
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Fever and pleurodynia after dental appointment in a 65-year-old male
George Dimeas; Stratos Skrimizeas; Ilias E Dimeas*; Eirini Varelopoulou; Zoe Daniil
Department of Respiratory Medicine, Faculty of Medicine, University of Thessaly, Biopolis, 41500, Larissa, Greece.
*Corresponding Author : Ilias E Dimeas
Department of Respiratory Medicine, Faculty of
Medicine, University of Thessaly, Biopolis, 41500
Larissa, Greece.
Email: dimel13@hotmail.com
Received : Feb 12, 2024
Accepted : Mar 01, 2024
Published : Mar 08, 2024
Archived : www.jcimcr.org
Copyright : © Dimeas IE (2024).
Abstract
We present a unique case of parapneumonic effusion from an unusual microorganism on a 65-year-old ex-smoker with a history of arterial hypertension and diabetes mellitus, following dental procedures for a periapical tooth abscess. Cultures from the dental abscess were taken, coming back negative. However, some days after the procedure, fever and pleurodynia started showing up on the patient with his condition progressively worsening, until he visited the emergency room of the hospital. Laboratory exams and imaging were consistent with a complicated pneumonia with parapneumonic effusion. After ultrasound-guided evacuation of the effusion, Parvimonas micra (P. micra) was isolated from pleural fluid cultures, so antibiotics were accordingly modified on the treatment plan. The patient responded well, and clinical and radiological improvements were observed. This case highlights the rare occurrence of P. micra-associated pleuropulmonary infection, because of the difficulty to be isolated in the aerobic environment of the lungs, and underscores the importance of considering dental procedures as a potential source of such infections. Early diagnosis and appropriate antibiotic therapy, guided by culture and sensitivity testing, are essential for successful management.
Keywords: Parvimonas micra; Pleural effusion; Fever; Pleurodynia; Dental procedure; Pneumonia.
Citation: Dimeas G, Skrimizeas S, Dimeas IE, Varelopoulou E, Daniil Z. Fever and pleurodynia after dental appointment in a 65-year-old male. J Clin Images Med Case Rep. 2024; 5(3): 2910.
Introduction
Parvimonas micra, a small and anaerobic pathogen, mostly inhabits the oral cavity and upper respiratory system, but has also been isolated in cases of pneumonia, spondylodiscitis and arthritis [1,2]. Lack of specific clinical symptoms, as in our case, and identification methods makes the diagnosis of such cases hard for the physicians [3]. This case serves as a unique and informative example of how seemingly unrelated events can lead to a rare yet significant medical condition.
Case presentation
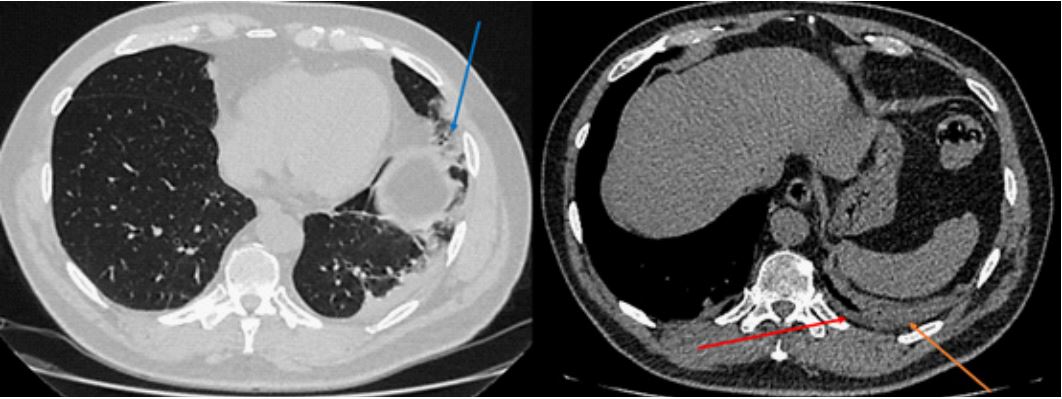
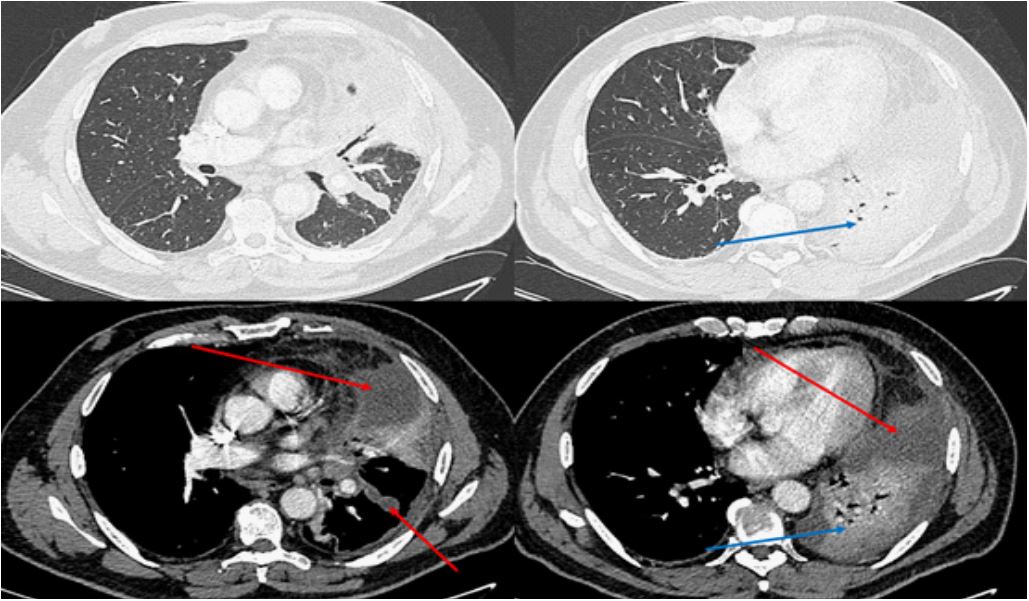
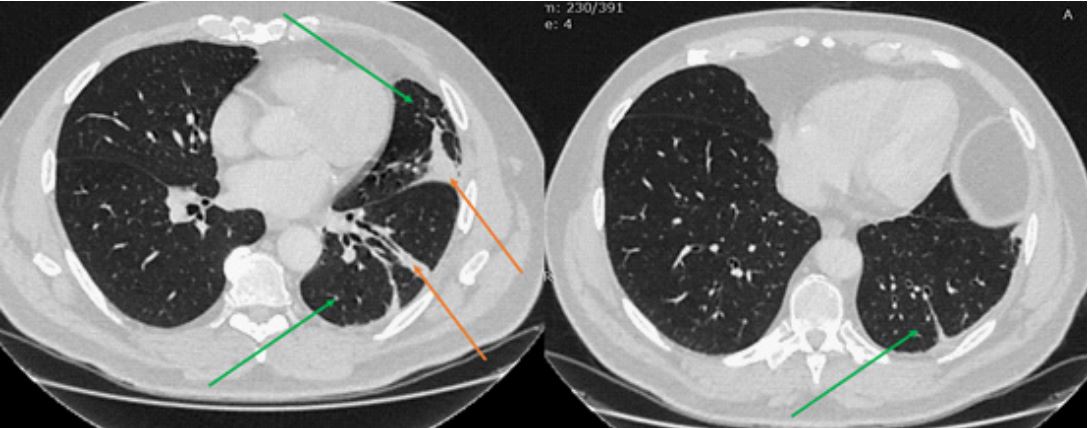
A 65-year-old ex-smoker (40 pack-years) with a medical history of arterial hypertension and diabetes mellitus was referred to our department of respiratory medicine because of a parapneumonic effusion, diagnosed in another local hospital in which he was first being treated for community-acquired pneumonia and followed-up as an outpatient. His symptoms started 15 days ago following a tooth extraction and dental cleaning due to a periapical tooth abscess. No microorganism was cultured from the tooth abscess’s pus. Ten days after the procedure, fever and left pleurodynia with acute onset were reported leading the patient to visit the Emergency Department (ED) of the local general hospital. Acute cardiac event was excluded at first and then a Computed Tomography Pulmonary Angiogram (CTPA) (Figure 1) revealed a consolidation in the left lower lobe with a very small pleural effusion without signs of pulmonary embolism. Blunted left costophrenic angle was also noted in the chest x-ray. The patient was prescribed ciprofloxacin and cefixime to be treated at home without being admitted. Persistence of his symptoms and the intensification of the chest pain led to another visit to the ED after 5 days, where he was resubmitted to a chest x-ray and subsequently to a chest CT showing a slight increase of the pleural effusion. The patient then was referred to our Department of Respiratory Medicine for further evaluation and management and was admitted. Upon admission, the patient was febrile (body temperature 38o C), tachypneic with 24 breaths per minute and hemodynamically stable. The cardiac examination did not reveal any pathological findings. On lung auscultation, decreased respiratory sounds were noted over the left base with additional inspiratory crackles over the same area. Peripheral lymph nodes were normal. No signs of oral or dental inflammation were observed. The rest of the physical examination was unremarkable. A hypoxemic respiratory failure was noted [pO2 =53 mmHg, pCO2 =36 mmHg, FiO2 =21%], according to arterial blood gas analysis necessitating supplemental oxygen therapy. Remarkable laboratory findings involved leukocytosis (21,4 x 103 cells/μL), normocytic normochromic anemia (hemoglobin concentration of 11.6 g/dL), and elevated C-reactive protein (8,93 mg/dL, [<0,05 mg/dL]). A lung ultrasound was performed showing consolidation in the left lower lobe and a small pleural effusion. A diagnostic thoracentesis revealed an orange-brown pleural fluid which was a neutrophilic exudate with pH=7,17, glucose: 39 mg/dl, LDH 870 IU/It, ADA 25,5 IU/L, albumin 3,4g/dl. Because the effusion was not big enough for a thoracic tube, 350cc of pleural fluid were actively removed with evacuative thoracentesis. The patient then was started on ceftaroline & metronidazole and oxygen therapy with nasal cannula. Even though the respiratory failure was improved after the 4th day and the patient no longer needed oxygen support, a new X-ray was performed because of the ongoing fever. A worsening of the pleural effusion was observed with an image of encapsulation which was also pointed in a chest CT (Figure 2). Under ultrasound guidance with the entry point being the anterior axillary line at the height of the nipple, 150cc of entangled parapneumonic effusion was evacuated and was sent again for further evaluation. This time from the culture, Parvimonas micra (P. micra) was isolated, which is bibliographically related to dental work. The antibiogram showed resistance to metronidazole so antimicrobial therapy changed to monotherapy with amoxicillin-clavulanate acid, to which our strain was sensitive. The patient was reevaluated on the 7th day with an ultrasound and a chest X-ray showing regression of the pleural effusion in addition to the improvement of his clinical condition. On the 10th day, the patient, afebrile, was discharged to complete 21 days of co-amoxicillin at total with a follow-up 1 month later in our outpatient clinic. At reevaluation his chest CT was improved (Figure 3) with him reporting no symptoms.
Discussion
P. micra, a conditionally pathogenic gram-positive anaerobic coccus, belonging to a family of microorganisms located mostly in various human mucous membranes. Characteristically, it is a small pathogen with a size of 0.3-0.7 μm. Historically, it was first named Peptostreptococcus micros, and then in 1999 it was reclassified as Micromonas micros. Since 2006 until now, it is formally known as P. micra [2]. It is more commonly known as an oral pathogen causing frequent oral infections after dental treatment and dental caries, but also cases of bloodstream infections, spinal infections, chest infections, and sepsis have been reported [4,5]. Cases of pneumonia have also been described, but rarely, due to the aerobic environment of the lungs. Common risk factors include immunodeficiency, cancer, diabetes mellitus, and orthopedic surgeries [6-8]. The symptoms differ based on the site of the infection. Pain is present in all patients with articular involvement and vertebral disease, pain is the most common symptom described. Fever and constitutional syndrome are also highly reported [6]. However, in some cases, the progression of the disease can be slow and nonspecific, and the patients remain without a diagnosis for a long time, increasing the risk of complications [2]. The gold standard for the diagnosis of P. micra infection is the culture of a sufficient sample taken from the site of the infection [6]. A patient with pleural effusion that is tested positive for the microorganism and a history of exposure to dental procedures can set the diagnosis [9]. Metagenomic Next-Generation Sequencing (mNGS) is a new diagnostic option, known for its higher sensitivity against traditional cultures, especially on anaerobes. The test is great for analyzing lung tissue samples, and finding the pathogenic bacteria, giving the medical community a useful tool in the testing repertoire to diagnose difficult-to-cultivate bacteria [9]. P. micra is generally sensitive to most antibiotic classes, including b-lactams, clindamycin, and metronidazole, but physicians should always be alarmed for drug-resistant strains. Close monitoring of the patient is recommended so that remission of the clinical manifestations is recorded meaning the patient responds well to antibiotics. Patients that show no regression of the symptoms or their lesions exacerbate should always raise suspicions for resistant strains, and a change to the treatment plan. It is recommended to always perform an antibiotics’ resistance test or a gene test for drug sensitivity alongside the cultures, as more information leads to the best possible treatment method [10]. In this case, the patient had been submitted to dental procedures 15 days before the onset of the symptoms. Our patient did not meet any of the other risk factors, so the dental procedures are the most likely origin. The method of isolating the microorganism was through pleuritic fluid cultures, so the proper antibiotic treatment plan was established. However, there are not many cases in the literature associating P. micra with pneumonia and pleural effusion, because the aerobic environment of the lung is not favorable for this microorganism. P. micra, probably after growing in the area of the abscess, proceeded to the lungs either hematogenously or through inhalation and caused the pulmonary manifestations.
Conclusion
Infections by P. micra are infrequent but should always be in the mind of the physician after dental interventions as the clinical manifestations of the infection tend to be non-specific. There are currently no guidelines for the treatment. The bacterium is found to be sensitive to most antibiotics. Metronidazole, once part of the initial therapy, nowadays is shown a rising resistance to, so it could be avoided until the antibiogram.
Declarations
Acknowledgments: None to declare.
Conflict of interest: None to declare.
Financial disclosures: None to declare.
Availability of data and materials: All data underlying the findings are fully available.
Ethics approval and consent to participate: No ethical committee approval was required for this case report by the Department, because this article does not contain any studies with human participants or animals. Informed consent was obtained from the patient included in this study.
Consent for publication: The patient gave his written consent to use his personal data for the publication of this case report and any accompanying images.
References
- Sultan AA, Cantrell WA, Khlopas A, et al. Acute septic arthritis of the knee: A rare case report of infection with Parvimonas micra after an intra-articular corticosteroid injection for osteoarthritis. Anaerobe. 2018; 51: 17-20. doi: 10.1016/j.anaerobe.2017.12.015.
- Shimizu K, Horinishi Y, Sano C, Ohta R. Infection Route of Parvimonas micra: A Case Report and Systematic Review. Healthcare (Basel). 2022; 10(9): 1727. Published 2022 Sep 8. doi:10.3390/healthcare10091727.
- Riggio MP, Lennon A. Identification of oral peptostreptococcus isolates by PCR-restriction fragment length polymorphism analysis of 16S rRNA genes. J Clin Microbiol. 2003; 41(9): 4475-4479. doi:10.1128/JCM.41.9.4475-4479.2003.
- Miyazaki M, Asaka T, Takemoto M, Nakano T. Severe sepsis caused by Parvimonas micra identified using 16S ribosomal RNA gene sequencing following patient death. IDCases. 2019; 19: 00687. doi: 10.1016/j.idcr.2019.e00687. PMID: 32071875; PMCID: PMC7011025.
- Jiang Y, Qin W, Li J, Gao Y, Zeng Y. A case report of sepsis and death caused by Parvimonas micra, a rare anaerobe. Front Public Health. 2022; 10: 994279. Published 2022 Sep 20. doi:10.3389/fpubh.2022.994279.
- Cobo F, Rodríguez-Granger J, Sampedro A, Aliaga-Martínez L, Navarro-Marí JM. Pleural effusion due to Parvimonas micra. A case report and a literature review of 30 cases. Rev Esp Quimioter. 2017; 30(4): 285-292.
- Feng Y, Wu C, Huang X, Huang X, Peng L, Guo R. Case report: Successful management of Parvimonas micra pneumonia mimicking hematogenous Staphylococcus aureus pneumonia. Front Med (Lausanne). 2022; 9: 1017074. Published 2022 Oct 28. doi:10.3389/fmed.2022.1017074.
- Yu Q, Sun L, Xu Z, Fan L, Du Y. Severe pneumonia caused by Parvimonas micra: a case report. BMC Infect Dis. 2021; 21(1): 364. Published 2021 Apr 17. doi:10.1186/s12879-021-06058-y.
- Zhu L, Hao Y, Li W, Shi B, Dong H, Gao P. Significance of pleural effusion detected by metagenomic next-generation sequencing in the diagnosis of aspiration pneumonia. Front Cell Infect Microbiol. 2022; 12: 992352. Published 2022 Dec 20. doi:10.3389/fcimb.2022.992352.
- Rams TE, Sautter JD, van Winkelhoff AJ. Antibiotic Resistance of Human Periodontal Pathogen Parvimonas micra Over 10 Years. Antibiotics (Basel). 2020; 9(10): 709. Published 2020 Oct 17. doi:10.3390/antibiotics9100709.