
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Schwannoma of the pterygopalatine fossa: Transfacial approach and maxillary swing technique
Noemí Vieira-Sebe; Anna Maria Simón-Flores; Guillermo García-Serrano*; Mario Pezzi Rodriguez; Julio Acero-Sanz
Department of Oral and Maxillofacial Surgery, Puerta de Hierro Majadahonda Hospital, Madrid, Spain.
*Corresponding Author : Guillermo García-Serrano
Department of Oral and Maxillofacial Surgery,
Puerta de Hierro Majadahonda Hospital, Madrid,
Spain.
Email: garciaserranomaxilofacial@gmail.com
Received : Feb 23, 2024
Accepted : Mar 08, 2024
Published : Mar 15, 2024
Archived : www.jcimcr.org
Copyright : © García-Serrano G (2024).
Abstract
The pterygopalatine fossa is a complex anatomic space related to the skull base. Primary and secondary tumors can be located in this area. The approach to this space can be challenging due to its anatomy and neurovascular relations. The aim of this paper is to describe systematically the maxillary swing technique used in the resection of a V2 Schwannoma located in the right pterygopalatine fossa. With this report we want to highlight that this classic approach should we considered in the management of Deep facial spaces when endoscopic approach cannot be performed.
Keywords: Pterygopalatine fossa; Maxillary swing; Transfacial approach; Schwannoma.
Citation: Vieira-Sebe N, Simón-Flores AM, García-Serrano G, Rodriguez MP, Acero-Sanz J. Schwannoma of the pterygopalatine fossa: Transfacial approach and maxillary swing technique J Clin Images Med Case Rep. 2024; 5(3): 2925.
Introduction
The pterygopalatine fossa (PPF) is a shaped like inverted quadrangular pyramid anatomical space found at the skull base. It is located between the maxilla, palatine, and sphenoid bones. It is limited by the maxillary tuberosity anteriorly, by the pterygoid process posteriorly, by the perpendicular plate of the palatine bone medially, and by the greater wing of the sphenoid bone superiorly. It is communicated superiorly with the inferior orbital fissure, posteriorly with the retropharyngeal space, and laterally with the pterygomaxillary fissure, which continues into the infratemporal fossa. The maxillary nerve (V2), the pterygopalatine ganglion, the most distal portion of the internal maxillary artery, and veins that drain into the pterygoid plexus are found into this cavity. Primary tumors of the PPF are rare. Usually, tumors found in this location are originated in nearby areas and extend into the PPF, for example, nasosinusal tumors or those originating in structures of the skull base. Tumors affecting the PPF can either be benign (angiofibromas, Schwannomas, or neurofibromas) or less frequently, malignant (adenoid cystic carcinomas and sarcomas) [1]. Schwannomas of the PPF are usually primary tumors of this location. They most commonly originate from the V2 branch of the trigeminal nerve. They are slow glowing benign tumors formed by a proliferation of Schwann cells. Head and neck Schwannomas typically stem from the peripheral portion of cranial nerves V, VII, IX, X, XI, and XII sympathetic chains, and cervical and brachial plexuses2. Sensory nerves are most frequently affected, while motor nerves affection is usually associated with neurofibromatosis3. Malignant transformation of this type of tumor is uncommon, with an incidence ranging from 8-13% [2].
Clinical case
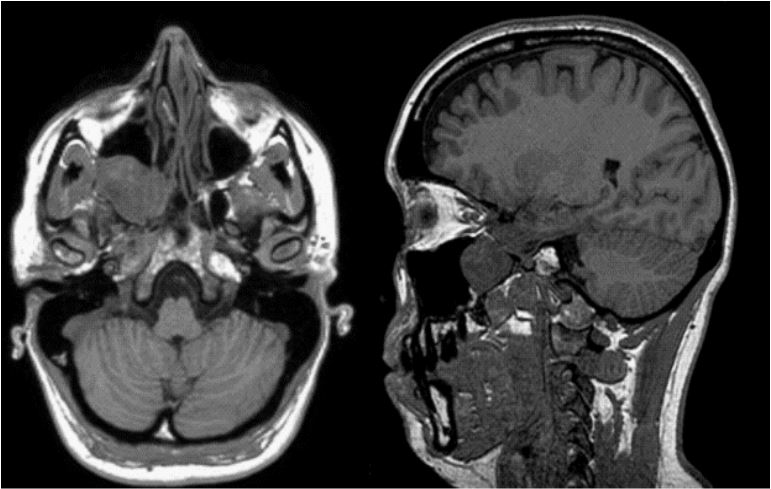
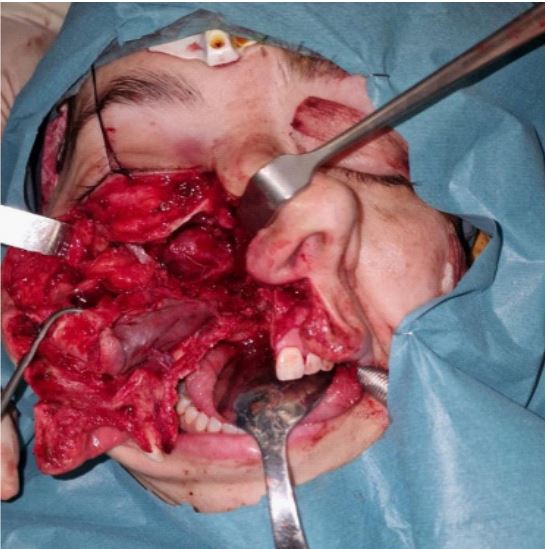
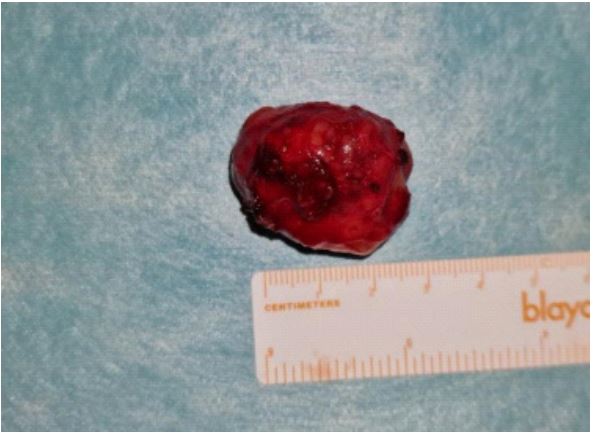
We report the case of 46-year-old woman who presented with right infraorbital nerve hypoesthesia for months. An MRI was performed which showed the presence of a 3.5 cm mass located in the right PPF suggestive of a V2 Schwannoma. An additional CT scan was performed that confirmed the existence of the mention mass and allowed for a more precise definition of the involvement of the surrounding bone (Figure 1). Considering the location and size of the mass, the resection of the tumor was assisted by an intraoperative navigation system and performed through a transfacial approach with a modified Weber-Ferguson incision with a subciliarly extension, keeping the facial soft tissues attached to the adjacent bone, followed by the maxillary swing technique. Miniplates were placed prior to the osteotomies (“preplatting”) to allow for the exact repositioning of bone segments. Osteotomies were performed using a piezoelectric system between the two central incisors to the floor of the nasal fossa, between the nasal vestibule and the nasal process; from the zygomatic arch 5 mm below the inferior orbital rim to the nasal osteotomy; from the most lateral portion of the infraorbital osteotomy to the total thickness of the zygomatic bone, and finally, an osteotomy was performed in the midline of the hard palate. Pterygomaxillary disjunction was then performed. Afterwards, the maxilla was mobilized laterally to expose the right pterygopalatine fossa, and the tumor was visualized (Figure 2) and removed through careful dissection. In this case, it was not possible to preserve the V2 branch, as it was completely included inside the tumor. The internal maxillary artery was identified and preserved. The maxillary bone was then repositioned, and osteosynthesis was performed with miniplates placed on the zygomatic arch, nasal process, and midline of the maxillary alveolar bone according to the preoperative design. Closure of the incision was done with absorbable and Nylon sutures. The postoperative recovery of the patient was favorable, presenting with hypoesthesia of the right infraorbital nerve, epiphora, and mild lagophthalmos after the intervention, and she was discharged on the 4th day after surgery. The patient showed improvement of the epiphora and lagophthalmos in the following weeks. The result of the histological study of the specimen was consistent with Schwannoma (Figure 3).

Discussion
Accessing the PPF is challenging due to its anatomy and neurovascular relations. Because of this, many approaches have been described for resecting tumors in this area. The classical “maxillary swing” technique, described by von Langenbeck and popularized by Hernández Altermir in his 19864 description, provides a safe alternative for approaching tumors located in this region. Other open approaches described in the literature to reach this anatomical region include the Lefort I and II osteotomies, the transmaxillary approach, paralateronasal rhinotomies, middle third facial degloving and lateral facial split. In the last decades the use of endoscopic-assisted surgery has increased because its efficiency, lower morbidity and possibility of using it combined with an open approach [5-9]. However, if endoscopic technique is not available or in cases with large tumor sizes and complex anatomical locations, the open approach could be an alternative offering a good control of the surgical área [10]. The maxillary swing technique consists of temporary mobilization of the maxilla offering a wide vision of the PPF, allowing a safer approach to the vasculo nervous structures in the area. Furthermore, this approach can be combined with other accesses for the removal of lesions located in the PPF that extend to other intra- and extracranial locations [5,8,10]. Additionally, advances in imaging techniques and intraoperatve navigation tools facilitate preoperative assessment and safe surgical removal of localized lesions. The final repositioning of the mobilized bone, combined with the location of the incisions in natural folds, achieves favorable aesthetic results. Despite the aforementioned advantages, this technique may present a series of complications. Due to the technique itself and secondary to excessive mucoperiosteal detachment, the vascularization of the bone may be compromised. On the other hand, there is a possibility of secondary oronasal communication due to the osteotomy performed in the hard palate [10]. Other complications to consider include possible intraoperative bleeding from the internal maxillary artery, loss of function of the V2 andV3 branches, temporary or permanent damage to branches of the facial nerve (VII), postoperative pain, maxillary sinusitis, epiphora, and visible scars 8. In the presented case, a complete and safe resection of the described lesion was achieved, with minor sequelae resulting from the tumor affecting V2. The final aesthetic result was optimal (Figure 4).
Conclusion
In conclusion, facial translocation through pedicle maxillectomy is considered an excellent alternative in cases requiring extensive and complex resections of tumors located in the PPF. When endoscopic approach is not indicated or technically not available, this approach allows a great surgical control of neurovascular structures located in the PPF increasing the safety of the procedure.
References
- Ríos CF, Flores KS, Acosta TM, Carpio DJ, Quisiguiña KP, Serrano JE, Narváez MM. Tumores de Fosa Pterigopalatina: Tipos de abordajes quirúrgicos y complicaciones. Cambios rev. méd. 2021; 20(1): 53-59. DOI: https://doi.org/10.36015/cambios.v20.n1.2021.000.
- Kanatas A, Mücke T, Thomas, Houghton D, Mitchell D. Schwannomas of thehead and neck. Oncol Rev 2009; 3: 107-111. DOI:10.1007/s12156-009-0015-6.
- Rosique-López, L.; Rosique-Arias, M.; Sánchez-Celemin, F.J.: Schwannoma de la fosa pterigopalatina. Abordaje endoscópico. Neurocirugía. 2010; 21: 405-410.
- Hernández Altemir F. Transfacial access to the retromaxillary area. J Maxillofac Surg. 1986; 14(3): 165-70. doi: 10.1016/s0301-0503(86)80285-5. PMID: 3014030.
- Osguthorpe JD, Patel S. Craniofacial approaches to tumors of the anterior skull base. Otolaryngol Clin North Am. 2001; 34(6): 1123-42. ix. DOI: 10.1016/s0030-6665(05)70370-4. PMID: 11728937.
- Acero-Sanz J, Navarro-Vila C. Midfacial Translocation Approach. In: Cappabianca P, Iaconetta G, Califano L. (eds) Cranial, Craniofacial and Skull Base Surgery. Springer, Milano. https://doi.org/10.1007/978-88-470-1167-0_23. 2010.
- Califano L, Piombino P, Esposito F & Iaconetta G. Midfacial Approaches. In Cranial, Craniofacial and Skull Base Surgery (pp. 301-307). https://doi.org/10.1007/978-88-470-1167-0_22. 2010.
- Pampín Martínez MM, Dueso Delgado V, Cebrián Carretero JL, Alfonso Carillo C, Burgueño García M. Combined endoscopic and open approach for a salivary gland carcinoma at the pterygoid region. Revista Española de Cirugía Oral y Maxilofacial. 2021; 43(1): 40-43. Epub 19 de abril de 2021. https://dx.doi.org/10.20986/recom.2020.1123/2020.
- Hao SP, Pan WL, Chang CN, Hsu YS. The use of the facial translocationtechnique in the management of tumors of the paranasal sinuses and skull base. Otolaryngol Head Neck Surg. 2003; 128(4): 571-5. DOI: 10.1016/s0194-5998(03)00092-5. PMID: 12707663.
- Kalra GS, Midya M, Bedi M. Access to the Skull Base - Maxillary Swing Procedure - Long Term Analysis. Ann Maxillofac Surg. 2018; 8(1): 86-90. doi: 10.4103/ams.ams_5_18. PMID: 29963431; PMCID: PMC6018278.