
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 5
Trick or teeth? A peculiar cause of deafness
Francisca Bartolomeu1*; José Carneiro1; João Neves1; António Miguéis1,2; Jorge Miguéis1
1Department of Otorhinolaryngology, Coimbra University Hospital Center, Portugal.
2University Clinic of Otorhinolaryngology, Faculty of Medicine, University of Coimbra, Portugal.
*Corresponding Author : Francisca Bartolomeu
Department of Otorhinolaryngology, Coimbra University Hospital Center, Portugal.
Email: 11757@chuc.min-saude.pt
Received : Feb 15, 2024
Accepted : Mar 01, 2024
Published : Mar 08, 2024
Archived : www.jcimcr.org
Copyright : © Bartolomeu F (2024).
Abstract
Abnormal development of specific first pharyngeal arch derivatives can result in ectopic teeth which can develop inside the middle ear causing hearing loss. This case is about an 11-year-old patient with hearing loss in the left ear caused by an ectopic tooth in the middle ear.
Keywords: Congenital malformation; Ectopic tooth; Conductive hearing loss.
Citation: Bartolomeu F, Carneiro J, Neves J, Miguéis A, Miguéis J. Trick or teeth? A peculiar cause of deafness. J Clin Images Med Case Rep. 2024; 5(3): 2911.
Introduction
Ectopic eruption is a disturbance in which teeth do not follow their usual course. The prevalence varies in literature 0.1% to 1% [1]. The ectopic tooth can be in the nasal cavity, maxillary sinus, palate, even in the ear and orbit [2]. Teeth derive from the first branchial arch. The outer and middle ear derive from the first and second branchial arches [3]. So abnormal development of specific first pharyngeal arch derivatives can affect both structures. If the ectopic tooth is in the ear, it can cause hearing loss, and it needs to be diagnosed and treated to reduce the impact on the patient’s life.
Case presentation
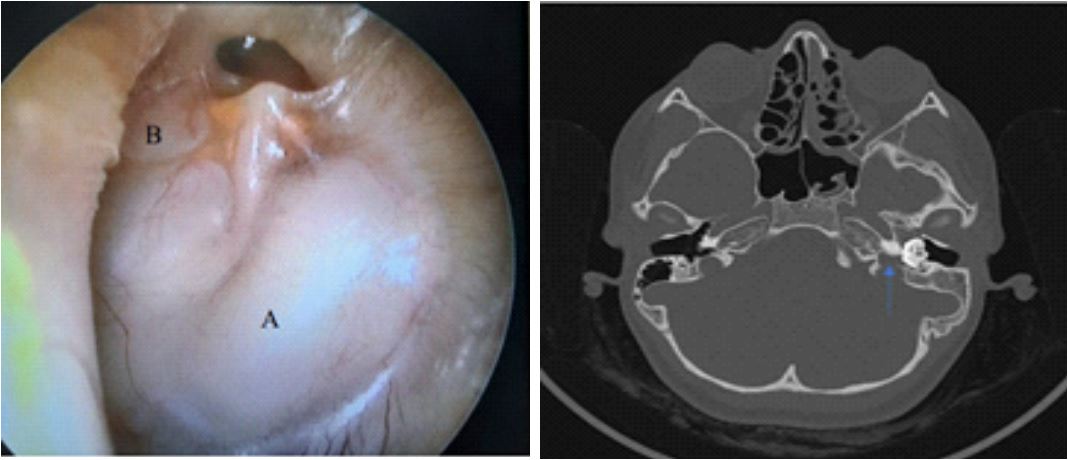
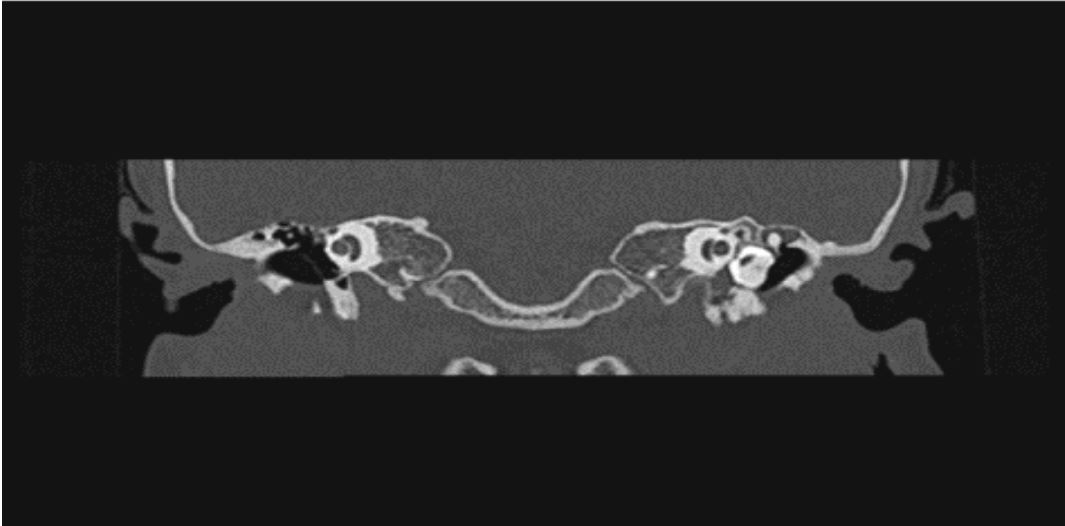
An 11-year-old patient came to our department with longterm hearing loss in the left ear. There was no history of previous otorrhea, facial paralysis or vertigo. Otoscopy showed a whitish filling of the middle ear (Figure 1A) and signs of effusion (Figure 1B). The tympanogram was type B and the pure tone audiometry showed an ipsilateral conductive hearing loss, with a threshold of 66,3 dB and an air-bone gap of 40 dB. The bone CT (Figure 2) was suggestive of an ectopic tooth occupying the mesotympanum and deviating the incudostapedial joint, although in the epitympanic region the ossicles appear to be intact. The remaining middle ear had chronic inflammation causing bone molding without compromise of the facial nerve but disrupting the cortical bone that separates the hypotympanum from the endocranial cavity, at the level of the jugular gulf (arrow in figure 2).
Discussion/Conclusion
Differential diagnosis includes teratoma, dermoid cyst and cholesteatoma, which were excluded based on clinical and imaging findings [3]. Given the surgical risk of deafness and large vessel injury in a patient without other complications besides the hearing loss, medical treatment with an ipsilateral hearing aid was suggested.
References
- Jiang X, Chen Q, Chen Y, Si Y, Liu Y, et al. Ectopic Eruption of Maxillary Third Molar Tooth in the External Acoustic Meatus: A Case Report. Ann Otolaryngol Rhinol. 2014; 2(1): 1016.
- Ray B, Singh LK, Das CJ, Roy TS. Ectopic supernumerary tooth on the inferior nasal concha. Clin Anat. 2006; 19: 68-74.
- Boone BN, Schuman TA, Eavey RD. Congenital aural atresia with ectopic tooth. Otol Neurotol. 2011; 32(9): e35.