
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 5
A rare case of severe Raynaud’s phenomenon
Harukazu Hirano*
Division of Occupational Medicine, Koyo Seikyo Clinic, Fukui Health Cooperative Association, Japan.
*Corresponding Author : Harukazu Hirano
Division of Occupational Medicine, Koyo Seikyo Clinic, Fukui Health Cooperative Association, Japan.
Email: koyo@asfu.jp
Received : Feb 23, 2024
Accepted : Mar 12, 2024
Published : Mar 19, 2024
Archived : www.jcimcr.org
Copyright : © Hirano H (2024).
Abstract
Raynaud’s phenomenon (RP) is episodic vasospasm of the peripheral blood vessels. RP secondary to connective tissue diseases, such as systemic sclerosis, is well known, but RP associated with vibrating tool users is often overlooked by clinicians. We report a clinical case of RP associated with hand-arm vibration syndrome in a 64-year-old man, which is an extremely rare case of severe RP involving the palms.
Keywords: Raynaud’s phenomenon; Hand-arm vibration syndrome; Finger blanching.
Abbreviations: RP: Raynaud’s phenomenon.
Citation: Hirano H. A rare case of severe Raynaud’s phenomenon. J Clin Images Med Case Rep. 2024; 5(3): 2928.
Description
A 64-year-old man noticed Raynaud’s phenomenon (RP) and numbness in both hands 17 years previously. He had cervical spinal stenosis three years ago, and his symptoms did not improve after surgery. and visited the clinic with photographs of RP (Figures 1 & 2). A physical examination revealed no scleroderma. Chest radiography did not reveal interstitial opacification. Laboratory tests showed no elevation of inflammatory markers, antinuclear antibodies, or rheumatoid factors. According to interviews regarding his work history, he had worked in forestry for 45 years and had used a chainsaw, a vibrating tool. RP was considered secondary, but the diagnosis of connective tissue diseases may be negative, and hand-arm vibration syndrome should be considered. Beraprost sodium tablets and alprostadil (intravenously, in winter) were administered as drug treatments. Treatments for cold hands, winter RP, and numbness were effective, but insufficient, as symptoms persisted for up to 15 years after diagnosis.

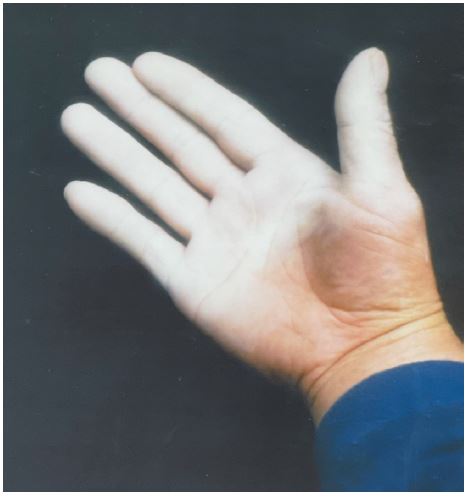
RP is a vasospastic disease characterized by an exaggerated vasoconstrictive response to cold and/or emotional stress, and is associated with significant pain and disability [1]. The classic color changes were white (ischemia), blue (deoxygenation), and red (reperfusion) [2]. RP usually appears on fingertips, and its boundaries are well recognized. However, RP rarely appears in the thumb [3]. To our knowledge, there have been no reports of severe RP affecting the palms, as in the present case. Even if RP is not as severe as in this case, patients with RP are often immediately referred to a rheumatologist without proper consideration of non-rheumatic diseases, including those caused by exposure to physical agents. In the clinical setting, determining social work history is crucial for patients with RP [4].
Declarations
Acknowledgments: I would like to thank the patient for allowing me to share this clinical image.The work was supported by the Fukui Rural Labor Union (Grant No. 202401).
Disclosure: The authors declare no potential conflict of interest.
References
- Maverakis E, Patel F, Kronenberg DG, et al. International consensus criteria for the diagnosis of Raynaud’s phenomenon. J Autoimmun. 2014; 48-49: 60-5.
- Ramahi A, Hughes M, Khanna D et al. Practical management of Raynaud’s phenomenon - a primer for practicing physicians. Curr OpinRheumatol. 2022; 34(4): 235-244.
- Poole CJM, Bovenzi M, Nilsson T et al.International consensus criteria for diagnosing and staging hand-arm vibration syndrome. Int Arch Occup Environ Health. 2019; 92(1): 117-127.
- Hirano H. Mottled Raynaud’s phenomenon and hand-arm vibration syndrome: followed up for 10 years. BMJ Case Rep. 2024; 17(1).