
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Bilateral combined laryngocoele: A case report
Suhaima PS1*; Kranti Bhavana2; Bhartendu Bharti3
1Junior Resident, ENT Department, AIIMS, Patna, India.
2Professor & Head of the Department, ENT Department, AIIMS, Patna, India.
3Associate Professor, ENT Department, AIIMS, Patna, India.
*Corresponding Author : Suhaima PS
Junior Resident, ENT Department, AIIMS, Patna,
India.
Email: suhaimaps@gmail.com
Received : Feb 07, 2024
Accepted : Mar 05, 2024
Published : Mar 12, 2024
Archived : www.jcimcr.org
Copyright : © Suhaima PS (2024).
Abstract
Laryngocele, an uncommon condition, involves an abnormal cystic enlargement of the saccule within the larynx, often containing air and communicating with the laryngeal space. It can manifest as internal, external, or mixed types. Here, we present a case of laryngocele that posed a diagnostic challenge initially but was eventually confirmed through radiological examination. Subsequently, the patient underwent surgical intervention via combined approach. Our article underscores the necessity of employing a combined open and Endo laryngeal approach for the comprehensive removal of a mixed laryngocele.
Citation: Suhaima PS, Bhavana K, Bharti B. Bilateral combined laryngocoele: A case report. J Clin Images Med Case Rep. 2024; 5(3): 2916.
Introduction
Laryngeal saccules [1] are extensions of the laryngeal ventricle which help in the lubrication of cords and increase resonance during phonation. Laryngocele is an abnormal cystic dilatation of the saccule. The incidence of laryngocele is one per 2.5 million population [2]. Most of the cases are unilateral but 15% of the cases have bilateral3 presentation. It can be classified as internal if it is lying within the larynx or external if it grows out through the thyrohyoid membrane. Symptoms of internal laryngocele can range from change in voice and minimum difficulty in breathing to stridor and respiratory distress if the laryngocele is completely obstructing the airway. Only 10% of cases have been reported as emergencies warranting tracheostomy [5]. Once the saccule protrudes through the thyrohyoid patients present with complaints of swelling in the neck (Combined laryngocele). However, the incidence of combined laryngocele is rare. Laryngocele could be associated with a laryngeal carcinoma hence it is always important to carry out detailed investigation in patients with laryngocele to rule out any associated malignancy [4].
Case report
A 60-year-old male farmer by profession, presented in emergency in respiratory distress. He was a heavy smoker with a history of change in voice and difficulty in breathing during straining for the last five years which was gradually progressive. For six months he noticed swelling lateral neck associated with difficulty in swallowing. He had no history of using wind instruments or glassblowing. On examination, he was in active stridor. He had bilateral neck swelling anterior to sternocleidomastoid of size 4x4cm on the right and 3x3cm swelling on the left. It was a soft to firm nontender swelling that became prominent on Valsalva maneuver.
Laryngoscopy showed a bulge over the ventricle which was more on the right pushing the epiglottis medially and obscuring the airway. Because of difficult intubation and deteriorating saturation emergency tracheostomy was done to secure the airway. Once the patient was stabilized FNAC was taken from the swelling and CECT neck was done. FNAC from the swelling was done and was reported as a dry tap. CECT showed dilated air spaces in the lateral neck spaces communicating with the bilateral laryngeal ventricles. Diagnosis of bilateral combined laryngocele was made, and the patient was taken up for excision under GA.
Laryngoscopy showed a bulge over the ventricle which was more on the right pushing the epiglottis medially and obscuring the airway. Because of difficult intubation and deteriorating saturation emergency tracheostomy was done to secure the airway. Once the patient was stabilized FNAC was taken from the swelling and CECT neck was done. FNAC from the swelling was done and was reported as a dry tap. CECT showed dilated air spaces in the lateral neck spaces communicating with the bilateral laryngeal ventricles. Diagnosis of bilateral combined laryngocele was made, and the patient was taken up for excision under GA.

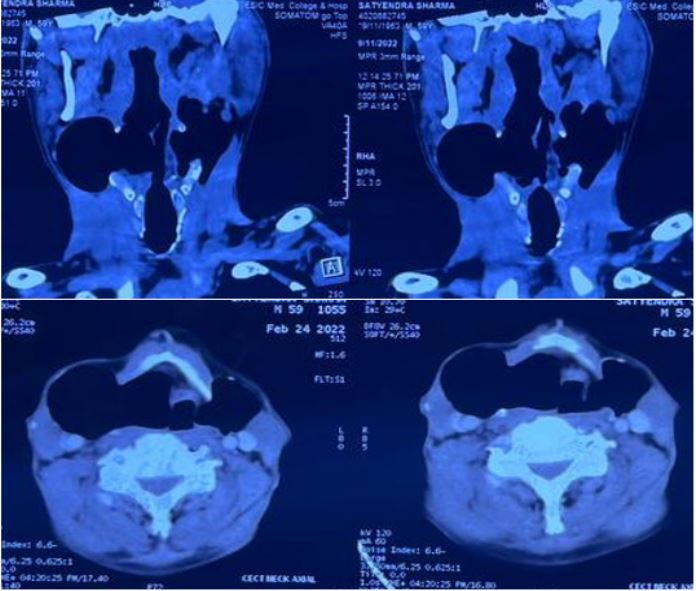




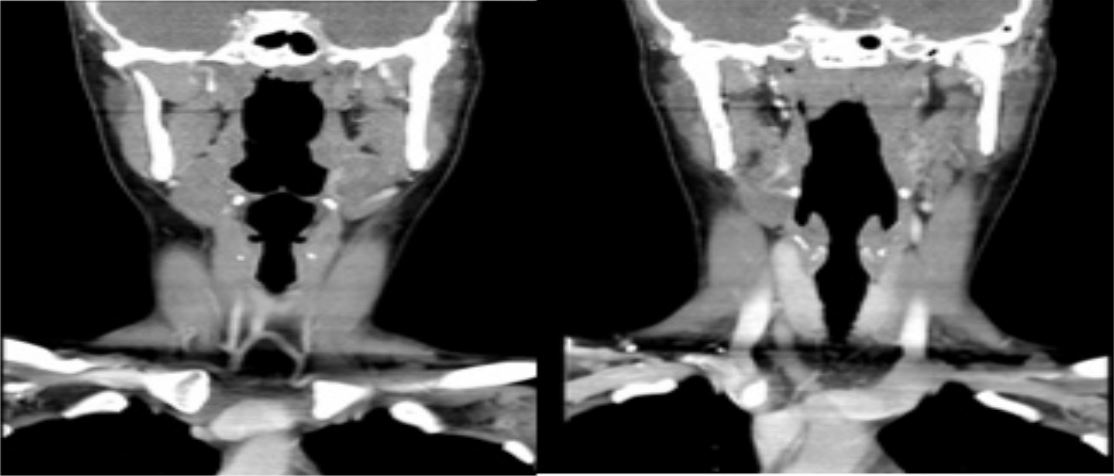
Horizontal skin crease incision was given and subplatysmal flaps were raised. Meticulous dissection of the sac was done. A cartilage window was created in the thyroid lamina and internal component was removed. Small portion of the internal component of laryngocele was removed by MLS excision in the same sitting and complete removal was confirmed.
Sample was then sent for histopathological examination, and it was confirmative for laryngocele. There were no features suggestive of laryngeal carcinoma. Patient was decannulated after one month and was kept under close follow-up for one year. Repeat laryngoscopy and imaging was done and there were no features of recurrence.
Discussion
Laryngoceles are 5-7 times more common in males compared to females and usually present in the sixth decade of life.6 It has a congenital predisposition, but the predisposing factors include increased intralaryngeal pressure like coughing, straining, singing, and playing musical instruments [7]. Incidence of laryngocele concurrent with laryngeal carcinoma, most commonly supraglottic squamous cell carcinoma is reported as 4.9-28.8% [8]. Most of the cases are asymptomatic and are detected incidentally on laryngoscopy or radiological evaluation, whereas some present with hoarseness, sore throat, cough, pain, difficulty in swallowing and difficulty in breathing [9]. They may present in respiratory distress and stridor requiring urgent tracheostomy [10]. Our patient was a 60-year-old farmer with a history of smoking. Commuted tomography is required in all cases of laryngocele to define the relation with surrounding structures and to identify coexistent laryngeal carcinoma, if any [11]. It also helps in differentiating from other cystic lesions of the neck.
Treatment options include excision via Endo laryngeal approach in case of an internal laryngocele and excision via an external approach in case of a combined laryngocele. Initially, all the types were accessed through an external approach [12]. During the last two decades micro laryngoscopic surgery using CO2 laser has become popular for treating internal laryngocoele [13]. It is a quick and precise alternative to the external approach with very less complication and faster recovery. The disadvantage of an endolaryngeal approach includes limited exposure, risk of incomplete excision, and risk of postoperative scarring [14]. When dealing with a combined laryngocele through internal means, it is recommended to first isolate the internal component. Subsequently, the lateral external component can be gradually drawn into the laryngeal lumen through the use of laser mobilization, traction, and blunt micro-surgical dissection. If the mobilized laryngocele proves too bulky to manage endoscopically, a medial and superior excision can be performed, followed by a controlled excision until the entire laryngocele has been successfully removed [13].
Most of the patients with combined or external laryngocele are treated using an external approach. Three types of external procedures have been described, the trans thyrohyoid membrane approach, thyrotomy with resection of the upper 1/3 of the thyroid cartilage, and V-shaped thyrotomy approach [15]. Most commonly used approach is the trans thyrohyoid approach. The purported benefits of utilizing external approaches include superior visualization of the laryngocele, enhanced procedural accuracy, and a reduced incidence of recurrence. Conversely, drawbacks associated with this approach encompass cutaneous scarring, heightened morbidity, prolonged surgical duration, extended hospitalization periods, and increased expenses [15].
Although the external approach has traditionally been the preferred method for managing combined laryngocele, the integration of the endo-laryngeal approach guarantees a thorough excision.
References
- Porter, Paul W, Vilensky, Joel A. The laryngeal saccule: Clinical significance. Clinical Anatomy. 2012; 25.
- Keles E, Alpay HC, Orhan I, Yildirim H Combined laryngocele: a cause of stridor and cervical swelling. Auris Nasus Larynx. 2010; 37: 117-120.
- Suqati A, Alherabi A, Marglani O, Alaidarous T. Bilateral Combined Laryngocele. Saudi Med J. 2016.
- Mitroi M, Capitanescu A, Popescu FC, Popescu C, Mogoanta CA, Mitroi G, etal. Laryngocele associated with laryngeal carcinoma. Rom J Morphol Embryol. 2011; 52:183-185.
- G. Ciabatti, “Transoral robotic surgery for large mixed laryngocoele,The Journal of Laryngology and Otology
- Harvey RT, Ibrahim H, Yousem DM, Weinstein GS. Radiologic findings in a carcinoma-associated laryngocele. Ann Otol Rhinol Laryngol. 1996; 105: 405-8.
- Lancella A, Abbate G, Dosdegani R. Mixed laryngocele: A case report and review of the literature. Acta Otorhinolaryngol Ital. 2007; 27: 255-7.
- Celin SE, Johnson J, Curtin H, Barnes L. The association of laryngoceles with squamous cell carcinoma of the larynx. Laryngoscope. 1991; 101: 529-36.
- Detsouli M, Chelly H, Essaadi M, Mokrim B, Touhami M, Benchekroun Y. Laryngocele as an etiology of respiratory distress. Ann Otolaryngol Chir Cervicofac. 1994; 111: 476-8.
- Pennings RJ, van den Hoogen FJ, Marres HA. Giant laryngoceles: a cause of upper airway obstruction. Eur Arch Otorhinolaryngol. 2001; 258: 137-40.
- Akbas Y, Unal M, Pata YS. Asymptomatic bilateral mixed-type laryngocele and laryngeal carcinoma. Eur Arch Otorhinolaryngol 2004; 261: 307-9.
- Myssiorek D, Madnani D, Delacure MD. The external approach for submucosal lesions of the larynx. Otolaryngol Head Neck Surg. 2001; 125(4): 370-373. doi: 10.1067/mhn.2001.118690.
- Devesa PM, Ghufoor K, Lloyd S, Howard D. Endoscopic CO2 laser management of laryngocele. Laryngoscope. 2002; 112(8,1): 1426-1430. doi: 10.1097/00005537-200208000-00018.
- Szwarc BJ, Kashima HK. Endoscopic management of a combined laryngocele. Ann Otol Rhinol Laryngol. 1997;106(7-1): 556-559. doi: 10.1177/000348949710600704.
- Thomé R, Thomé DC, De La Cortina RAC. Lateral thyrotomy approach on the paraglottic space for laryngocele resection. Laryngoscope. 2000;110(3-1): 447-450. doi: 10.1097/00005537-200003000-00023.