
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
An esophageal neuroendocrine tumor with initial present dysphagia: A case report
Sepide Shirchi1; Alireza Kashian1; Hossein Ghorbani2; Javad Shokri-Shirvani3*
1Student Research Committee, Babol University of Medical Sciences, Babol, Iran.
2Department of Pathology, Rohani Hospital, Babol University of Medical Sciences, Babol, Iran.
3Department of Internal Medicine, Rohani Hospital, Babol University of Medical Sciences, Babol, Iran.
*Corresponding Author : Javad Shokri-Shirvani
Department of Internal Medicine, Rohani Hospital,
Babol University of Medical Sciences, Babol, Iran.
Email: javadshokry@gmail.com
Received : Feb 03, 2024
Accepted : Feb 28, 2024
Published : Mar 06, 2024
Archived : www.jcimcr.org
Copyright : © Shokri-Shirvani J (2024).
Abstract
Introduction: Neuroendocrine Neoplasms (NENs) of the esophagus are exceedingly rare, representing 1.3% of gastrointestinall NENs and 0.4%-2% of all esophageal malignancies. Esophageal NENs are classified into well-differentiated Neuroendocrine Tumors (NETs) and poorly differentiated Neuroendocrine Carcinomas (NECs). Esophageal NETs commonly present with dysphagia, weight loss, and appetite loss.
Case report: A 70-year-old male with a history of GERD presented with progressive dysphagia and weight loss. Endoscopy revealed an ulcerative lesion, which was confirmed to be a small cell neuroendocrine carcinoma through biopsy and immunohistochemistry. A PET scan indicated a stage III tumor with locoregional lymph node involvement. The patient initiated chemotherapy and, symptomatic improvement was reported after two cycles.
Conclusion: We present a case of esophageal Small Cell Neuroendocrine Carcinoma (SCNEC) characterized by initial symptoms of dysphagia and weight loss. Given the rarity of this malignancy and the absence of a well-established standard treatment and staging system for Neuroendocrine Carcinomas (NECs), the management of patients and prediction of patient prognosis pose considerable challenges.
Keywords: Neuroendocrine neoplasm; Esophageal cancer; Small cell carcinoma; Dysphagia.
Citation: Shirchi S, Kashian A, Ghorbani H, Shokri-Shirvani J. An esophageal neuroendocrine tumor with initial present dysphagia: A case report. J Clin Images Med Case Rep. 2024; 5(3): 2905.
Introduction
Neuroendocrine Neoplasms (NENs) of the esophagus are extremely rare, comprising 1.3% of all NENs arising from the gastrointestinal tract and between 0.4% and 2% of all malignancies of the esophagus [1,2]. The 2019 World Health Organization (WHO) Classification for the digestive system categorizes NENs into well-differentiated Neuroendocrine Tumors (NETs) and poorly differentiated Neuroendocrine Carcinomas (NECs) based on their molecular differentiation. NETs can be subdivided into three grades based on the mitotic rate and Ki-67 index, while NECs are considered high grade and can be subdivided into Large-Cell type (LCNEC) and Small-Cell type (SCNEC) according to the nucleus/cytoplasm ratio, cell shape, chromatin, and nucleoli [3]. The most common symptom of esophageal NETs is dysphagia, followed by weight and/or appetite loss. Retrosternal and epigastric pains, odynophagia, dysphonia, dyspnea, and digestive bleeding (hematemesis and melena) have also been reported as less frequent clinical features [4]. Standardized guidelinesfor staging and managing esophageal NENs have not yet been described due to their rarity. This report describes a 70-yaer-old male diagnosed with small cell cancer of the esophagus.
Case report
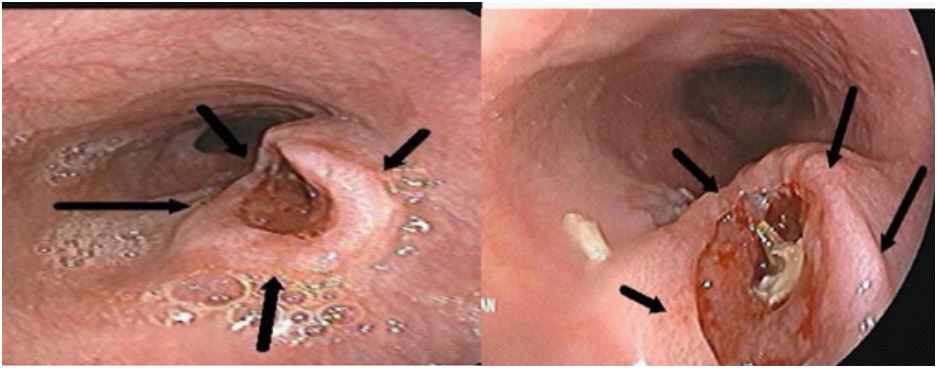
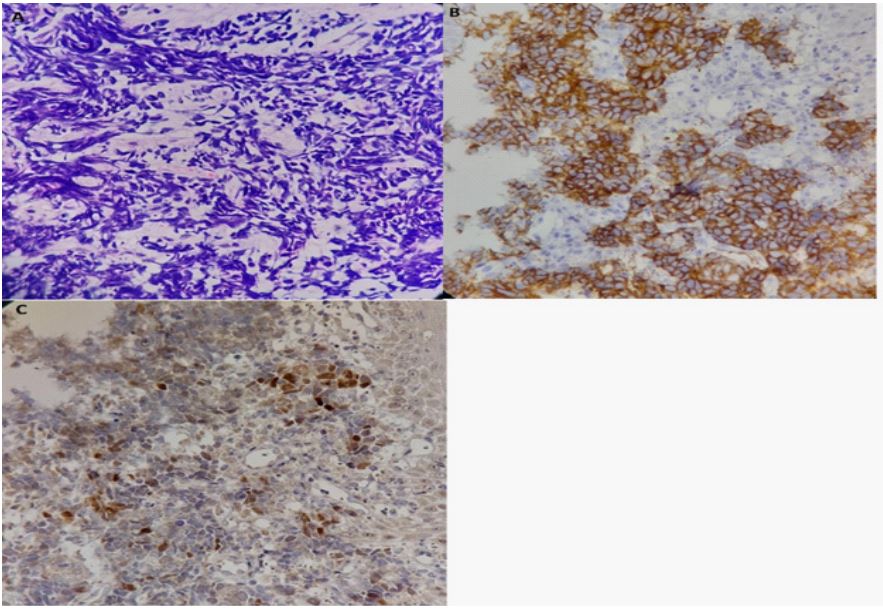
A 70-year-old male who presented with a six-month history of progressive dysphagia to solid foods associated with weight loss attended the gastroenterology clinic in September 2023. He denied retrosternal and epigastric pain, gastrointestinal bleeding, or fever. He had a history of Gastroesophageal Reflux Disease (GERD) for several years and was managed with Proton Pump Inhibitors (PPIs). The patient’s past medical history, apart from GERD, was unremarkable. He also reported no use of alcohol or tobacco. On physical examination, the patient exhibited a normal head and neck and a soft, nontender, nondistended abdomen, indicating no apparent organomegaly or lymphadenopathy. The initial laboratory test results, including complete blood count, basic metabolic panel, and liver function test results, were within normal ranges. The patient underwent Esophagogastroduodenoscopy (EGD), which revealed a 1.5x1.5 cm ulcerative lesion precisely situated at the 10 cm mark from the gastroesophageal junction (Figure 1). Biopsy obtained via endoscopy demonstrated the presence of small cell neuroendocrine carcinoma. According to the Immunohistochemistry (IHC) results, TTF1 (Transcription Termination Factor 1) exhibited positivity in a subset of neoplastic cells, while synaptophysin demonstrated strong immunoreactivity; however, no immunoreactivity wasobserved for chromogranin or CK5/6 (cytokeratin 5/6) (Figure 2). A Positron Emission Tomography (PET) scan indicated a hypermetabolic tumoral mass in the middle thoracic esophagus, confirming the existence of the known malignancy. Furthermore, there was locoregional lymph node involvement in the right paratracheal region (CNI), with no indication of hypermetabolic tumoral lesions in other imaged areas of the body. The involvement of locoregional lymph nodes without evidence of distant metastases confirmed stage III poorly differentiated small cell neuroendocrine carcinoma. The patient initiated chemotherapy in November 2023, during which he underwent two cycles per month. Thus far, the treatment has been well-tolerated, and the patient has reported improvement in his initial symptoms.
Discussion
The incidence of neuroendocrine neoplasms of the esophagus varies geographically, generally constituting a rare type of NEN. Tutsumi et al. reported that of 2957 patients, 98% had SCNEC (23% in Western countries; 77% in Eastern countries), 1.18% had LCNEC (94% in Western countries; 6% in Eastern countries) and 0.82% had carcinoid tumors (43% in Western countries; 54% in Eastern countries). Esophageal SCENC demonstrateda predominant prevalence in men, with a mean age of 63.8 years [5]. According to Schizas et al. dysphagia remains the most prevalent presenting symptom. The most frequent endoscopic finding was a single elevated polypoid or nodular lesion [6]. In contrast, the endoscopic findings of our patient revealed an ulcertype tumor. The risk factors for esophageal Small Cell Neuroendocrine Carcinoma (SCENC) are generally smoking and alcohol consumption, similar to those for Squamous Cell Carcinoma (SCC) [7]. However, due to its rarity and lack of adequate data, the causal relationship between these factors and SCENC has not been strongly established. It is noteworthy that our patient was a lifelong nonsmoker and did not consume alcohol. Our patient exhibited regional lymph node involvement according to the findings from the PET scan. Based on Tutsumi et al.’s research, among 423 patients with Small Cell Esophageal Neuroendocrine Carcinoma (SCENC), 63% were diagnosed with distant metastasis, while 22% and 15% of the patients were diagnosed with regional and localized disease, respectively. At present, there is no established standard treatment for NECs, and esophageal NENs were not included in the 8th edition of the AJCC/UICC TNM staging system [8]. This can pose a challenge in evaluating the prognosis and management of patients. Largescale research is required to develop a standardized staging system and treatment algorithm.
Conclusion
We present a case of esophageal Small Cell Neuroendocrine Carcinoma (SCNEC) with initial symptoms of dysphagia and weight loss. The diagnostic journey revealed regional lymph node involvement, and the patient started chemotherapy two months after the initial visit. Extensive research is needed to establish a standardized staging system and treatment algorithm.
References
- Lee CG. et al. The clinical features and treatment modality of esophageal neuroendocrine tumors: a multicenter study in Korea. BMC cancer. 2014; 14: 1-7.
- Egashira A. et al. Neuroendocrine carcinoma of the esophagus: Clinicopathological and immunohistochemical features of 14 cases. PLoS One. 2017; 12(3): 0173501.
- Nagtegaal ID. et al. The 2019 WHO classification of tumours of the digestive system. Histopathology. 2020; 76(2): 182-188.
- Giannetta E. et al. A rare rarity: Neuroendocrine tumor of the esophagus. Crit Rev Oncol Hematol. 2019; 137: 92-107.
- Tustumi F. et al. Primary neuroendocrine neoplasm of the esophagus - Report of 14 cases from a single institute and review of the literature. Arq Gastroenterol. 2017; 54(1): 4-10.
- Schizas D. et al. Neuroendocrine Tumors of the Esophagus: State of the Art in Diagnostic and Therapeutic Management. J Gastrointest Cancer. 2017; 48(4): 299-304.
- Ilett EE. et al. Neuroendocrine Carcinomas of the Gastroenteropancreatic System: A Comprehensive Review. Diagnostics (Basel). 2015; 5(2): 119-76.
- Tustumi F. et al. The Prognosis of the Different Esophageal Neuroendocrine Carcinoma Subtypes: A Population-Based Study. Arq Gastroenterol. 2022; 59(1): 53-57.