
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Pathophysiological mechanisms, diagnosis and treatment of the fractures of the temporal bone styloid process
Sarazhyna K1*; Khodos O1; Solodovnikova Y1; Son A2
1Assistant Professor, Department of Neurology and Neurosurgery, Odesa National Medical University, Odesa, Ukraine.
2Head, Department of Neurology and Neurosurgery, Odesa National Medical University, Odesa, Ukraine.
*Corresponding Author : Kateryna Sarazhyna
Department of Neurology and Neurosurgery, Assistant Professor, ONMedU, st. Tinysta 8, Odesa,
65125, Ukraine.
Tel: +38 0636252919.
Email: katasarazina@gmail.com
Received : Feb 13, 2024
Accepted : Mar 04, 2024
Published : Mar 11, 2024
Archived : www.jcimcr.org
Copyright : © Sarazhyna K (2024).
Abstract
The styloid process is a needle-like osseous projection beneath the temporal bone, typically measuring 2.5-3 cm. Its fracture is uncommon and mostly occurs in elongated processes, often due to trauma, dental procedures, or sports. This paper presents an unusual case of a normallength styloid process fracture in a 24-year-old serviceman, resulting from a mine explosion. The patient complained of intense headaches, and pain during yawning, swallowing, and head rotation. Examination revealed pain in the left pterygopalatine fossa, and decreased pharyngeal reflex on the left, and a CT scan showed brain contusion, subarachnoid haemorrhage and a linear fracture in the normal-sized left styloid process, with no displacement. Treatment with anti-inflammatory drugs and muscle relaxants led to symptoms improvement, and no fragment dislocation was observed in a follow-up CT. This report contributes to understanding the diagnosis of normal-length styloid process fractures, contrasting with the more reported elongated ones.
Keywords: Styloid process; Blast injury; Eagle’s syndrome; Glossopharyngeal pain.
Citation: Sarazhyna K, Khodos O, Solodovnikova Y, Son A. Pathophysiological mechanisms, diagnosis and treatment of the fractures of the temporal bone styloid process. J Clin Images Med Case Rep. 2024; 5(3): 2913.
Introduction
The styloid process is a small, thin, cartilage-like cylindrical bone that projects downwards, forwards, and medially from the lower surface of the temporal bone, located posteriorly to the mastoid process, anteromedial to the stylomastoid foramen, and lateral to the jugular foramen and carotid canal. The name of the process derives from the Greek word στῦλος, meaning “pillar”. Medially to the process runs the internal jugular vein and the 7th, 9th, 10th, and 11th cranial nerves. Its apex is connected with the stylohyoid ligament, which links the styloid process to the angle of the lower jaw, and the stylohyoid ligament, which connects the base of the skull with the lesser horn of the hyoid bone (stylohyoid apparatus) [1]. There are three muscles originating from the process: the styloglossus, stylohyoid, and stylopharyngeus [1,2]. The styloid process can move with the rotation or nodding of the head [3]. There are four morphological variants of the styloid process: I - normal (up to 30 mm); II - elongated (more than 30 mm); III - pseudoarticulated; IV - segmented [4,5]. The length is measured along the posterior side of the process between its base and apex) [6]. The latter can ossify, or the process itself can elongate and fuse with the branch of the hyoid bone, which is palpable in the pharyngeal wall and causes pain during lower jaw movements forward and sideways [2]. The elongated part runs between the internal and external carotid arteries (with which it may come into contact), near the sympathetic chain [1]; the concave tip can displace the palatine tonsil medially. There are two mechanisms of injury to the styloid process: external and internal. The mechanism of external injury involves direct impact by a traumatic agent to the styloid region or an indirect mechanism due to the fracture of the lower jaw and its posterior displacement, affecting the process. The mechanism of internal injury includes uncoordinated muscle contractions during sudden neck movements or a fracture of the lower jaw, and traction of the styloid process through the stylo-mandibular ligament, which is attached to the angle of the lower jaw [7].
Clinical case
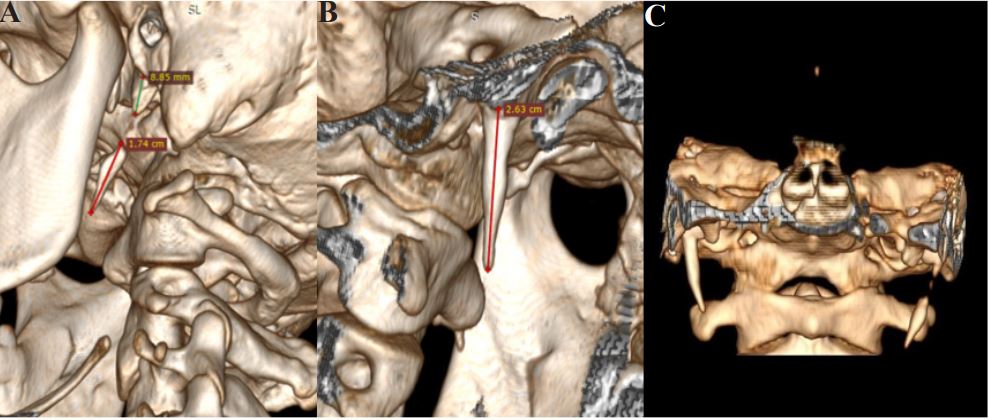
A 24-year-old serviceman was admitted to the neurological department a few days after a mine explosion injury with complaints of periodic severe headaches and facial pain on the left side during yawning and swallowing. The symptoms were provoked by palpation and exacerbated when turning his head to the right. During the injury, he was thrown backwards by the explosion wave from the left and front. Upon falling, he experienced hyperextension of the neck with a turn of the head to the right. During the examination of the patient, pain was found upon palpation in the area of the left pterygopalatine fossa and a decreased pharyngeal reflex on the left. Symptoms of vagotonia were absent. A CT scan of the brain in bone mode revealed signs of brain contusion, subarachnoid haemorrhage, and a fracture of the left styloid process without displacement (Figure 1).
The sizes of the styloid processes are 2.64 cm on the left and 2.63 cm on the right which correspond to the normal variant (up to three centimeters).
On the background of conservative treatment with nonsteroidal anti-inflammatory drugs and muscle relaxants, the symptoms regressed within 5 days. Control CT did not reveal any signs of fragment dislocation.
Discussion
Fractures of the styloid processes are extremely rare. However, some cases of elongated styloid process fractures, often accompanied by fractures of the facial skull and lower jaw, were reported. Frequent causes include sports injuries and traffic accidents [8,9]. In the available medical literature, there are isolated publications of clinical cases where injuries occur during dental procedures (with an open mouth) [5,10,11], due to uncoordinated movements between the stylohyoid and stylopharyngeal muscles on the hyoid bone, which normally should move freely but can act as a support for the muscles due to excessive stress [8,10]. During such manipulations, the muscles pull the styloid process, leading to a fracture; the fragment usually is displaced medially, caudally, and ventrally [12]. In cases of lower jaw fractures, there is an excessive posterior displacement of the mandible ascending branch, causing contact between the upper end of the branch and the styloid process and resulting in the latter’s fracture [5].
Isolated cases of spontaneous avulsion fractures caused by laughter, excessive swallowing movements, strong, abrupt coughing, or epileptic seizures are described [6,12]. If the process protrudes into the tonsillar fossa, it can be damaged during tonsillectomy [13]. Contractures that arise as part of the posttonsillectomy scar towards the styloid process can affect cranial nerves: the fifth, seventh, ninth, and tenth [6]. A styloid process of a normal length cannot be palpated through the peripharyngeal fascia, unlike the elongated one, where while palpating the tonsillar fossa with the index finger, a firm resistance can be felt [14,15]. Glossopharyngeal and pterygopalatine neuralgia can also be caused by a fracture or displacement of the styloid process, as the glossopharyngeal nerve wraps around its apex [2].
Fractures of the styloid process can be asymptomatic or have nonspecific manifestations. The most common symptoms of styloid process fracture include glossopharyngeal pain and pain during swallowing, dysphagia, otalgia, poorly localized facial pain, limited movements of the lower jaw, especially towards the affected side with difficulty in mouth opening, trismus, pain in the temporomandibular joint area, swelling and hematoma in the periauricular and peritonsillar areas [1,5,10]. On palpation, pain, and crunching can be detected between the mastoid process and the upper posterior edge of the ascending branch of the lower jaw, and pain upon palpation in the retromandibular and tonsillar fossae [6,10]. These symptoms usually resemble Eagle’s syndrome [12], and differential diagnosis is made between temporomandibular joint dysfunction, tonsillitis, and mastoiditis [5]. Eagle’s syndrome occurs due to elongation of the styloid process or calcification of the stylohyoid ligament [1]. The first manifestations of this syndrome were recorded in 1652, and the first removal of the process associated with the syndrome was in 1872 [16]. A simply elongated process may be asymptomatic, unlike one that is directed somewhat medially. This pathology is more common in people over 30 years of age and can be unilateral or bilateral. Although bilateral elongation is more common, patients with unilateral elongation are usually more symptomatic [5]. Carotid syndrome, which is accompanied by pain along the course of the carotid artery and sometimes tinnitus, may occur due to pressure on the artery during head rotation [15]. The most pronounced symptoms occur when the sympathetic chain, which forms an abundant supply to the walls of the carotid artery, is irritated, manifesting as syncope, ipsilateral head and orbital pain [14]. Compression of the external carotid artery can provoke pain in the area of distribution of the temporal and maxillary processes [6]. The pain is not intense but persistent [15]. For measuring the length of the process, and for differential diagnosis of a fracture from natural segmentation (segmentation) of the styloid process, Computer Tomography (CT) is the most appropriate [7]. A fracture often has uneven edges, whereas segmentation has smooth bone edges on both sides [8]. 3D CT is more appropriate than panoramic radiography in detecting minor fractures of the styloid process [17].
The treatment of the styloid process fracture depends on the length of the process, the location of the fracture, and the degree of dislocation of the distal segment [5,10]. Conservative treatment is appropriate for a styloid process of normal size and includes a soft diet with the use of liquid and soft food, non-steroidal anti-inflammatory drugs, and muscle relaxants. Intermaxillary immobilization for approximately 3-4 weeks is sometimes indicated [8,13]. Surgical treatment in the form of fragment removal through a transpharyngeal approach in the tonsillar fossa is performed in cases of longitudinal or significantly displaced fragments of the styloid process and when conservative treatment is ineffective [10]. The intraoral technique can be performed under local anesthesia and is used if the distal fragment of the styloid process can be palpated in the tonsillar fossa [5]. Initially, a vertical incision is made on the soft palate, and the muscle and ligaments are bluntly separated, exposing the process, which is then secured with a ligature, and the elongated process is shortened with Rongeur forceps [6]. The transcervical approach requires general anesthesia but allows for more adequate visualization and exposure. It is more often used for fractures of elongated styloid processes or when the distal fragment is fused with the hyoid bone. The main disadvantages of this approach are an external scar, increased operation time, and the potential risk of damaging adjacent anatomical structures [5].
Conclusion
A fracture of the styloid process is a rare condition that requires a thorough collection of anamnestic data regarding the mechanism of injury and careful clinical examination of the patients. Fractures of the styloid process of normal length can be encountered in patients with mine-explosion injuries that are accompanied by jerk neck rotation and hyperextension of the cervical spine.
Declarations
Acknowledgements: None.
Ethical considerations: The work described was carried out in accordance with the Code of Ethics of the World Medical Association. It is certified that the referred patient provided verbal consent for the publication of the image and his privacy has been guaranteed.
Funding: The publication of this article has not received funding.
Conflict of interest: None of the authors declare any conflict of interest.
References
- Koshy JM, Narayan M, Narayanan S, Priya BS, Sumathy G. Elongated styloid process: a study. J Pharm Bioallied Sci. 2015; 7(Suppl 1):131–3. doi:10.4103/0975-7406.155861.
- Asherson, N. Glosso-Pharyngeal Neuralgia (Otalgia) and the Elongated Styloid Process: A Record of Five Cases. The Journal of Laryngology & Otology. 1957, 71(07), 453–470. doi:10.1017/s0022215100052014.
- Bacher JA. Styloid process in tosilectomy. Cal State J Med. 1922, 20(3):99. PMID: 18738694; PMCID: PMC1517258.
- Knipe H, Deng F, Hacking C, et al. Styloid process. Reference article, Radiopaedia.org (Accessed on 26 Dec 2023) doi.org/10.53347/rID-28371.
- Miloro, M. Fracture of the styloid process: A case report and review of the literature. Journal of Oral and Maxillofacial Surgery. 1994, 52(10), 1073–1077. doi:10.1016/0278-2391(94)90181-3
- Blythe, J. N. S. J., Matthews, N. S., & Connor, S. Eagle’s syndrome after fracture of the elongated styloid process. British Journal of Oral and Maxillofacial Surgery. 2009, 47(3), 233–235. doi: 10.1016/j.bjoms.2008.08.009.
- Tiwary, P., Sahoo, N., Thakral, A., & Ranjan, U. Styloid Process Fracture Associated with Maxillofacial Trauma: Incidence, Distribution, and Management. Journal of Oral and Maxillofacial Surgery. 2017, 75(10), 2177–2182. doi: 10.1016/j.joms.2017.06.016.
- Dubey KN, Bajaj A, Kumar I. Fracture of the styloid process associated with the mandible fracture. Contemp Clin Dent. 2013, 4(1):116-8. doi: 10.4103/0976-237X.111633.
- Saccomanno, S.; Quinzi, V.; D’Andrea, N.; Albani, A.; Coceani Paskay, L.; Marzo, G. Traumatic Events and Eagle Syndrome: Is There Any Correlation? A Systematic Review. Healthcare 2021, 9, 825. doi: 10.3390/healthcare9070825.
- Reichart, P. A., & Sooss, W. Fracture of the styloid process of the temporal bone: An unusual complication of dental treatment. Oral Surgery, Oral Medicine, Oral Pathology. 1976, 42(2), 150–154. doi:10.1016/0030-4220(76)90117-1.
- Raja, K., Gopi, G., Ramamoorthy, J., Doss, G., Sharma, A., & Panneerselvam, E. Concomitant “Ear Bleed and Styloid Fracture”: An Unusual Complication of Impacted Mandibular Third Molar Removal. Craniomaxillofacial Trauma & Reconstruction. 2016, 10(03), 212–215. doi:10.1055/s-0036-1592086.
- Babbitt, J. A. LVIII. Fracture of the Styloid Process and its Tonsil Fossa Complications, with Report of a Case. Annals of Otology, Rhinology & Laryngology. 1933, 42(3), 789–798. doi:10.1177/000348943304200310.
- Sinberg, S. E., & Burman, M. S. Roentgenologic Visualization of the Fractured Temporal Styloid Process. Radiology. 1945, 45(6), 599–602. doi:10.1148/45.6.599
- Eagle, W. W. Symptomatic Elongated Styloid Process. Report of Two Cases of Styloid Process-Carotid Artery Syndrome with Operation. Archives of Otolaryngology - Head and Neck Surgery. 1949, 49(5), 490–503. doi:10.1001/archotol.1949.0376011.
- Eagle, W. W. Elongated Styloid Process: Further Observations and a New Syndrome. Archives of Otolaryngology - Head and Neck Surgery. 1948, 47(5), 630–640. doi:10.1001/archotol.1948.0069003.
- Eagle, W. W. Elongated Styloid Process: Report of Two Cases. Archives of Otolaryngology - Head and Neck Surgery. 1937, 25(5), 584–587. doi:10.1001/archotol.1937.0065001.
- Hirano K, Mori T, Suzuki T, Hinohira Y, Kobayashi H. A Rare Case of Elongated Styloid Process Fracture. Am J Case Rep. 2020; 21:e925405. doi: 10.12659/AJCR.925405.