
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
The diagnostic dilemma in ovarian ectopic pregnancy
Chun Phoy Cheng1*; Li Xinyi2
1Senior Resident, Department of Obstetrics & Gynaecology, KK Women’s & Children’s Hospital, 100 Bukit Timah Road, Singapore.
2Consultant, Department of Obstetrics & Gynaecology, KK Women’s & Children’s Hospital, 100 Bukit Timah Road, Singapore.
*Corresponding Author : Chun Phoy Cheng
Senior Resident, Department of Obstetrics and
Gynaecology, KK Women’s and Children’s Hospital
100 Bukit Timah Road, Singapore.
Email: Phoycheng.chun@mohh.com.sg
Received : Feb 21, 2024
Accepted : Mar 11, 2024
Published : Mar 18, 2024
Archived : www.jcimcr.org
Copyright : © Cheng CP (2024).
Abstract
Diagnosis of ovarian ectopic pregnancy (OEP) is challenging because of its rarity. We report a case of 30-year-old woman who presented with abdominal pain. Her pelvic ultrasound showed bilateral ovarian cysts and a right adnexal mass which was separated from the right ovary. OEP was diagnosed intraoperatively with histological confirmation. Diagnostic dilemma is expected, either via imaging or intraoperatively as OEP can mimic appearance of ovarian cysts and blood clots. Preoperatively, patients should be counselled adequately regarding the possible intraoperative findings and their treatments. Surgeons should have the technical abilities to perform ovarian ectopic excision or have minimally invasive surgery specialist available to perform the operation. In conclusion, identification of OEP remains a challenge. Therefore, high clinical suspicion and improved imaging skills are warranted.
Keywords: Ovarian ectopic pregnancy; Ovarian cysts.
Abbreviations: OEP: Ovarian Ectopic Pregnancy; ART: Assisted Reproductive Technique; IVF: In Vitro Fertilization; TVUS: Transvaginal Ultrasound; CLC: Corpus Luteum Cyst; MRI: Magnetic Resonance Imaging; CT: Computerized Tomography.
Citation: Cheng CP, Xinyi L. The diagnostic dilemma in ovarian ectopic pregnancy. J Clin Images Med Case Rep. 2024; 5(3): 2927.
Introduction
Diagnosis of ovarian ectopic pregnancy (OEP) is typically difficult because of its rarity and similar sonographic appearance to bleeding corpus luteum cyst, hemorrhagic cyst, and tubal ectopic pregnancy. Incidence of OEP is reported to be 0.5% to 1% of all ectopic pregnancies (EP), or 1 in 7000 – 14000 live births [1,2]. It is essential to make a correct diagnosis as OEP can be life-threatening in the event of rupture or bleeding, which may necessitate blood transfusion and emergency surgery. Risk factors for OEP are like any ectopic pregnancy. They include pelvic pathologies such as endometriosis and pelvic adhesions [3], previous intrauterine surgery, prior use of intrauterine device [4] and assisted reproductive techniques (ART) [5]. There are several theories to explain the pathophysiology of OEP. With pelvic pathologies such as endometriosis and pelvic adhesions, the egg released during ovulation process is trapped in the ruptured follicle and fail to implant in the womb [6]. Previous intrauterine surgery may modify the environment for intrauterine embryo implantation, while prior use of intrauterine device may affect tubal motility, leading to ovarian implantation. A study by Hallet JG et al. revealed that one in every nine EP among intrauterine devices users is an ovarian pregnancy [7]. In assisted reproductive techniques, the use of ovulation- stimulating drugs and large volume of medium injection into the uterus during embryo transfer with high injection pressure increases the uterine smooth muscle contractility and alter tubal motility. In addition, higher number of embryos transferred during each IVF cycle has been associated with higher incidence of OEP [8].
Case presentation
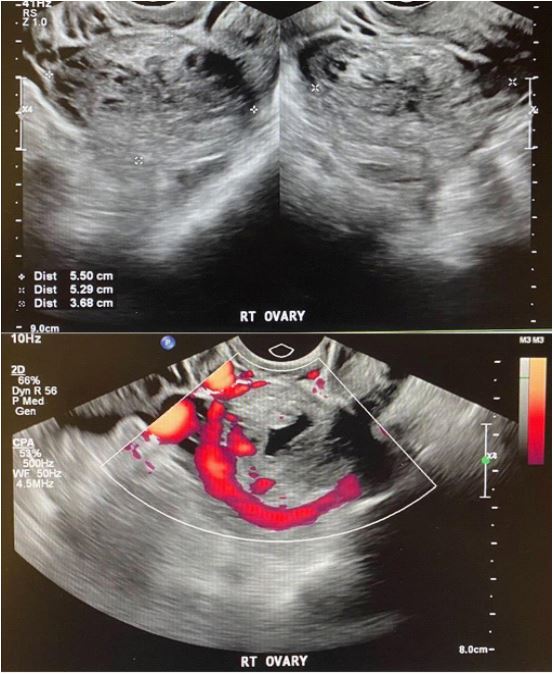
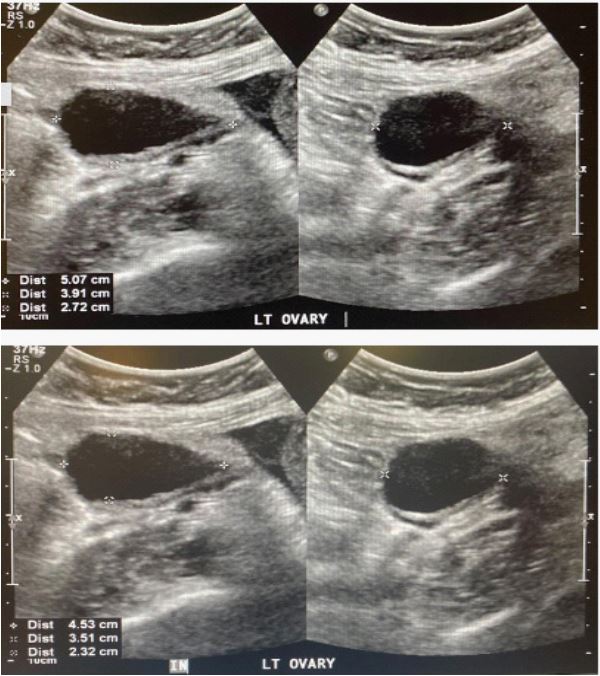
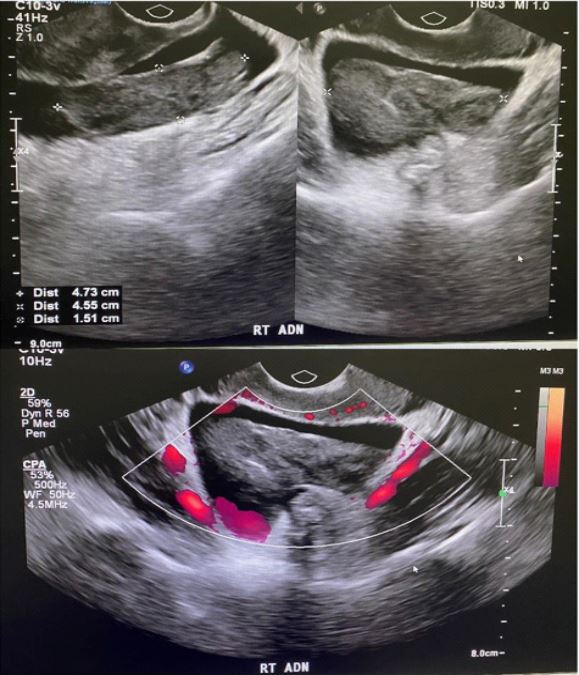
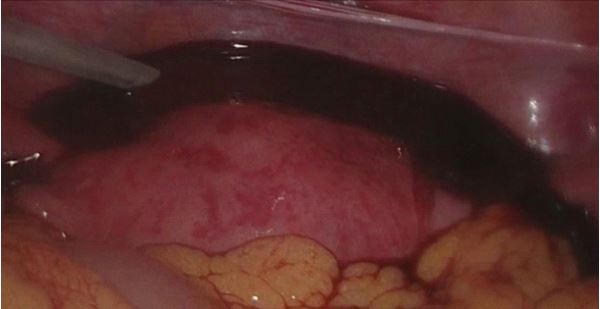
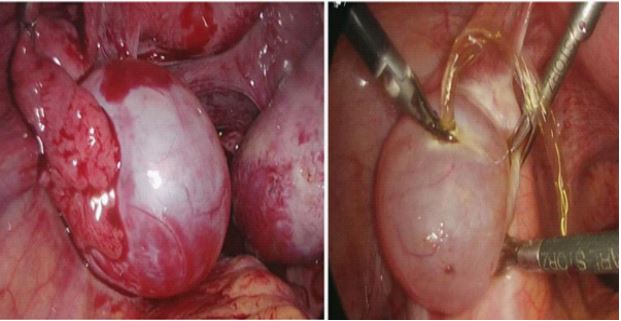
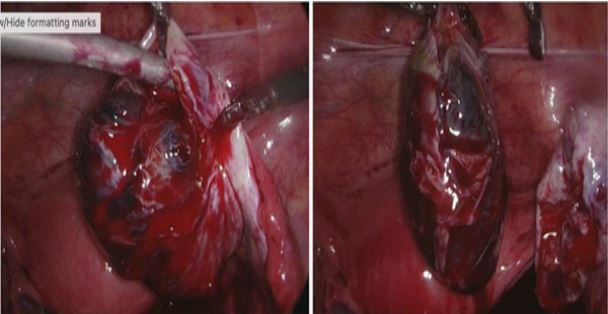
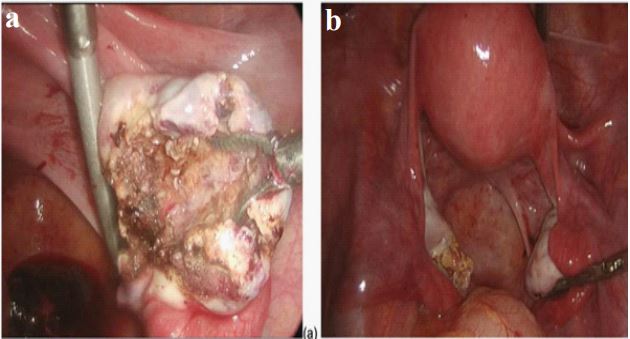
We report a case of OEP which was diagnosed intraoperatively. She was a woman in her 30s, gravida 4 para 2 who presented with persistent lower abdominal pain for 1 day, with pain score of 9/10. She had 2 previous full term normal vaginal delivery and 1 previous medical termination of pregnancy. This was a spontaneous unplanned pregnancy. Her menses were regular. She was 7+1 weeks amenorrheic on the day of consult. Her vitals were normal with temperature of 36.0 degree Celsius, blood pressure 105/68 mmHg, and heart rate 69 beats per minute. On examination, she was alert, her abdomen was soft, with tenderness over the lower abdominal area. There were no signs of acute abdomen. Speculum examination revealed a normal cervix with no per vaginal bleeding. Her BHCG level was 43392 IU/L, Hemoglobin 13.4 g/dL and blood group A+. Pelvic ultrasound showed endometrium thickness of 7mm, right ovary was normal with a corpus luteum within (Figure 1), left ovary with a 4.5x3.5x2.3 cm anechoic avascular cyst which may be functional (Figure 2). There was an ovoid heterogenous hypoechoic lesion in the right adnexal region separated from the ovary which appeared non-vascular, measuring 4.7x 4.6x1.5 cm (Figure 3), possible an ectopic pregnancy, with a differential of a large blood clot. There was moderate pelvic fluid containing low level echoes which may represent free blood from a ruptured EP. She was counselled for surgery in view of the above findings. Intraoperatively, her uterus was 6 weeks size, there was 450 mls of hemoperitoneum (Figure 4), a left functional cyst measuring 3 cm (Figure 5) and a right ruptured ovarian ectopic pregnancy measuring 5cm with active bleeding (Figure 6). Bilateral tubes, Pouch of Douglas and liver were normal (Figure 7). She underwent diagnostic laparoscopy, right ovarian ectopic excision, drainage of left ovarian cyst and evacuation of uterus. Repeated BHCG on the next day was 22432.6 IU/L. She was discharged well on post-operative day 1. Subsequent weekly BHCG levels down trended and her urine pregnancy test was negative a month later. Histology of right ovarian ectopic excision confirmed products of conception. She was started on combined oral contraceptive pills for pregnancy prevention.
Discussion/conclusion
The finding of an adnexal mass with empty uterus and normal fallopian tubes should always raise suspicion for an OEP. Transvaginal ultrasound (TVUS) is generally used as first line imaging for EP due to its convenience and relatively low cost. It is reported to have a sensitivity of 69–99% and specificity of 84– 99.9% for diagnosis of EP [9]. Yet, sonographic identification of OEP is often difficult because it can mimic appearance of ovarian cysts and blood clot. Study by Choi HJ et al. and Ciortea R et al. showed that a correct diagnosis of OEP by TVUS was only 18% [10] and intraoperatively was only 28% [3], respectively. Koroglu M et al. study showed that hemoperitoneum is associated with a positive predictive value of 86–93% in diagnosing EP and may be the sole finding on TVUS. In 15–35% of cases, an extrauterine mass may not be detected at ultrasound [11].
Unlike Spielberg’s diagnostic criteria which are observed intraoperatively, there is no established diagnostic criteria for OEP in TVUS. Sosa M et al. suggested that the presence of a hyperechoic ring in the outer half to one-third of the ovary should raise suspicion for an OEP [12]. Raziel et al., Levine et al., and Comstock et al. considered these as ultrasonographic diagnostic criteria for OEP – 1) thick-walled, echogenic rings with internal anechoic area within or on the surface of ovary, 2) presence of ovarian cortex, and 3) an increased ring echogenicity as compared to ovarian stroma [13-15]. A tubal ectopic pregnancy has a thinner wall compared to OEP, while a corpus luteum cyst (CLC) echogenicity is lesser when compared to ovarian stroma. The use of color doppler to demonstrate significant vascularity is unreliable as both ectopic ring and corpus luteum wall can display the “ring of fire” sign [16]. Similarly, the use of pulsed wave doppler is of limited value as there is no significant difference in peak systolic velocity measurement between OEP and CLC. A negative sliding organ sign may be useful to diagnose OEP in which the mass cannot be separated from ovarian tissue. Nonetheless, this sign can be falsely positive in cases of severe endometriosis or frozen pelvis.
With increasing number of ART, clinicians including surgeons, radiologists and radiographers should have a high clinical suspicion for OEP. In cases of inconclusive or non-specific sonographic findings, consideration should be given to perform an interval scan, to consult a second radiologist, or to transfer the patient to a tertiary center with relevant expertise for second opinion. What the mind does not think the eyes will not see. Alternative imaging such as magnetic resonance imaging (MRI) and computerized tomography (CT) have been studied as tools in OEP diagnosis. MRI scan has excellent tissue contrast, allowing accurate localization of abnormal implantation site [9]. It is quite sensitive to blood and can identify the hemorrhage phase [11]. On MRI, EP structure appears as a high-intensity mass containing distinct, low-intensity foci on T2-weighted imaging, which indicate bleeding; a CLC has a thick wall showing a slightly increased intensity on T1-weighted images and relatively low intensity on T2-weighted images [9]. Its purpose in OEP diagnosis is likely to be limited to very stable patients with diagnostic dilemma such as pregnancy of unknown location or in patients who do not consent to diagnostic laparoscopy. Not to mention, most patients may not be stable enough to await MRI due to its limited resources and cost. In contrast to MRI, CT scan is more easily available in most hospitals. However, the role of CT is mostly limited to identifying other causes of intraabdominal bleeding besides EP, and in localizing other sites of EP such as abdominal, hepatic, omental or retroperitoneal.
Laparoscopy is both diagnostic and therapeutic in OEP. Spielberg’s diagnostic criteria for an OEP consist of 4 findings: the fallopian tube on the affected side is normal, the ovary must be connected to the uterus by ovarian ligament, the fetal sac must occupy a place on the ovary and definite ovarian tissue must be demonstrated in some part of the sac. Unfortunately, Spielberg’s criteria are observed intraoperatively, and cannot be proven via sonography. When discussing diagnostic laparoscopy, patients should be counselled adequately about the possible intraoperative findings and their corresponding treatments, especially in cases where pre-operative imaging is not confidently diagnostic. They should be informed regarding needs for serial BHCG trend or scan to ensure complete resolution of pregnancy.
In the management of OEP, laparoscopy is the gold standard. Type of surgery depends on the size of ectopic – a wedge resection or excision of the ectopic for small lesions, and oophorectomy for larger lesions. Surgeons should have the technical abilities to perform ovarian ectopic excision or have minimally invasive surgery specialist available to operate should the need arise. Other treatments such as methotrexate injection can be considered in cases of unruptured OEP with low levels of serum BHCG.
References
- Bouab M, Touimi AB, Jalal M, Lamrissi A, Fichtali K, Bouhya S. Diagnosis and management of ectopic ovarian pregnancy: A rare case report. Int J. Surg. Case Rep. 2022; 91: 106742.
- Almahloul Z, Amro B, Nagshabandi Z, Alkiumi I, Hakim Z, Wattiez A, Tahlak M, Koninckx PR. Ovarian Pregnancy: 2 Case Reports and a Systematic Review. J. Clin.Med. 2023; 12: 1138. https:// doi.org/10.3390/jcm12031138.
- Ciortea R, Costin N, Chiroiu B, Mălutan A, Mocan R, Hudacsko A, Gaia A, Bucuri C, Mihu D. Ovarian pregnancy associated with pelvic adhesions. Clujul Med. 2013; 86(1): 77-80. Epub 2013 Feb 4. PMID: 26527922; PMCID: PMC4462474.
- Ghasemi Tehrani H, Hamoush Z, Ghasemi M, Hashemi L. Ovarian ectopic pregnancy: A rare case. Iran J Reprod Med. 2014; 12(4): 281-4. PMID: 24976824; PMCID: PMC4071634.
- Marcus SF, and Brinsden PR. Primary ovarian pregnancy after in vitro fertilization and embryo transfer: Report of seven cases. Fertil. Steril. 1993; 60: 167-169. doi:10.1016/s0015-0282(16)56057-9.
- Roy J, Sinha Babu A. Ovarian pregnancy: two case reports. Australas Med J. 2013; 6(8): 406-14. doi: 10.4066/AMJ.2013.1760. PMID: 24039634; PMCID: PMC3767028.
- Hallatt JG. Primary ovarian pregnancy: a report of twentyfive cases. Am J Obstet Gynecol. 1982; 143(1): 55-60. doi: 10.1016/0002-9378(82)90683-4. PMID: 7081312.
- Ren F, Liu G, Wang T, Li M and Guo Z. Unruptured ovarian ectopic pregnancy: Two case reports and literature review. Front. Physiol. 2022; 13: 1036365. doi: 10.3389/fphys.2022.1036365.
- Tamai K, Koyama T, Togashi K. MR features of ectopic pregnancy. Eur Radiol. 2007; 17(12): 3236-46. doi: 10.1007/s00330-007-0751-6. Epub 2007 Sep 20. PMID: 17882426.
- Choi HJ, Im KS, Jung HJ, Lim KT, Mok JE, Kwon YS. Clinical analysis of ovarian pregnancy: a report of 49 cases. Eur J Obstet Gynecol Reprod Biol. 2011; 158(1): 87-9. Doi: 10.1016/j.ejogrb.2011.04.015. 23. PMID: 21601978.
- Köroğlu M, Kayhan A, Soylu FN, Erol B, Schmid-Tannwald C, Gürses C, Karademir İ, Ernst R, Yousuf A, Oto A. MR imaging of ectopic pregnancy with an emphasis on unusual implantation sites. Jpn J Radiol. 2013; 31(2): 75-80. doi: 10.1007/s11604-012-0151-y. Epub 2012 Nov 7. PMID: 23132557.
- Sosa M, Brancazio S, Drummey A, Nguyen T, Toussaint T. Transvaginal Ultrasound Diagnosis of Ovarian Ectopic Pregnancy. Cureus. 2023; 15(1): e33536. doi: 10.7759/cureus.33536. PMID: 36779156; PMCID: PMC9907383.
- Raziel A, Schachter M, Mordechai E, Friedler S, Pansky M, Ron-El R. Ovarian pregnancy: a 12year experience of 19 cases in one institution. Eur J Obstet Gynecol Reprod Med. 2004; 114: 92-6.
- Levine D. Ectopic pregnancy. Radiology. 2007; 245(2): 385-97. doi:10.1148/radiol.2452061031. PMID: 17940301.
- Comstock K, Huston K, Lee W. The ultrasonographic appearance of ovarian ectopic pregnancies. Obstet Gynecol 2005; 105: 42-5.
- Kadau JV. Sonographic Detection of Ovarian Ectopic Pregnancy: A Case Study. Journal of Diagnostic Medical Sonography. 2016; 32(5): 299-303. doi:10.1177/8756479316663163.