
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Non-traumatic gallbladder hemorrhage with shock in Asia: A case report
Chung Yang Tu*
Department of Chemical Biology, Ernest Mario School of Pharmacy, Rutgers, The State University of New Jersey, Piscataway, New Jersey, USA.
*Corresponding Author : Chung Yang Tu
Department of Chemical Biology, Ernest Mario School of Pharmacy, Rutgers, The State University of New Jersey, Piscataway, New
Jersey, USA.
Email: worktu0611@gmail.com
Received : Feb 03, 2024
Accepted : Mar 12, 2024
Published : Mar 19, 2024
Archived : www.jcimcr.org
Copyright : © Yang Tu C (2024).
Abstract
Gallbladder hemorrhage, rare due to trauma, iatrogenic factors, or conditions like liver/kidney dysfunction or cancer, presents with symptoms such as right upper abdominal pain and fever. In severe cases, gallbladder blood may enter the gastrointestinal tract, causing melena or hematemesis, necessitating surgical intervention. Delay can lead to life-threatening hemorrhagic shock. Diagnosing in the emergency room is challenging, with delayed recognition risking severe outcomes. Ultrasound is vital for diagnosis. A 64-year-old female presented with three days of epigastric pain and nausea, denying trauma, fever, respiratory or chest symptoms. Unstable vital signs were noted. Blood tests showed no abnormalities; ultrasound revealed a distended gallbladder without stones. Post-cholecystectomy confirmed acute hemorrhagic cholecystitis, highlighting ultrasound’s pivotal role. Gallbladder hematoma, rare with vague symptoms, poses diagnostic challenges linked to trauma, tumors, anticoagulant use, or liver/renal disease. Initial symptoms include right upper quadrant pain, tenderness, nausea, and vomiting, resembling cholecystitis. Persistent bleeding may result in dark or bloody stools. Laboratory tests may reveal abnormalities, but sensitivity is limited. Diagnosis is complex, delayed recognition in the emergency department can lead to severe shock and increased mortality. The literature review emphasizes the association with liver/kidney dysfunction and anticoagulant use, presenting symptoms akin to gallbladder inflammation and occasional gastrointestinal bleeding. Ultrasound is pivotal for diagnosis, showcasing features like uneven echoes and localized wall thickening. Treatment approaches vary, with some cases opting for deferred surgical intervention after conservative treatment. Non-traumatic gallbladder hematoma is linked to risk factors like liver/kidney diseases and chronic anticoagulant use. Gallbladder inflammation and gastrointestinal bleeding symptoms coexist, underscoring ultrasound’s crucial role. This study establishes early detection and diagnosis protocols for emergency room settings.
Keywords: Gallbladder hemorrhage; Shock, Ultrasound, Emergency
Citation: Yang Tu C.Non-traumatic gallbladder hemorrhage with shock in Asia: A case report. J Clin Images Med Case Rep. 2024; 5(3): 2929.
Introduction
Gallbladder hemorrhage is an uncommon condition that can be caused by trauma, iatrogenic factors, or underlying conditions like liver or kidney dysfunction, and cancer [1]. Symptoms may include right upper abdominal pain and fever. In severe cases, blood from the gallbladder can enter the gastrointestinal tract, resulting in symptoms such as melena (dark stools) or hematemesis (vomiting blood). Blood clots may also cause blockage and inflammation [2-4], requiring surgical intervention for effective management. Failure to promptly address this condition can lead to life-threatening hemorrhagic shock.
Case report
The 64-year-old woman had a history of depression and reflux esophagitis. Her medications included Llonazepam, gomelatine, Melitracen/Flupentixol, Lorazepam, Duloxetine, Propranolol, Estazolam, Lansoprazole, and Atorvastatin. She didn’t use anticoagulants. She experienced epigastric pain and nausea for three days without fever, chills, vomiting, or diarrhea. At resuscitation room vital signs showed a body temperature of 36°C, heart rate of 140 bpm, respiratory rate of 24/min, and blood pressure of 70/30 mmHg. A physical examination found mild tenderness in the right upper quadrant with a positive Murphy sign. There were no rebound pain or peritoneal signs. Lab results included Hemoglobin (Hb) at 8.4 g/dL, C-reactive protein (CRP) at 0.9 mg/L, white blood cell count (WBC) at 7900 μL, segmented neutrophils at 76.1%, total bilirubin at 0.4 mg/dL, lipase at 21 U/L, alanine transaminase (ALT) at 19 U/L, activated partial thromboplastin time (APTT) at 27.3 sec, and prothrombin time (PT) at 12 sec. Bedside sonography showed a distended and hyperechoic gallbladder without stones (Figure 1). Suspecting hemorrhagic cholecystitis with shock, a massive blood transfusion and immediate surgery were initiated. Preliminary suspicion of hemorrhagic cholecystitis, immediate administration of a large blood transfusion, and consultation with a general surgeon. During laparoscopic cholecystectomy, a distended gallbladder with a significant blood clot but no wall thickening or pigmented stones was observed. The cystic duct and artery were healthy (Figure 2). After surgery and hospitalization, her symptoms improved. She had a favorable prognosis and was discharged. Follow-up bile culture showed no growth, and the gallbladder pathology indicated vascular congestion with blood colt. However, the gallbladder cytologic sample lacked sufficient cells for proper evaluation.
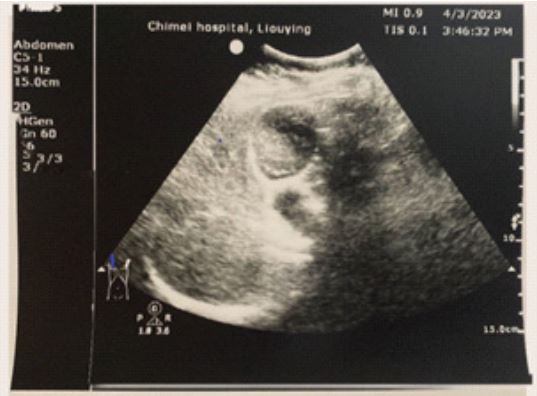

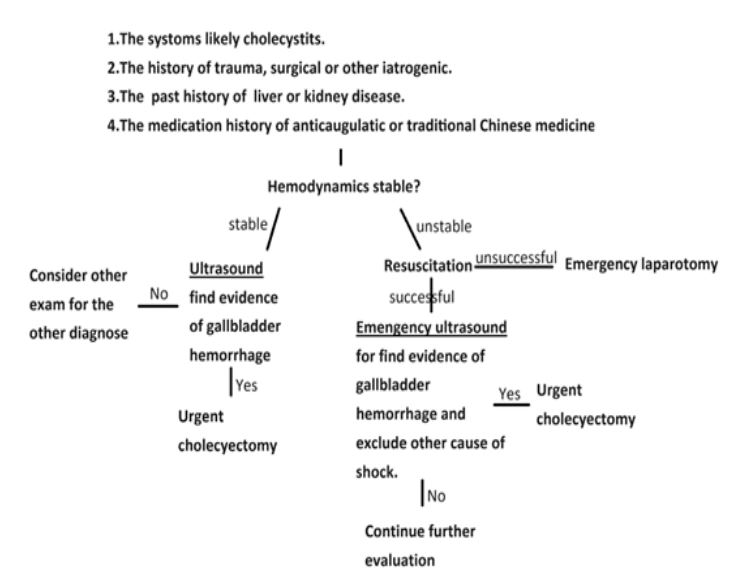
Table 1: 1980-2023 Gallbladder hematoma case reports.
| Reference | Age/Gender | Past history | Chief complaint | Anti -coagulite Drugs | Treatment | |
|---|---|---|---|---|---|---|
| 1. |
Berland et al. [5], 1980 |
56/ male | Alcohol liver disease | Upper abdominal pain | N |
1. Laparotomy 2. Open Cholecystectomy |
| 2. |
Brady et al[6], 1985 |
79/ male |
Breast carcinoma s/p radical mastectomy |
Fever, Epigastric, RUQ pain |
N | 1. Open cholecystectomy |
| 3. |
Stempel et al[7], 1993 |
78/ male | HTN, Renal insufficiency | RUQ pain |
Heparin during Abdominal aorta aneurysm repair |
1. Cholecystostomy drainage |
| 4. |
Nishiwaki et al[8], 1999 |
58/ male | Alcohol abuse | RUQ pain, chest pain | N |
1. Laparotomy 2. Open cholecystectomy |
| 5. |
Gremmels et al[9], 2004 |
66/ male | COPD | RUQ pain | N |
1. Laparotomy 2. Open cholecystectomy |
| 6. |
Kim et al[10], 2007 |
55/ male |
Liver cirrhosis, Gallbladder stone |
Upper abdominal pain | N |
1. Cholecystostomy drainage |
| 7. |
Pandya et al [11], 2008 |
85/ female |
DIverticulitis, Left
common vein thrombosis |
Diffuse abdominal pain |
Aspirin Warfarin |
1. Conservative with IV antibiotics |
| 8. |
Morris et al [12], 2008 |
91/ female | CHF |
Nausea, vomiting, Right abdominal pain |
N | 1. Open cholecystectomy |
| 9. |
Lai et al[13], 2009 |
81/ male |
ESRD regular
hemodialysis, COPD |
RUQ pain | Heparin for dialysis |
1. Conservative with IV antibiotics, elective laparo- scopic cholecystectomy |
| 10. |
Chen et al[14] 2010 |
75/ female | HTN, CHF |
Chest tightness, cold sweating |
Hepirin |
1. Laparoscopic cholecystectomy |
| 11. |
Parekh et al [15], 2010 |
60/ male |
Renal cell carcinoma, Prostate carcinoma, HTN, hypothyroidism |
Abdominal pain, nausea, fever |
N |
ERCP + Laparoscopic cholecystectomy |
| 50/ male | HCV |
1. Right abdominal pain after meal. 2. Blunt trauma several days ago |
N |
ERCP + Laparoscopic cholecystectomy |
||
| 12. |
Jung et al[16], 2011 |
55/ male | Not mentioned | RUQ pain | N |
Laparoscopic cholecystectomy |
| 13. |
García et al [17], 2011 |
24/ female | SLE | RUQ pain | N |
1. Laparoscopic open cholecystectomy 2. Iintra-operative cholangiography |
| 14. |
Kwon et al [18], 2012 |
75/ male | Af, HTN | RUQ pain | Warfarin |
Laparoscopic cholecystectomy |
| 15. | Choi [19], 2012 |
36/ male |
Myocardial infarction s/p CABG |
RUQ pain | Aspirin Clopidogrel |
Laparoscopic cholecystectomy |
| 16. |
Taniguchi et al[20], 2013 |
48/ male |
Alcohol liver cirrhosis, ESRD |
RUQ pain | Hepirin |
Laparotomy Open cholecystectomy |
| 17. |
Seok et al[21], 2013 |
84/ male | HTN | Epigastric pain | N |
Laparoscopic cholecystectomy |
| 18. |
Onozawa et al[22], 2014 |
58/ female | Not mentioned |
Abdominal and back pain |
N |
Laparoscopic cholecystectomy |
| 19. |
Aljiffry et al [23], 2014 |
57/ male |
Primary sclerosing cholangitis, liver cirrhosis |
RUQ and epigastric pain | N |
1.Cystic artery embolization 2.Open cholecystectomy |
| 20. | Cho et al[24] 2015 |
61/ male | HTN, DM, Angina, Af | Dyspnea, dizziness | Warfarin |
Cholecystostomy drainage |
| 21. |
Calvo Espino et al[25], 2016 |
59/ male | Liver cirrhosis | Abdominal pain | N |
1.Laparotomy 2. Open cholecystectomy |
| 22. |
Tsai et al[26], 2016 |
80/ male |
DM, Liver cirrhosis, CKD, GB stone |
Tarry stool passage |
N |
1.Cholecystostomy 2. Elective laparoscopic cho- lecystectomy |
| 23. |
Yoshida et al [27], 2017 |
73/ male |
Ischemia heart disease
s/p CABG |
Epigastric pain | Aspirin Warfarin |
Laparoscopic cholecystectomy |
| 24. |
Oshiro et al [28], 2017 |
61/ female |
SLE, Antiphospholipid syndrome |
Abdominal pain and melena |
Warfarin |
1. Conservative with IV antibiotics 2. Elective laparoscopic cholecystectomy |
| 25. |
Shishida M et al[29], 2017 |
79/ male | DM, ESRD | RUQ pain | Hepirin | 1.ERCP 2.ENBD |
| 26. |
Kinnear et al [30], 2017 |
74/ male |
Small bowel obstruction, Hernia Hyperparathyrodism HTN |
RUQ pain | Apixaban |
1. Laparotomy 2. Open cholecystectomy |
| 28. |
Choi et al [31], 2017 |
65/ male | Non |
Blunt trauma of RUQ abdomen |
N |
1.Laparotomy 2. Open cholecystectomy |
| 29. |
Berndtson et al[32], 2017 |
75/ female | Myeloma |
Epigastric pain, nausea, vomiting |
N | Open cholecystectomy |
| 30. |
Liefman et al [33], 2018 |
73/ female |
DM, HTN, Myocardial infarction |
RUQ pain Melena |
Aspirin Clopidogrel |
1. Conservative with IV antibiotics 2. Elective laparoscopic cholecystectomy |
| 31. |
Ng et al [34], 2018 |
68/ female | DM, Depression |
Abdominal pain, nausea, vomiting |
N | Open cholecystectomy |
| 32. |
San Juan López C et al [35],2019 |
55/ male | Liver cirrhosis | RUQ pain | N |
Laparoscopic cholecystectomy |
| 33. |
Honda et al [36], 2019 |
71/ male | Polyangiitis | RUQ pain | N |
Laparoscopic cholecystectomy |
| 34. |
Itagaki et al [37], 2019 |
86/ female |
HTN, Embolic cerebral infarction |
Melena | Edoxaban |
1. Conservative with IV antibiotics 2. Elective laparoscopic cholecystectomy |
| 35. |
Reens et al [38], 2019 |
76/ male |
HTN, Hyperlipidemia, DM, Af, CAD |
RUQ pain | Warfarin | Cholecystostomy |
| 36. |
Tarazi et al [39], 2019 |
87 / male |
COPD, Ischemia heart dis- ease, Pulmonary embolism |
Sharp right iliac fossa pain | Warfarin | 1. Cholecystostomy |
| 65/ female |
Hypothyroidism, Af, Poly- cystic kidney disease, Ovarian cystectomy |
Nausea, upper abdominal pain |
Warfarin |
1. Conservative with IV antibiotics |
||
| 92/ female |
Renal carcinoma, Diverticular disease, |
Intermittent sharp pain
of RUQ, epigastric |
N | 1. Cholecystostomy | ||
| 37. |
Kishimoto et al[40], 2020 |
96/female | Cholecycarcinoma | Epigastric pain | N |
Laparoscopic cholecystectomy |
| 38. |
Gomes et al [41], 2020 |
87/ male |
Dementia, Cholelithiasis, CVA |
RUQ pain and fever | Aspirin | Open cholecystectomy |
| 39. |
Yam et al[42], 2020 |
51/ female |
ESRD, Parathyroidectomy, Hemithyroidectomy |
Abdominal pain | N |
1. Cystic artery
embolization, 2. Cholecystostomy 3. Open cholecystectomy |
| 40. |
Azam et al [43], 2021 |
55/ male |
HTN, DM, Renal transplant, Deep veins thrombosis |
RUQ pain | Apixaban | Cholecystectomy |
| 41. | Leaning [44], 2021 |
73/ male |
Pulmonary embolism, COPD, CVA, HTN, CKD |
RUQ pain, nausea, vomiting |
Apixaban |
Laparoscopic Cholecystectomy |
| 42. |
Chen X et al [45], 2021 |
63/ female | N | RUQ pain, Icteric sclera | N |
1. ERCP and ENBD, 2. Cholecystectomy |
| 43. |
Nguyen D et al[46], 2021 |
74/ male | Atrial fibrillation |
Abdominal pain, vomiting, nausea |
Warfarin |
1. Cystic artery
embolization 2. Cholecystectomy |
| 44. |
Pickell Z et al[47], 2021 |
67/ male | CAD, Af, CHF, CVA, CKD |
Substernal and subxiphoid pain with nause . |
tPA | Cholecystectomy |
| 45. |
Valenti MR et al[48], 2022 |
76/ male |
Osteoporosis, Parkinsonism. |
Abdominal pain, constipation |
N | Open cholecystectomy |
Discussion
Gallbladder hematoma is a rare condition with vague symptoms, making it challenging to diagnose. It is often associated with trauma, tumors, anticoagulant use, or liver/renal disease. Common symptoms include pain in the right upper quadrant (RUQ), tenderness, nausea, and vomiting, which may be confused with cholecystitis initially. Persistent bleeding can cause dark or bloody stools. Laboratory tests may show abnormalities, but their sensitivity is limited. Diagnosing gallbladder hematoma can be complex, and a delayed diagnosis in the emergency department can lead to severe shock and increased mortality. A literature review of 48 cases is summarized in Table 1.
The literature review identified 48 cases of non-traumatic gallbladder bleeding, indeed highlighting the correlation with liver or kidney dysfunction and the use of anticoagulant medications. Symptoms resemble those of gallbladder inflammation, with one case report additionally noting gastrointestinal bleeding. Ultrasound is crucial for diagnosis, revealing distinctive features such as uneven echoes and localized wall thickening. Treatment approaches vary, with some cases opting for deferred surgical intervention after conservative treatment. However, surgical intervention remains a common outcome. In summary, non-traumatic gallbladder hematoma is primarily associated with risk factors such as liver or kidney diseases and chronic use of anticoagulant medications. In cases where symptoms of gallbladder inflammation and gastrointestinal bleeding coexist, timely ultrasound diagnosis is crucial to prevent fatal hemorrhagic shock. This study establishes early detection and diagnosis protocols (Figure 3) as a reference for future emergency room diagnoses of this condition.
References
- Derici H, Kara C, Bozdag AD, Nazli O, Tansug T, Akca E. Diagnosis and treatment of gallbladder perforation. World J Gastroenterol. 2006; 12(48): 7832-7836.
- Choi YS. Gallbladder hemorrhage mimicking acute cholecystitis in a patient under antiplatelet therapy. Gastroenterol. 2012; 50: 285-287.
- Gremmels J M, Kruskal J B, Parangi S & Kane R A. Hemorrhagic Cholecystitis Simulating Gallbladder Carcinoma. Journal of Ultrasound in Medicine. 2004; 23(7): 993-5.
- Jung YM, Son BK, Ahn SB, Kim DH, Kim EK. Intramural gallbladder hematoma mimicking gallbladder neoplasm in a 55-year-old male patient. J Korean Surg Soc. 2011; 81: 216-220.
- Berland, L. L., Doust, B. D., & Foley, W. D. Acute Hemorrhage into the Gallbladder Diagnosed by Computed Tomography and Ultrasonography. Journal of Computer Assisted Tomography. 1980; 4(2): 260-2.
- Brady, E., & Welch, J. P. (1985). Acute hemorrhagic cholecystitis causing hemobilia and colonic necrosis. Diseases of the Colon & Rectum. 1985; 28(3): 185-7.
- Stempel L R & Vogelzang RL. Hemorrhagic Cholecystitis with Hemobilia: Treatment with Percutaneous Cholecystostomy and Transcatheter Urokinase. Journal of Vascular and Interventional Radiology. 1993; 4(3): 377-380.
- Nishiwaki M, Ashida H, Nishimura T, Kimura M, Yagyu R, Nishioka A, Yamamura T. Posttraumatic intra-gallbladder hemorrhage in a patient with liver cirrhosis. Journal of Gastroenterology. 1999; 34(2): 282-285.
- Gremmels JM, Kruskal JB, Parangi S, Kane RA. Hemorrhagic cholecystitis simulating gallbladder carcinoma. J Ultrasound Med. 2004; 23: 993-995.
- Kim YC, Park MS, Chung YE, Lim JS, Kim MJ, Kim KW. Gallstone spillage caused by spontaneously perforated hemorrhagic cholecystitis. World J Gastroenterol. 2007; 13: 5525-5526.
- Pandya R & O’Malley C. Hemorrhagic cholecystitis as a complication of anticoagulant therapy: role of CT in its diagnosis. Abdominal Imaging. 2008; 33: 652-653.
- Morris DS, Porterfield JR, Sawyer MD. Hemorrhagic cholecystitis in an elderly patient taking aspirin and cilostazol. Case Rep Gastroenterol. 2008; 2: 203-207.
- Lai YC, Tarng DC. Hemorrhagic acalculous cholecystitis: an unusual location of uremic bleeding. J Chin Med Assoc. 2009; 72: 484-487.
- Chen YY, Yi CH, Chen CL, Huang SC, Hsu YH. Hemorrhagic cholecystitis after anticoagulation therapy. Am J Med Sci. 2010; 340: 338-339.
- Parekh J, Corvera CU. Hemorrhagic cholecystitis. Arch Surg. 2010; 145: 202-204.
- Jung YM, Son BK, Ahn SB, Kim DH, Kim EK. Intramural gallbladder hematoma mimicking gallbladder neoplasm in a 55-year-old male patient. J Korean Surg Soc. 2011; 81:2 16-220.
- García Pérez R, Ruiz de Angulo D, López Poveda MJ, Febrero Sánchez B, Navas Carrillo D, Parrilla Paricio P. Hemorrhagic cholecystitis and hemobilia: two infrequent complications of systemic lupus erythematosus. Rev Esp Enferm Dig. 2011; 103: 431-433.
- Kwon JN. Hemorrhagic cholecystitis: report of a case. Korean J Hepatobiliary Pancreat Surg. 2012; 16: 120-122.
- Choi YS. Gallbladder hemorrhage mimicking acute cholecystitis in a patient under antiplatelet therapy. Z Gastroenterol. 2012; 50: 285-287.
- Taniguchi M, Kanai S, Kitamura M, Nakamura I, Nakamura T, Shimomatsuya T. A case of gallbladder hemorrhage with intraperitoneal bleeding. J Japan Surg Associa.2013; 74: 503-507.
- Seok DK, Ki SS, Wang JH, Moon ES, Lee TU. Hemorrhagic cholecystitis presenting as obstructive jaundice. Korean J Intern Med. 2013; 28: 384-385.
- Onozawa H, Saito M, Yoshida S, Sakuma T, Matsuzaki M, Katagata N, Watanabe F, Yamaguchi Y, Takenoshita S, Nomizu T. Multiple metastatic malignant melanoma presenting intraluminal gallbladder bleeding. Int Surg. 2014; 99: 600-605.
- Aljiffry M M, Almulhim A N, Jamal M H & Hassanain M M. Acute cholecystitis presenting with massive intra-abdominal haemorrhage. Journal of Surgical Case Reports.2014(4);rju019–rju019.
- Cho SH, Lee HY, Kim HS. Anticoagulant Therapy-Induced Gallbladder Hemorrhage after Cardiac Valve Replacement. Korean J Thorac Cardiovasc Surg. 2015; 48: 432-434.
- Calvo Espino P, Chaparro Cabezas M D, Jiménez Cubedo E, Lucena de la Poza J L & Sánchez Turrión, V. Colecistitis hemorrágica perforada. Cirugía Española. 2016; 94(2): 35-6.
- Tsai JL & Tsai SF. Gallbladder bleeding-related severe gastrointestinal bleeding and shock in a case with end-stage renal disease. Medicine. 2016; 95(23): 3870.
- Yoshida S, Yokoyama K, Nishida T, Ikuta H. A Case of Gallbladder Hemorrhage Occurred during Anticoagulation Therapy. J Japan Surg Associa. 2017; 78: 359-364.
- Oshiro Y, Tsukamoto S, Owada Y, Takahashi K, Oda T, Sakamoto N, Ohkohchi N. Hemorrhagic Cholecystitis During Anticoagulant Therapy in a Patient With Systemic Lupus Erythematosus and Antiphospholipid Syndrome Undergoing Elective Laparoscopic Cholecystectomy. Int Surg. 2017; 105: 1-3.
- Shishida M, Ikeda M, Karakuchi N, Ono K, Tsukiyama N, Shimomura M, Oishi K, Miyamoto K, Toyota K, Sadamoto S, Takahashi T. Hemorrhagic Cholecystitis in a Patient on Maintenance Dialysis. Case Rep Gastroenterol. 2017; 11: 488-493.
- Kinnear N, Hennessey D B& Thomas R. Haemorrhagic cholecystitis in a newly anticoagulated patient. BMJ Case Reports. 2017; 12: 2017:bcr2016214617.
- Choi KK, Lee MA, Ma DS, Lee GJ, Yu BC, Lee JN. A Hemorrhagic Cholecystitis in a Penetrating Hepatic Injury Trauma Image Proced. 2017; 2(1): 15-16. Published online: May 31, 2017.
- Berndtson A E, Hamel M G, Costantini T W & Coimbra R. Acalculous Perforated Hemorrhagic Emphysematous Cholecystitis Caused by Clostridium perfringens in a Patient with Myeloma Taking Daratumumab. Surgical Infections Case Reports. 2017; 2(1): 1-4.
- Liefman D, Wullschleger M. Hemorrhagic cholecystitis: a rare cause of presentation with upper gastrointestinal bleeding. Int Ann Med. 2018; 2: 5.
- Ng Z Q, Pradhan S, Cheah K & Wijesuriya R. Haemorrhagic cholecystitis: a rare entity not to be forgotten. BMJ Case Reports. 2018; 2018: 226469.
- San Juan López C, Lázaro Sáez M, Hernández Martínez Á, López González J, Vega Sáenz JL. Bleeding from gallbladder varices in a patient with an unknown liver cirrhosis. An exceptional entity. Rev Esp Enferm Dig. 2019; 111: 723-724.
- Honda F, Tsuboi H, Toko H, Terasaki T, Terasaki M, Shimizu M, Sumida T. Contrast Enhanced Computed Tomography Revealed Gallbladder Hemorrhage Due to Active Vasculitis in a Patient With Microscopic Polyangiitis. JCR: Journal of Clinical Rheumatology. 2018; 25(6): 84-85.
- Itagaki H, Katuhiko S. Gallbladder hemorrhage during orally administered edoxaban therapy: a case report. J Med Case Rep. 2019; 13: 383.
- Reens D, Podgorski B. Hemorrhagic Cholecystitis: A Case of Expedited Diagnosis by Point-of-Care Ultrasound in the Emergency Department. J Emerg Med. 2019; 57: 74-76.
- Tarazi M, Tomalieh FT, Sweeney A, Sumner D, Abdulaal Y. Literature review and case series of haemorrhagic cholecystitis. J Surg Case Rep. 2019; 2019: 360.
- Kishimoto T, Hashimoto Y, Imamura H, Shigetsu K, Murotani M, Yoneda N, Kidogami S, Mokutani Y, Hirose H, Yoshioka S, Endo S, Tamura S, Sasaki Y. [A Case of Rapidly Progressive Gallbladder Cancer Presented with Gallbladder Hemorrhage. Gan To Kagaku Ryoho. 2020; 47: 2361-2363.
- Gomes AF, Fernandes S, Martins J, Coutinho J. Carcinoma of the gallbladder presenting as haemorrhagic cholecystitis. BMJ Case Rep. 2020; 13.
- Yam MKH, Sim SW, Tam KY, Li YL. A 51-year-old female presenting with shock due to hemorrhagic cholecystitis. Radiol Case Rep. 2020; 15: 2547-2549.
- Azam M U, Ibrahim M A, Perry I, Ellison S B, Barrett A & Vega K J. It’s the Bloody Gallbladder! Spontaneous Gallbladder Hemorrhage Following Factor Xa Inhibition. Journal of the National Medical Association. 2021; 113(3): 252-254.
- Leaning M. Surgical case report—acalculous hemorrhagic cholecystitis. Journal of Surgical Case Reports, 2021; (3).
- Chen X, Yu L. A haemorrhagic cholecystitis presenting as obstructive jaundice. Hepatobiliary Surg Nutr. 2021; 10: 299-300.
- Nguyen D, Goodwin JS, Bhowmik N, Boiteau G, Potts J. Acute Hemorrhagic Cholecystitis with Large Hemoperitoneum: Treatment with Microcoil Embolization and Subsequent Cholecystectomy. J Radiol Case Rep. 2021; 15: 25-34.
- Pickell, Z., Raghavendran, K., Westerhoff, M., & Williams, A. M. Acute hemorrhagic cholecystitis with gallbladder rupture and massive intra-abdominal hemorrhage. Autopsy Case Reports. 2021; 11: 2020232.
- Valenti MR, Cavallaro A, Di Vita M, Zanghi A, Longo Trischitta G, Cappellani A. Gallbladder hemorrhage–An uncommon surgical emergency: A case report. World J Clin Cases 2022; 10(27): 9734-9742.