
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Acute emergence of a post-phacoemulsification inflammatory membrane: Ophthalmological enigma revealed
Krichene Amine*; Robbana L; Hassina S; Tebbay N; Akannour Y; Serghini L; Abdellah E
University Mohammed V Rabat, Morocco.
*Corresponding Author : Krichene Amine
University Mohammed V Rabat, Morocco.
Email: drkrichene.m.amine@gmail.com
Received : Jan 09, 2024
Accepted : Mar 06, 2024
Published : Mar 13, 2024
Archived : www.jcimcr.org
Copyright : © Amine K (2024).
Abstract
Purpose: This case reports the manifestation of a postoperative inflammatory membrane in a 75-year-old patient with a grade 3 corticonuclear cataract and pseudoexfoliations. The aim of this study is to discuss complications associated with pseudoexfoliations during cataract surgery and therapeutic approaches.
Case report: The patient, a type 2 diabetic, presented with a bilateral decrease in visual acuity. Ophthalmological examination revealed pseudoexfoliations impeding pupillary dilation. After phacoemulsification with iris retractors, a postoperative inflammatory membrane developed in the right eye, leading to corneal edema, elevated intraocular pressure and reduced visual acuity.
Discussion: Pseudoexfoliations complicate cataract surgery by limiting pupillary dilation, increasing the risk of complications such as capsular rupture or zonulopathy. The inflammatory membrane, which differs from cyclitic inflammations, probably results from an abnormal immune response to pseudoexfoliative material. Corticosteroids are used for their anti-inflammatory and anti-fibrotic effect, and surgery may be required in cases of resistance to treatment.
Conclusion: Postoperative inflammatory membrane in patients with pseudoexfoliations during cataract surgery represents a serious complication requiring prompt recognition and appropriate corticosteroid treatment, underlining the crucial importance of early management to improve visual prognosis and reduce long-term complications.
Citation: Amine K, Robbana L, Hassina S, Tebbay N, Akannour Y, et al. Acute emergence of a post-phacoemulsification inflammatory membrane: Ophthalmological enigma revealed. J Clin Images Med Case Rep. 2024; 5(3): 2918.
Introduction
Pseudoexfoliations (PXF) represent a major challenge for ophthalmologists due to the potential complications associated with cataract surgery. Fibrillar deposits in pseudoexfoliations can make the surgical procedure more difficult, notably by reducing pupillary dilation and increasing the risk of intraoperative complications. To overcome these problems, various methods have been investigated, including the use of iris retractors to make cataract surgery easier in these patients.
Case report
A 75-year-old woman with a history of well-balanced type 2 diabetes and glycated hemoglobin of 6.5% on oral antidiabetic therapy. She presented with a bilateral visual acuity drop of 2/10 in the Right Eye (RE) and 3/10 in the Left Eye (LE). On ophthalmological examination of the anterior segment of both eyes, the cornea was clear and the anterior chamber was calm with good depth. However, both eyes (RLE) showed grade 3 cortico-nuclear cataracts and pseudoexfoliations preventing proper pupillary dilation. The fundus was not perfectly accessible but appeared without abnormalities. AB ultrasound was performed and returned normal on RLE.
The patient underwent RE phacoemulsification to remove the lens, using iris retractors to improve dilation. The patient was implanted without intraoperative complications or posterior capsule rupture.
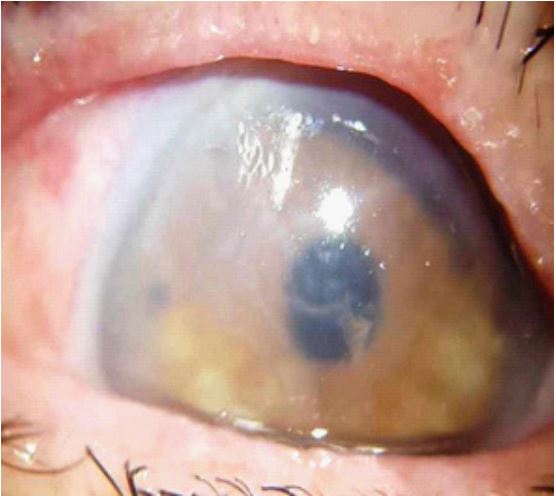
On postoperative day 1, mild corneal edema was noted, with an inflammatory-looking membrane just retro-corneally in the anterior chamber of the OD, without Tyndall and Intraocular Pressure (IOP) at 22 mmHg.
The patient was treated with hourly eye drops of corticosteroids for 24 hours, then 8 drops a day, with subconjunctival injections of corticosteroids once a day for 3 days. On postoperative day 5, the membrane began to shrink, and the IOP fell to 18 mmHg. An additional corticosteroid injection was performed. At 10 days post-operatively, the membrane had disappeared and there was an improvement in ocular redness. Post-operative treatment was continued in a normal fashion for 3 weeks, and OD visual acuity became 10/10 with a correction of +1.00 dioptres.
Discussion
Ophthalmic surgeons face a major challenge when cataract patients present with pseudoexfoliations, due to the potential complications associated with this condition. The accumulation of fibrillar material in various ocular structures characterizes pseudoexfoliations, which have an impact on the stability of cataract surgery. One of the main concerns of patients with pseudoexfoliation during cataract surgery is difficulty dilating the pupil. An unresponsive pupil may be caused by the presence of fibrillar deposits, making pupillary dilation more difficult and increasing the risk of intraoperative complications such as capsular rupture or zonulopathy. According to Shingleton et al., to overcome this problem, the use of iris retractors and other specific pupillary dilation methods can be considered to facilitate the surgical procedure [7].
Our case illustrates a serious but rare complication of cataract surgery in patients with PXF. The postoperative inflammatory membrane is different from the cyclitic membrane, which is more common in patients with neovascular glaucoma or chronic uveitis. A distinctive sign of an inflammatory membrane is an intense inflammatory reaction on the inflammatory membrane, which may be confused with endophthalmitis but is distinguished by the absence of infectious signs such as fever, leukocytosis, or positive blood cultures. A whitish or greyish fibrous membrane, located in front of the lens or implant and behind the cornea, can be seen on biomicroscopic examination for diagnosis. The membrane may be associated with hypopyon, Tyndall effect, iridocapsular synechia, uveitis, or phacolysis [1].
Although the mechanism of inflammatory membrane formation has not been fully elucidated, it suggests an unusual immune response to antigens released during phacoemulsification, in particular pseudoexfoliative material [2].
An unusual product of cellular metabolism called pseudoexfoliative material is deposited on ocular structures and possesses pro-inflammatory and pro-fibrotic characteristics [1]. It has the potential to activate immune cells, generate cytokines, stimulate fibroblasts, and produce collagen [1]. In addition, pseudoexfoliative material has the potential to disrupt the functioning of the blood-aqueous barrier and promote the entry of antigens into the anterior chamber [2]. Other factors may contribute to the formation of the inflammatory membrane, such as surgical trauma, mechanical irritation of the implant, the presence of foreign bodies, or viscoelastic residues [3].
Local and systemic corticoids have an anti-inflammatory and anti-fibrotic effect [4] in the treatment of inflammatory membranes. The severity and evolution of the membrane should determine the dosage and duration of treatment. In the event of resistance or recurrence, further surgery to remove the membrane may be required, which may be performed either anteriorly or posteriorly, depending on the location and extent of the membrane [5]. Complications of surgery include capsular rupture, vitreous loss, decentering or dislocation of the implant, macular edema, endophthalmitis, or retinal detachment [6].
The visual prognosis of inflammatory membranes varies according to the speed of diagnosis, the effectiveness of treatment, and the occurrence of complications. Following medical or surgical treatment, some authors describe a complete recovery of visual acuity, while others describe irreversible visual loss due to optic nerve atrophy, secondary cataracts, glaucoma, or retinopathy [6]. Good patient preparation, rigorous surgical technique, irrigation-ablation of pseudoexfoliative material, and anti-inflammatory prophylaxis are all means of preventing inflammatory membrane disease [6]. Thus, it is crucial to recognize this entity and treat it correctly.
The surgical approach for patients with pseudoexfoliation is always influenced by technological advances. Research is focusing on the creation of new devices to maximize pupillary dilation. Innovative pre-treatment methods may also emerge to reduce the burden of pseudoexfoliative deposits prior to surgery. In addition, in-depth studies into the immunological mechanisms responsible for postoperative inflammatory membrane formation could lead to more effective targeted therapies, reducing complications and improving long-term outcomes.
Conclusion
In patients with pseudoexfoliation, post-operative inflammatory membranes are a rare but serious complication of cataract surgery. It manifests as a severe inflammatory reaction that can lead to reduced visual acuity, ocular hypertonia, and other complications. Diagnosis is based on biomicroscopic examination, and treatment is based on the administration of local and systemic corticosteroids or even reoperation. The visual prognosis varies according to the speed of diagnosis, the effectiveness of treatment, and the occurrence of complications. It is therefore crucial to recognize this entity and treat it correctly.
References
- Ritch R, Schlötzer-Schrehardt U. Exfoliation syndrome. Surv Ophthalmol. 2001; 45(4): 265-315.
- Shingleton BJ, Crandall AS, Ahmed II. Pseudoexfoliation and the cataract surgeon: preoperative, intraoperative, and postoperative issues related to intraocular pressure, cataract, and intraocular lenses. J Cataract Refract Surg. 2009; 35(6): 1101-20.
- Asano S, Miyake K, Ota I, Sugita G, Kimura W, Horiguchi M, et al. Reducing the risk of intraoperative complications in patients with pseudoexfoliation syndrome. J Cataract Refract Surg. 2006; 32(4): 633-7.
- Kanski JJ, Bowling B. Clinical Ophthalmology: A Systematic Approach. 8th ed. Elsevier. 2016.
- Foster CS, Vitale AT. Diagnosis and Treatment of Uveitis. 2nd ed. Jaypee Brothers Medical Publishers. 2013.
- Kothari M, Jain S, Shah N. Postoperative fibrinous membrane over intraocular lens in a patient with pseudoexfoliation. Indian J Ophthalmol. 2009; 57(4): 311-3.
- Shingleton BJ, Crandall AS, Ahmed II. Pseudoexfoliation and the cataract surgeon: preoperative, intraoperative, and postoperative issues related to intraocular pressure, cataract, and intraocular lenses. J Cataract Refract Surg. 2009 ; 35(6): 1101-20. doi: 10.1016/j.jcrs.2009.03.011. PMID: 19465298.