septa are noticed, with yellow to pink lacunae indicating blood. Hypopyon - like features are also seen.

Ultrasound (USG) shows multicystic lesions with internal septations and no blood flow in color Doppler. Lymphangiography and Magnetic Resonance Imaging (MRI) are preferred for evaluating deeper structures and determining the extent. There will be serpiginous-like structures in the subcutaneous tissue (isointense musculature in T1 and hyperintense in T2) [4]. Biopsy reveals angulated channels staining positive for CD31 and D2-40.
Complications if no intervention is done are secondary infection, hemorrhage, lymphorrhea, cellulitis, Squamous Cell Carcinoma (SCC), verruciform xanthoma, lymphangiosarcoma, trauma obstruction, pain, and thrombosis. Other diseases to be considered before pinning down the diagnosis are angiokeratoma, epidermal warts, anogenital warts (if perianal lesions), hemangioma, molluscum contagiosum, metastatic carcinoma, haemolymphangioma, herpes zoster, warts, angiosarcoma, leiomyoma syndromes in which lymphangioma circumscriptum is an accompanying feature include Turner syndrome, KlippelTrenaunay-Weber syndrome, and CLOVES syndrome.
Treatment
Topical treatment with 5% Imiquimod cream has shown promise in LC remission on long-term usage. By inducing endogenous interferons and interleukins, imiquimod exhibits efficacy in inhibiting vessel formation and inducing endothelial cell apoptosis [5].
Destructive treatment includes CO2 laser and long-pulsed Nd: YAG laser therapy with varied efficacy in ablating lesions, offering a less invasive alternative to surgical treatment. Electrosurgery and electrocoagulation provide additional options for targeted tissue destruction. Cryotherapy is considered, especially for smaller and localized lesions. Superficial radiotherapy remains a viable option, though its use may be limited due to potential side effects. Pulsed Dye Laser therapy is employed for its selective photothermolysis effect on vascular lesions. Sclerosing injection therapies involving 23.4% hypertonic saline, 1% or 3% tetradecyl sulfate, doxycycline, polidocanol, or ethanol directly into lymphatic malformation offer an alternative nonsurgical approach [5].
Embolization or ligation and intralesional steroid administration are also tried. Compression therapy may be utilized to reduce the swelling size, especially in cases where the lymphatic malformation involves larger areas. Wide surgical excision is the best treatment and has a recurrence rate of 23%, emphasizing the need for alternative approaches. Antibiotic coverage should be considered in cases of infection, providing adjunctive support to prevent complications.
Conclusion
This case report underscores the atypical late presentation, and uncommon site of lymphangioma circumscriptum in an adolescent girl and highlights the importance of considering this diagnosis in cases of longstanding vesicular skin lesions. Even though wide surgical excision is the better option, cryotherapy as demonstrated in this case, offers a potential therapeutic option with ongoing clinical follow-up needed for optimal therapeutic output.
Declarations
Ethical committee approval: Written informed consent was obtained from the patient /parents described here in this article. The manuscript has been read and approved by all the authors, and the requirements for authorship in this document have been met, and that each author believes that the manuscript represents honest work.
Source of support: Nil.
Conflict of interest: None declared.
References
- Neville BW, Damm DD, Allen CM, Bouquot JE. Soft tissue tumors. In: Neville BW, editor. Oral and Maxillofacial Pathology. 2nd ed. New Delhi, Philadelphia: Saunders Publishers. 2002; 475-7.
- Leshin B, Whitaker DC, Foucar E. Lymphangioma circumscriptum following mastectomy and radiation therapy. J Am Acad Dermatol. 1986; 15(5-2): 1117-9. doi: 10.1016/s0190-9622(86)70276- 4.
- Ganesh C, Sangeetha GS, Narayanan V, Umamaheswari TN. Lymphangioma circumscriptum in an adult: an unusual oral presentation. J Clin Imaging Sci. 2013; 3: 44. doi: 10.4103/2156- 7514.120779.
- Martínez-Menchón T, Mahiques-Santos L, Febrer-Bosch I, Valcuende-Cavero F, Fortea-Baixauli JM. Lymphangioma circumscriptum: an example of Whimster’s hypothesis. Pediatr Dermatol. 2004; 21(6): 652-4.
- Puri N; Treatment options of lymphangioma circumscriptum; Indian Dermatol Online J. 2015; 6(4): 293-4.