
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Placental site trophoblastic tumor with lung metastasis: A case report and literature review
Xin Wang1,2; Qiulin Tang2; Xue Shao1,2; Lingling Han1,2; Guiqing Chen2; Shuang Luo2*
1Chengdu University of Traditional Chinese Medicine, No.1166, Willow Terrace Avenue, Wenjiang District, Chengdu City, 610000, Sichuan Province, China.
2Department of Gynecology, Suining Central Hospital, No. 127 Desheng West Road, Chuanshan District, Suining, 629000, Sichuan Province, China.
*Corresponding Author : Shuang Luo
Department of Gynecology, Suining Central Hospital, No. 127 Desheng West Road, Chuanshan
District, Suining, 629000, Sichuan Province, China.
Email: 79622499@qq.com
Received : Feb 19, 2024
Accepted : Mar 05, 2024
Published : Mar 12, 2024
Archived : www.jcimcr.org
Copyright : © Luo S (2024).
Abstract
Placental Trophoblastic Tumor (PSTT) is a rare Gestational Trophoblastic Disease (GTD), which is uncommon in clinical practice. Imaging examinations show no specificity, and it may metastasize to the lung, liver, vagina, or uterine adnexa. Patients with metastasis often face challenges in diagnosis, and the final diagnosis depends on histopathological examination. Lung metastasis is one of the most common sites. We describe the case of a 46-year-old female patient with PSTT and lung metastasis which mechanism is complex, without heterogeneity, but successfully treated with radical hysterectomy and postoperative chemotherapy. The case highlights:
(1) The difficulty in the preoperative diagnosis of PSTT, requiring multiple tissue biopsies.
(2) Imaging suggests the possibility of pulmonary metastasis, necessitating multidisciplinary management.
(3) Monitoring serum β-HCG levels and the size of metastatic lesions was instructive for early diagnosis, outcome evaluation, and follow-up.
Keywords: PSTT; Metastatic lung tumor; Serum β-HCG; Medical Imaging.
Citation: Wang X, Tang Q, Shao X, Han L, Chen G, et al. Placental site trophoblastic tumor with lung metastasis: A case report and literature review. J Clin Images Med Case Rep. 2024; 5(3): 2917.
Introduction
Placental Site Trophoblastic Tumor (PSTT), also known as atypical choriocarcinoma, syncytioma, chorioepitheliosis or trophoblastic pseudotumor, is a rare gestational trophoblastic disease (0.25-5% of all trophoblastic tumors) [1]. The incidence of Placental Site Trophoblastic Tumor (PSTT) is about 1 in one hundred thousand [2]. The specific pathogenesis is unclear. This paper reports a case of PSTT treated in our hospital.
Case characteristics
On March 9, 2022, a 46-year-old Chinese woman was admitted to the Suining Central Hospital with mild uterine bleeding. Her previous menstrual cycle was 30 days, the duration is about 5 days. Following a thorough examination, diagnostic curettage was performed. Her chemical report showed a serum β-HCG level >10,000 mIU/mL. Ultrasound revealed heterogeneous lesions measuring approximately 4.3×2.4 cm inside the uterine cavity. Scraping biopsies indicated cellular proliferation and degeneration of trophoblast cells. Post operative month-1, the patient experienced abdominal pain, The patient was sexually active during this period, prompting consideration of ectopic pregnancy. The outside hospital an emergency procedure was conducted, involving abdominal bilateral salpingectomy + right cornual pregnancy lesion resection. The serum β-HCG was going up, postoperative serum β-HCG was 34,994.0 mIU/mL. Pathological examination revealed a large number of highly proliferative and active trophoblast cells in the right horn lesion. Post operative day-44, during an outpatient visit to our hospital, the patient’s serum β-HCG was 171,438 mIU/mL. Ultrasound showed an anterior-posterior diameter of the uterus measuring 5.0 cm. In the uterine cavity, a 1.5 cm-wide strip of heterogeneous slightly strong echo was observed, accompanied by punctate blood flow signals. The muscle wall echo was uniform, with no exact occupying in the body. Additionally, a liquid dark area of 7.8 cm × 3.2 cm was found in the pelvic cavity. Chest enhanced CT revealed multiple small nodules in both lungs, with the larger one measuring about 1.2 cm × 0.7 cm. The enhanced scan indicated mild enhancement, raising suspicions of metastasis (Figure 1). The admission diagnosis was invasive hydatidiform mole with pulmonary metastasis. On April 26, 2022, the patient experienced massive vaginal bleeding at night, leading to an emergency total abdominal hysterectomy. Intraoperative findings included uterine enlargement resembling a 2-month pregnancy, soft texture, cervical enlargement, and a surgical wound in the right uterine horn measuring about 4×3 cm. The intraoperative section of the uterus revealed a polypoid neoplasm about 1.5×1.0×1.0 cm in the uterine cavity, with a poorly defined boundary, surrounding tissue, and focal bleeding and necrosis (Figure 2). Postoperative pathology confirmed a uterine placental trophoblastic tumor, with no involvement of the cervical canal, and the presence of vascular thrombus. TP/TE chemotherapy was administered from May 27, 2022, to December 12, 2022 (The recommended dose schedule for TP/TE is paclitaxel 230 mg/m2 ; cisplatin 100 mg/m2 ; and etoposide 200 mg/m2 once weekly for 2 weeks, repeated every 4 weeks). The chemotherapy process was smooth, with dynamic reexamination of serum β-HCG gradually decreasing to normal (Table 1). Chest CT reexamination showed that the lesions were shrunk (Figure 3).
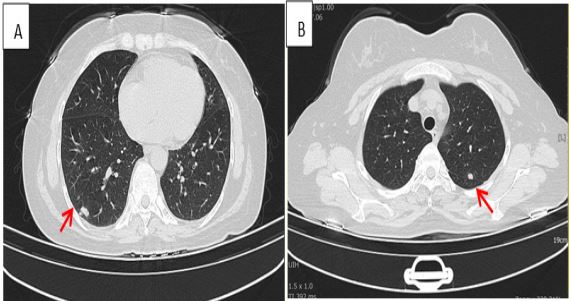
A)arrow indicates right lung lesion.
B)arrow indicates left lung lesion

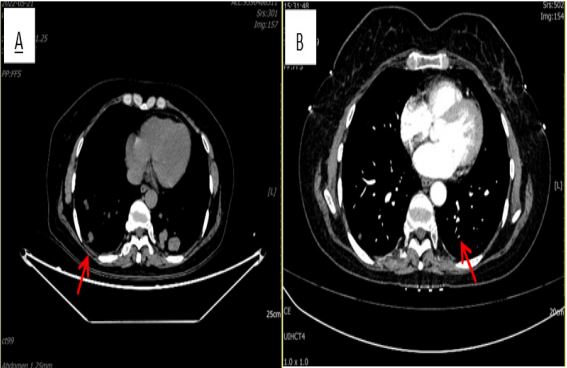
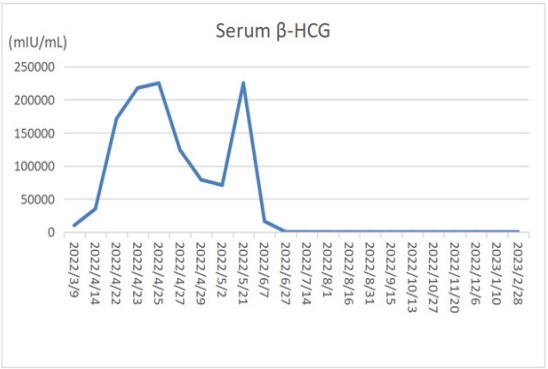
Table 1: The basic situation of some PSTT patients with metastasis was summarized.
| Age | Transferring site | β-HCG (mlu/ml) |
Imaging examination |
Treatment | Prognosis | Other | |
|---|---|---|---|---|---|---|---|
| 1 | 44 | breast | 900 | Ultrasound, CT |
total abdominal
hysterectomy with left salpingo-oophorectomy +a single dose of methotrexate chemotherapy |
alive without recurrence |
|
| 2 | 27 |
pulmonary arteriovenous |
Unknown (positive) | Chest x-ray, CT | An en-bloc right middle lobectomy | alive |
Early diagnosis with lung disease as the main symptom |
| 3 | 29 | Vagina | 124.1 | US,PET-CT |
chemotherapy ( etoposide,
metho- trexate, cyclophosphamide, and Vincristine) |
alive |
Early misdiagnosis as poorly differentiated squamous cell carci- noma |
| 4 | 40 | vaginal metastasis | >200000 | US,PET-CT |
Chemotherapy of 5-Fu+KSM+ cervical LEEP surgery |
alive |
molar pregnancy--ETT-- PSTT |
| 5 | 31 | gallbladder | 95.4 | MRI |
A total abdominal
hysterectomy with a bilateral salpingo-oophorec- tomy was performed. |
alive |
Early manifestations are lupus nephritis |
| 6 | 43 |
ovaries, lungs, kidneys, adrenals, and pancreas. |
3189 | CT |
surgery and an extensive
subse- quent chemotherapy |
died | |
| 7 | 32 | gallbladder | 289 | US,CT,MRI |
total
hysterectomy+chemotherapy +hysteroscopy |
alive |
Nephrotic syndrome before |
| 8 | 37 | liver | 857 |
US,CT, Hysteroscopy |
abdominal Hysterectomy
+bilateral salpingectomy+chemotherapy |
alive |
paraneoplastic syn- dromes may herald or accompany a diagnosis of PSTT |
Discussion
Diagnosis: PSTT is a unique trophoblastic tumor originating from the placental implant site. It is commonly found in women of childbearing age and is often characterized by irregular vaginal bleeding, and in severe cases, excessive bleeding. Biopsies typically reveal ill-defined boundaries on a polypoid or endogenous intrauterine mass with hemorrhage and necrosis. Intermediate trophoblastic cells can be observed under the microscope [3,4]. PSTT is predominantly composed of intermediate trophoblastic cells with few syncytiotrophoblastic cells. Serum β-HCG, mainly produced by syncytiotrophoblastic cells, is mostly negative or slightly elevated in PSTT [4]. This characteristic makes it easily confused with invasive hydatidiform moles and choriocarcinoma. Both PSTT and ETT are less chemosensitive than choriocarcinoma. Pregnancy-associated Major Basic Protein (PMBP), a marker of intermediate trophoblast, is useful in distinguishing PSTT from other forms of Epithelial Trophoblastic Tumors (ETT) [5]. However, the final diagnosis relies on histopathological examination. The patient in our report was diagnosed with an invasive mole based on the significantly elevated serum β-HCG level combined with biopsy testing (Table 1) . Subsequently, we analyzed eight cases of PSTT with metastasis reported in PubMed over the last 10 years. Serum β-HCG was positive in all eight patients at the early stage with varying degrees of elevation. Only one case showed a serum β-HCG increase of more than 200,000 mIU/mL (Table 2). Our findings suggest that the positive level of serum HCG cannot be solely used as a criterion for diagnosing PSTT, nor can it be used for the differential diagnosis of PSTT, invasive mole, and choriocarcinoma. However, studies have shown that blood HCG levels will also increase in patients with PSTT as the metastatic sites progress [6]. Clinical serum HCG positivity can be used as one of the indicators of PSTT with some organ metastasis and for assessing the severity of the disease after treatment [7]. Literature from the past decade suggests that PSTT often metastasizes to the lung, vagina, brain, liver, and other sites [8]. Patients often seek treatment due to clinical symptoms of metastasis, and imaging findings without specificity, leading to delayed diagnosis or misdiagnosis, sometimes requiring multiple histopathological examinations. The patient we reported was finally diagnosed after three biopsies. PSTT metastasis often occurs in the late stage, resulting in a poor prognosis, which also affects psychology [9].
For Gestational Trophoblastoma Neoplasia (GTN) with atypical clinical features, curettage can easily miss small intrauterine lesions, wide root lesions, and lesions located in the uterine horn. Hysteroscopy is an alternative and safe method helpful for the diagnosis and differential diagnosis of GTN [10-12]. The patient was admitted to another hospital on March 9, 2022; her serum β-HCG was more than 10,000 mIU/mL. Transvaginal ultrasound showed abnormal echoes in the uterine cavity, approximately 4.3×2.4 cm in size. Scraping biopsies revealed cellular proliferation and degeneration of trophoblast cells. The postoperative examination indicated a very small amount of villi tissue and flaky trophoblast cells with active proliferation and degeneration in the intrauterine. For patients suspected of suffering from GTN, hysteroscopy can detect, diagnose, and treat GTN as early as possible, reducing the risk of metastasis. The surgery has no significant effect on the outcome of patients with GTN. Simultaneously, it can effectively treat non-GTN diseases and improve patient prognosis [13].
Therefore, GTN patients lack pathological results to support chemotherapy. If the decline in serum β-HCG is not significant, PSTT with organ metastasis should be considered promptly. Completing a histopathological examination as soon as possible is necessary, improving prognosis through comprehensive treatment based on surgery and chemotherapy [8].
Treatment: Usually, surgery is the primary choice for treating placental trophoblastic tumors. The principle is to remove all lesions, and the surgical scope includes total hysterectomy and bilateral adnexectomy. Salvage hysterectomy can also be chosen for patients with local metastasis who desire fertility, followed by postoperative adjuvant chemotherapy [3]. PSTT with metastasis is a high-risk factor for poor prognosis and requires postoperative adjuvant treatment. A review of the literature in the past 10 years shows that surgical resection of the primary lesion is the main method, followed by adjuvant chemotherapy. EMA/CO (etoposide, methotrexate, actinomycin-D, cyclophosphamide, vincristine), EMA/EP (etoposide, methotrexate, actinomycin-D, cisplatin), or FAEV regimen (floxuridine, actinomycin-D, etoposide, vincristine) are the main chemotherapy regimens [3,4]. Some PSTT patients with metastasis can be treated with single-agent chemotherapy (single-dose methotrexate or single-drug actinomycin-D) after surgical resection of the lesion, and the prognosis is good [14]. However, it has been documented that in patients with a single lung metastasis with a PSTT component, we suggest lung metastasectomy not followed by adjuvant chemotherapy. Multicenter studies are needed to create guidelines for the treatment of metastatic disease in this uncommon tumor type [15]. The 46-year-old middle-aged woman who presented massive vaginal bleeding underwent emergency hysterectomy. Confusingly, postoperative serum HCG increased, and the computed tomography enhanced scan indicated metastatic lesions. After the combination treatment of TP/TE regimen, her pulmonary lesion was smaller than before, and the serum HCG was normal. In this case, due to actinomycin-D deficiency and severe side effects, TP/TE was used with the dose adjusted according to the state of the illness (The recommended dose schedule for TP/TE is paclitaxel 230 mg/m2 ; cisplatin 100 mg/m2 and etoposide 200 mg/m2 once weekly for 2 weeks, repeated every 4 weeks). It has good efficacy and few side effects. Literature studies have shown that patients with PSTT with extrauterine metastasis are at risk of recurrence and need regular follow-up examinations [2,3].
Conclusion
PSTT with metastasis is rare and lacks imaging specificity, making it prone to delayed diagnosis or misdiagnosis. The diagnosis depends on histopathological examination, and the treatment mainly involves a combination of surgery and chemotherapy. The elevation of serum β-HCG is common in patients with metastasis, providing guidance for early diagnosis, evaluation of therapeutic effects, and follow-up.
Declarations
Author contributions: All authors listed have significantly contributed to the investigation and writing of this article.
Acknowledgments: We wish to acknowledge the support of the Chengkun Yin of the Department of Imaging for his support.
Declaration of competing interest: The authors have stated explicitly that there are no conflicts of interest in connection with this article.
Patient consent statement: Written informed consent was obtained from the patient.
References
- Zampacorta C, Pasciuto MP, Ferro B, et al. Placental site trophoblastic tumor (PSTT): a case report and review of the literature. Pathologica. 2023; 115(2): 111-116. doi:10.32074/1591-951X-873
- Zhao J, Xiang Y. Placental trophoblastic tumor and its diagnosis and treatment[J]. Journal of Practical Oncology, 2008, 23(1): 5-7.
- Jiang S, Zhao J, Shi X, et al. Retrospective analysis of clinical features and fertility outcomes with fertility-sparing treatment of placental site trophoblastic tumor. Gynecol Oncol. 2023; 171: 1-8. doi:10.1016/j.ygyno.2023.02.002
- Guidelines for the diagnosis and treatment of gestational trophoblastic disease[J]. Chinese Journal of Cancer. 2021; 31(6): 520-532.
- Bouquet de la Jolinière J, Khomsi F, Fadhlaoui A, et al. Placental site trophoblastic tumor: a case report and review of the literature. Front Surg. 2014; 1: 31. Published 2014 Aug 27. doi:10.3389/fsurg.2014.00031
- Shen XY, Ren T, Xiang Y. Value of human chorionic gonadotropin in the diagnosis and treatment of placental trophoblastic tumors[J]. Chinese Clinical Journal of Obstetrics and Gynecology. 2012; 13(3): 198-201.
- De Nola R, Schönauer LM, Fiore MG, et al. Management of placental site trophoblastic tumor: Two case reports. Medicine (Baltimore). 2018; 97(48): e13439. doi:10.1097/MD.0000000000013439
- Zheng RL, Wang HB, Lu CH, et al. Analysis of trophoblastic tumor in placenta site[J]. Chinese science and technology periodical database. (SciFinder Scholar) Health & Medicine. 2023(5): 0036-0038.
- Fathaddin AA, Arafah MA. A malignant placental site trophoblastic tumor of the uterus with multiple metastases: A case report of a rare tumor showing an aggressive behavior. Indian J Pathol Microbiol. 2019; 62(1): 142-145. doi: 10.4103/IJPM.IJPM_45_18.
- Feng FZ, Xiang Y, He HJ, et al. Value of hysteroscopy and laparoscopy in differential diagnosis of gestational trophoblastic neoplasia. Zhonghua Fu Chan Ke Za Zhi. 2007; 42(7): 464-7.
- Zhu TT, Wang Q, Lu X. Application value of hysteroscopy in differential diagnosis and treatment of gestational trophoblastic tumor[J]. Chinese Journal of Minimally Invasive Surgery. 2018; 18(11): 978-981.
- Sardo ADS, Calagna G, Di Carlo C. Tips and tricks in office hysteroscopy. Gynecol Minim Invasive Ther. 2015; 4: 3e7.
- Gu Y, Femg FZ, Xiang Y et al. Application of laparoscopy and/or hysteroscopy in differential diagnosis and treatment of suspected gestational trophoblastic tumors [J]. Journal of Concord Medicine, 2016; 7(04): 253-258.
- Nagamine K, Iwasaki S, Shimizu D, et al. Placental site trophoblastic tumor with sole metastasis to breast: A case report. 2017; 21: 86-90. doi: 10.1016/j.gore.2017.07.003.
- Billè A, Girelli L, Colecchia M, Pastorino U. Single synchronous pulmonary metastasis from placental site trophoblastic tumor and teratoma. Tumor. 2015; 101(3): e110-e111. Published 2015 Jun 25. doi:10.5301/tj.5000290.